Article Text

Abstract
Objectives Microbial threats pose a growing concern worldwide. This paper reports the analysis of Iran’s policy process against microbial threats.
Design This is a qualitative study.
Participants We interviewed 16 purposefully identified key informants selected through snowball sampling.
Setting Through the lens of stages heuristic framework, we analysed the interviews by using thematic content analysis. We used MAXQDA V.2020 software for data analysis, identified key themes and subthemes and discussed our findings to validate the results.
Results We extracted four main categories in accordance with the stages heuristic domains. Through content analysis of the agenda-setting process, we identified three main themes: magnitude of the problem, actors’ power and priorities. Participants highlighted the significant impact of microbial threats, the influence of powerful stakeholders and the underprioritisation of infectious diseases based on perceived urgency and resources. In the process of policy formulation, we explored three main themes, related to governance, coherence and integration of policies and barriers to effective policy formulation. Governance issues included transparency, engagement with stakeholders, conflict of interest and use of evidence, while coherence and integration of policies focused on insufficient coherence and integration of plans as well as temporary and defensive policymaking. Barriers to effective policy formulation encompassed delay in policymaking, policy gap in response to public needs, weakness in policy feasibility, risk assessment and management. For policy implementation, we extracted governance and coordination, and health system capacity. Effective implementation of policies was hindered by fragmented governance, inadequate communication and accountability and systemic barriers, while health system capacity was limited in terms of infrastructure and human resources. Finally, content analysis of monitoring and evaluation (M&E) resulted in identification of two main themes: discrepancies in M&E and barriers to effective M&E. The discrepancies in M&E varied, with some programmes having regular evaluations and others lacking compliance with international standards. Barriers to effective M&E included inadequate data access, limited information-sharing and inefficiencies in the M&E system.
Conclusions Iran needs to prioritise infectious diseases, invest in preventive measures, improve governance and coordination, strengthen health system capacity, enhance M&E and so on, to combat microbial threats effectively. Learning from successful experiences of other countries can help Iran develop more effective strategies to address microbial threats and strengthen global public health in the country.
- Qualitative Research
- Infectious Diseases
- Health policy
Data availability statement
Data are available upon reasonable request. The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study:
Credibility: discussed findings with participants to strengthen the credibility of the research.
Purposeful selection: key informants were selected for their relevant expertise, ensuring depth and insight.
Structured framework: employed the stages of heuristic framework to systematically analyse policy stages.
Sectoral limitations: the study participants were exclusively from the human health sector, excluding perspectives from the animal and environmental health sectors, which might limit the comprehensiveness of the findings and does not fully encompass the One Health approach.
Contextual generalisability: the qualitative nature of the study and specific context of Iran may limit the generalisability of the findings to other settings.
Introduction
Microbial threats, including neglected tropical diseases, emerging infectious diseases (EID) and re-emerging infectious diseases (RID), antimicrobial resistance (AMR), foodborne and water-borne infections and so on, pose a global health security challenge. They cause high morbidity and mortality and require urgent policy action worldwide.1 2 In 2019 about 4.95 million deaths linked to bacterial AMR globally, with 1.27 million directly attributed to AMR.3 This figure may reach 10 million deaths annually by 2050.3 According to the WHO, 60% of EID are zoonotic, with 75% originating from animals,4 highlighting the need for multisectoral collaboration against microbial threats.2 5 This underscores the importance of the ‘One Health’ approach, which integrates human, animal and environmental health sectors to effectively address these threats.
Factors such as population growth, technology, international travel and trade, globalisation, urbanisation and climate change facilitate the spread of infectious diseases, increasing the complexity and diversity of microbial threats from bacterial to viral and the emergence of EID, RID, bioterrorism and AMR.6 7 The threats can cross borders, create epidemics and pandemics and disrupt social and economic systems. The world has faced many outbreaks since 2000, such as Severe Acute Respiratory Syndrome (SARS), H1N1 Influenza, Cholera, Middle East Respiratory Syndrome (MERS), Ebola Virus Disease, Zika Virus Disease, Yellow Fever and the Novel Coronavirus Disease (COVID-19).8 9 These challenges require effective policies and interventions to mitigate the risks and impacts on human health and society.10
Agenda setting is usually the first stage in the policy process, where problems are identified and prioritised for governmental action. It involves recognising issues that requires attention and mobilising resources to address them. This stage is crucial as it determines which issues will receive governmental focus and resources. Factors influencing agenda setting include focusing events, that is, outbreaks or pandemics, which highlight the urgency of addressing specific health threats.11 Understanding agenda setting helps in analysing how microbial threats are prioritised and addressed within the policy frameworks.
Health system overview
Healthcare services in Iran are delivered through three main routes: the public–governmental system, the private sector and non-governmental organisations. In line with upstream policies, the Ministry of Health and Medical Education (MoHME) is the primary body responsible for health system governance, the provision of healthcare services, medical education, policymaking and regulation. Iran’s healthcare system has made significant strides in improving public health, particularly through the establishment of an extensive Primary Healthcare (PHC) network. This network has been instrumental in reducing child and maternal mortality rates and increasing life expectancy.12
Iran has historically faced high burdens of infectious diseases on its health system.13 The improvements in public health and sanitation, healthcare accessibility and vaccination coverage have significantly reduced the infectious diseases burden during the past four decades in Iran.14 The top five powerful stakeholders involved in health policy process to combat microbial threats in Iran include the President Office and the Cabinet, the Minister of Health and Medical Education, the Parliament, the National COVID-19 Committee (NCC) and the Plan and Budget Organisation (PBO).15 The Iranian Communicable Diseases Control (CDC), affiliated with the MoHME, has been playing a pivotal role in managing infectious diseases in Iran, that is, in controlling outbreaks and implementing public health policies. Historically, the Iranian CDC has been involved in significant public health initiatives, that is, the eradication of smallpox and control of cholera and plague outbreaks.16–18 Nevertheless, the country still faces infectious diseases, such as respiratory infections, tuberculosis, avian influenza, MERS and COVID-19.19 20 The government of Iran has developed policies against microbial threats through prevention, early detection and recovery planning. To enrich existing literature on policy process for addressing microbial threats, this paper reports our qualitative analysis of the policy process in the face of microbial threats in Iran. Understanding the policy process, we hope to identify different policy approaches and develop policy recommendations for improving the effectiveness and sustainability of microbial threat policies, in Iran and beyond.
Methods
Research design
This is an exploratory qualitative case study. Using a deductive approach and through the lens of stages heuristic framework, we examined the policymaking process against microbial threats in Iran. The study adopts an interpretivist paradigm, which is a well-suited approach for exploring the complexities of policy processes and the experiences and perspectives of key informants in Iran.21
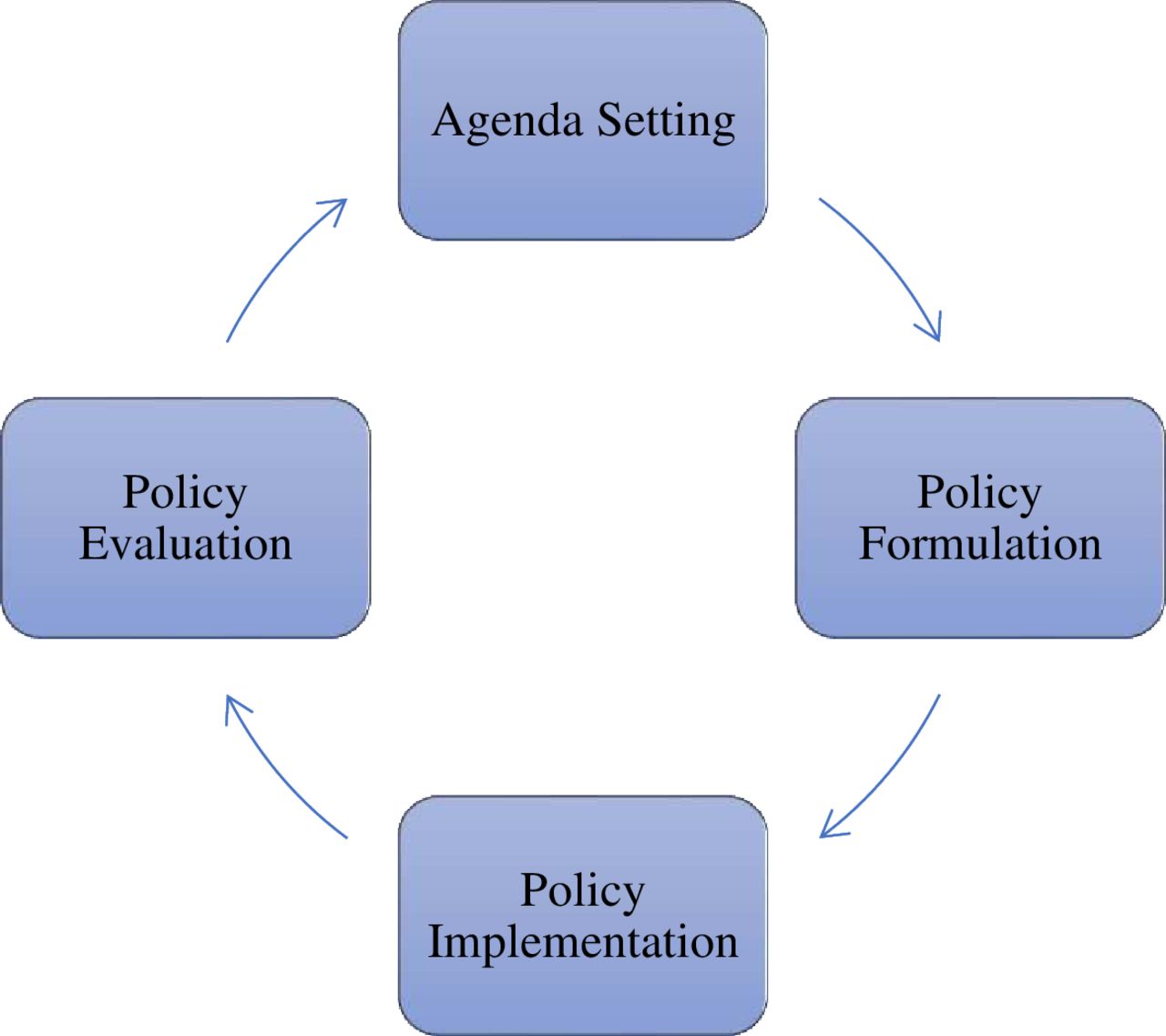
The stages heuristic framework, introduced by Harold Lasswell in the 1950s, is a widely recognised framework in public policy analysis. This model breaks down the complex policymaking process into manageable stages, making it easier to analyse and understand, including:
Agenda setting: prioritising the issue and bringing it to the attention of policymakers.
Policy formulation: developing possible solutions and selecting the most appropriate one.
Policy implementation: putting the approved policy into action through government agencies and other actors.
Policy evaluation: assessing the effectiveness of the policy and making necessary adjustments (figure 1).

The stages heuristic framework.
This model is particularly useful because it simplifies the policy process into distinct phases, allowing for a clearer analysis of each stage.22
The underlying epistemology guiding this study is interpretivism, which shaped both the study design and the analysis. This framework facilitated an in-depth exploration of the participants’ perspectives on policy processes related to microbial threats in Iran, resulting in a nuanced understanding of the subject matter.
Data collection
We conducted semistructured, in-depth face-to-face interviews with key informants using a generic interview guide (online supplemental file 1), developed by the research team based on an extensive literature review19 23–32 and in accordance with the study objectives. The initial draft of the interview guide was iteratively refined throughout the study, based on ongoing feedback from interviewees and insights gained during the interviews. Before each interview, we sent the interview guide, the information sheet and the informed consent form to the interviewees. We recorded and transcribed all interviews verbatim. Each interview lasted between 45 and 90 min.
Supplemental material
Sampling
We selected our interviewees purposefully with elements of snowball sampling with maximum diversity, targeting individuals with relevant expertise. Interviewees were relevant key informants, including, policymakers, government officials, healthcare professionals, public health officials, academics and researchers, who had knowledge and experience in microbial threats or related policies, participated in the formulation or were knowledgeable about the studied policies in Iran. Initially, we compiled a list of potential interviewees based on their positions and contributions within the field. They were contacted via email, where we provided an overview of the study, its objectives and the importance of their insights. The interviewer also coordinated the date, time and location of the interviews with each interviewee. Follow-up communication was also conducted through phone calls, messages or additional emails to maximise response rates. A total of 25 individuals were contacted for participation in the study. Out of these, 9 individuals declined to participate. The reasons for rejection varied, from time constraints and other commitments as barriers to participation. Finally, we interviewed 16 people from March to December 2022 (table 1). All participants were from the human health sector. This focus was chosen to gain in-depth insights into the human health policy processes against microbial threats in Iran. Most interviews were conducted in the interviewees’ offices or via an online platform such as Skype. Prior to commencing the interview process, the interviewer (first author: AR) introduced herself and provided a comprehensive explanation of the study’s purpose and the confidentiality of the data obtained from participants. Informed consent was then obtained verbally. Participants were also assured of their right to withdraw from the study at any stage and without any explanation. With the interviewees’ verbal permission, the interviews were digitally recorded. We aimed to gather subjective information about the participants’ experiences and opinions related to the research objectives by establishing effective communication and interaction and through guiding the conversation towards relevant topics. Additionally, we took notes during the interviews to capture important details.
Participants characteristics* (Tehran, Iran, 2022)
Interviews were conducted until data saturation was achieved, ensuring that no new themes or insights were emerging from the data. As the interviews progressed and a consistent set of themes emerged—particularly concerning policy processes related to microbial threats—we determined that additional interviews were unlikely to yield substantially different insights, thus confirming data saturation. To bolster the reliability of our observations regarding data saturation, AR sought feedback from the research team, with a range of personal attributes and professional qualifications and expertise in public health policy and qualitative research methodologies. With a focus on improving policy processes and understanding participants’ experiences throughout the research process, we tried to ensure thoroughness and validity. We reviewed preliminary findings and themes after a portion of the interviews had been completed. After each interview, AR asked the interviewee to introduce other experts in the field, whom we approached for possible interview.
AR, had a background in health policy and qualitative research. The interviewee maintained detailed field notes throughout the interview process, which included reflections on the context of each interview, non-verbal cues observed during the discussions and initial impressions of the themes emerging from the conversations. The field notes were invaluable in complementing the audio recordings and transcriptions, aiding in the analysis by providing contextual depth and enhancing the overall interpretation of the data.
As interpretivist researchers, we maintained reflexivity throughout the study, being aware of our own positionality and its possible influence on data collection and interpretation. Regular self-reflection ensured that we remained cognisant of biases and assumptions that could affect the research outcomes.
Data analysis
The first author initiated the coding process of the interview data. To ensure rigour and validity in the analysis and reduce potential bias, AR engaged in a process of peer review with AT, an established qualitative researcher, who independently coded a subset of the interviews. We then compared our codes and discussed any discrepancies to reach a consensus on the coding framework. This collaborative approach ensured that different perspectives were incorporated into the analysis, thereby strengthening the credibility of the findings. We applied a deductive approach using the stages heuristic framework to extract and analyse data. Using thematic content analysis, we identified key themes and subthemes and interpreted the findings. The team discussed data interpretation multiple times to improve accuracy. We used the MAXQDA software V.2020 for data management.33
Member checking
To ensure the accuracy and relevance of the identified themes and strengthen the results’ credibility, we employed member checking. This process involved sharing the preliminary findings with a subset of the study participants to verify the accuracy of the data and the interpretations. Participants were asked to review the themes and provide feedback on whether they accurately reflected their experiences and perspectives. This feedback was then incorporated into the final analysis to ensure that the themes were representative and credible. This method served as a form of triangulation to strengthen the study credibility.
Results
The findings are categorised into agenda-setting, policy formulation, implementation and monitoring and evaluation (M&E) using the stages heuristic framework.
Agenda-setting
Content analysis of Iran’s policy process on microbial threats identified three themes and eight subthemes for agenda-setting (table 2).
Content analysis of agenda-setting to combat microbial threats in Iran (Tehran, Iran, 2022)
Magnitude of the problem
Participants highlighted that recent outbreaks, that is, COVID-19, have shown the devastating impact of microbial threats on public health, economy, security, global trade and sustainability. They urge further research to find cost-effective and evidence-based interventions to convince policymakers about microbial threats’ political priorities.
Throughout time, especially in the last hundred years, the importance of health security in general and microbial threats in particular has become clear. …. But I think that, at least, in the last ten years, the role and importance of preparing for biological and microbial threats is not well understood in our country. COVID-19 showed that we did not have the necessary preparedness. (P9, S. manager)
Actors’ power
Interviewees emphasised the importance of actors’ power in Iran’s policymaking process against microbial threats. Public, media and civil society organisations’ demand for action influenced politicians’ response more effectively:
Public demand is crucial, so microbial threat has to become the first demand and concern of people towards changing our policies accordingly. (P3, M. manager)
Participants noted that inadequate political will and commitment to address microbial threats has delayed effective policy implementation. They advocate for politicians to prioritise microbial threats, increase funding and develop appropriate policies and programmes:
In the era of COVID-19, the need to establish a CDC [Centers for Disease Control and Prevention] has become more prominent, but the necessary tools or the serious willingness of the system for a fundamental change have not been provided. (P5, S. policymaker)
Interviewees also pointed out the structural deficiencies and inadequate coordination within the MoHME, which they identified as a key actor regarding microbial threats and health security:
The existing structure of the MoHME and its governance really needs fundamental change. The heavy, stiff and inflexible body of the MoHME prevents any reforms. (P5, S. policymaker)
Participants described Iran’s health policymaking as fragmented among parallel organisations, causing duplication, contradictory policies, inefficiencies, confusion and inadequate response to health challenges, for example, microbial threats. They mentioned some of these parallel organisations: Supreme Council of Health and Food Safety (SCHFS), Crisis Management Organisation (CMO), Passive Defence Organisation (PDO), Pasteur Institute, Rapid response team to diagnose and manage disease outbreaks, National Vaccination Committee, National scientific/policy committees and NCC:
One of the challenges is structural. Look, we have the SCHFS, the MoHME, CDC, PDO, CMO, etc., … but none of them takes serious action when a crisis happens. (P15, M. manager)
Finally, interviewees discussed the authority, power and capacity of the centre responsible for managing communicable diseases in the country. Some experts praised the centre’s ability to respond to microbial threats, while others argued its limited power, hence strengthening the CDC is necessary for effective microbial threat management:
Now, they prepare the main material of decision-making and bring it to the NCC. In the beginning, maybe they had fewer authority; but this is not the case anymore. (P1, S. manager)
Unfortunately, we do not have an independent and established CDC at the moment. … During COVID-19, the lack of a comprehensive CDC was highlighted. (P5, S. policymaker)
Priorities
Participants highlighted the policymakers’ considerations before setting the agenda for addressing microbial threats in Iran.
Participants identified the underprioritisation of infectious diseases by policymakers in their agenda-setting against microbial threats in Iran:
Infectious diseases are no longer the country’s first concern…. Consequently, we had a significant increase in all infectious diseases during the COVID-19 period. (P3, M. manager)
Participants noted that Iran prioritises curative measures over health promotion and prevention measures, potentially delaying response to microbial threats after they emerge rather than implementing proactive measures:
Regarding COVID-19, I think that more investment and attention was paid to the field of treatment, and perhaps it has weakened the PHC a bit. (P4, M. manager)
Policy formulation
Analysis of Iran’s microbial threat policymaking process identified three themes and 10 subthemes in policy formulation category (table 3).
Content analysis of policy formulation to combat microbial threats in Iran (Tehran, Iran, 2022)
Governance
Within the theme of governance, we identified four subthemes: transparency, stakeholder engagement, conflict of interest and use of evidence.
Participants highlighted insufficient transparency of policymakers, noting the lack of openness and disclosure in the policymaking process. They emphasised that transparency is crucial for enhancing trust in society, as insufficient transparency causes uncertainty among stakeholders and decreases trust in policymakers, potentially reducing overall policy credibility:
Even for introducing a new vaccine, it is behind closed doors. If we make the right decision, is it behind closed doors. … When there is transparency, I cannot simply exercise my own interests. … A situation which we are actually deprived of it. (P11, Academic member)
Participants emphasised the importance of involving relevant stakeholders in the policy formulation, noting that insufficient participation of stakeholders in Iran led to inefficiency and ineffectiveness of policies:
Perhaps one of the most important factors that makes policies not to be successful in practice is that, in the last several years and decades, we could not make policies that involve all stakeholders… (P3, M. manager)
Participants emphasised the importance of an independent policymaking process to prevent vested interests’ influence, noting that dual practice, revolving doors, corruptive administrative structures and conflict of interest mismanagement contributed to ineffective policymaking process addressing microbial threats in the country.
Most policymakers are public servants with significant private interest, so they are not actually seeking to establish a strong, sustainable and coherent surveillance system. (P2, S. policymaker)
Participants also pointed to the extent to which policymakers use evidence in their decision-making process. They noted that evidence-informed policymaking ensures that policies are supported by data and evidence to achieve better results. However, they revealed that there is inconsistent and sometimes insufficient evidence in microbial threat policy formulation:
Of course, in all our planning, we mostly used international guidelines and instructions published by international organizations such as the [United States] CDC and WHO…, we also got technical assistance from some countries. This means that we follow their policies in some cases … (P1, S. manager)
… Let me say very clearly that until now we have not defined any policy in accordance with scientific principles that can be implemented in microbial threats. (P9, S. manager)
Coherence and integration of policies
Participants noted weak coherence and integration in Iran’s microbial threat policy formulation, highlighting a lack of a clear structure and prior plan for addressing these threats. They also identified insufficient coherence and integration of plans, which may highlight challenges in creating interconnected and coherent microbial threat policies. They suggested that the policies may be created in isolation or without considering integration, resulting a fragmented policy approach.
I see most of the problems at the beginning of the COVID-19 pandemic, which if you remember, there was a lot of inconsistency and there was confusion in that period, we didn't know what to do. (P1, S. manager)
They also noted that while temporary and defensive policymaking addresses immediate challenges and has led to immediate improvements, it raises concerns about long-term strategic planning for addressing microbial threats in the country.
Our response to COVID-19 seems to be solving our temporary problems; not all of them will be useful for our future. For example, we had a very small laboratory structure in diagnosis, COVID-19 helped us to upgrade this structure to a stronger network structure … Our laboratory network reached a quantitative and qualitative development during COVID-19, but this was not a futuristic policymaking. (P3, M. manager)
Barriers to effective policy formulation
Participants identified several barriers to effective policy formulation against microbial threats in Iran, including delays in policymaking, policy gap in response to public needs, weakness in the feasibility of policies and weakness in risk assessment and management.
Participants noted that delay in policymaking challenges prompt response to microbial threat. They identified a time lag in policy formulation, which could threaten the effectiveness of policies to tackle microbial threats:
We were usually late in many of our decisions, both in starting the restrictions, and in removing the restrictions. (P10, Academic Member)
Some participants emphasised that to formulate more efficient policies, policymaker must consider the needs of different groups in the society. They criticised policymakers’ lack of awareness about population needs and inadequate knowledge on addressing challenges, highlighting a ‘policy gap in response to public needs’:
My interest [as a policymaker] is that I want to start what I am familiar with. I'm not looking for what the public need might be. Because I'm not literate of it at all, I don't know what to do in this case. (P2, S. policymaker)
Several interviewees highlighted the weakness in policy feasibility, noting the need to measure the possibility of effective implementation of policies in practice. They indicated that the feasibility of policies against microbial threats in Iran was rarely examined prior to implementation:
We also have policies that are not well designed and thought out. For example, I will design a plan without considering the collective wisdom, … and then I will see that the bureaucrats cannot implement it. (P12, M. manager)
Some experts identified weakness in risk assessment and management is another barrier to formulate effective policies to tackle microbial threats in Iran, which might compromise their effectiveness:
In my opinion, we do not have the literacy of preparedness and risk reduction. We do not know risk assessment at all. … We could not use the data for risk assessment and risk management and risk reduction. (P13, S. manager)
Policy implementation
In this category, we identified two themes and five sub-themes (table 4).
Content analysis of policy implementation to combat microbial threats in Iran (Tehran, Iran, 2022)
Governance and coordination
The interviewees highlighted intersectoral collaboration as a significant issue, noting insufficient inter and intrasectoral collaboration and coordination among stakeholders (within the MoHME or between other sectors and the MoHME) during the policy implementation process. They indicated that the lack of collaboration among stakeholders can hinder policy implementation efficiency and reduce their effectiveness:
To some extent, this probably goes back to our societal characteristics and the behavior of our managers, and the fact that the inter-sectoral and intra-sectoral cooperation in our country has not been realized and is not performed as it should be. …. The health system is also weak in coordinating with other sectors. (P10, Academic Member)
Participants emphasised communication and accountability, noting inadequate accountability of policymakers, insufficient transparency in information sharing and distrust among stakeholders, which they believed might result in the policy implementation gap:
Unfortunately, not only do we [policymakers] not work to create trust, but actually we destroyed trust as much as we could. We presented false statistics, published news and then immediately denied that news, …. No one asked us why, even we were encouraged to some extent. (P11, Academic Member)
Some stakeholders identified systemic barriers refers to some embedded challenges in the society, which might hinder policy implementation and reduce effectiveness. They categorised these barriers into socioeconomic situation, the role of certain stakeholders in preventing policy implementation, insufficient implementation guarantee and administrative bureaucracies:
On the other hand, there are some stakeholders who do not allow a plan to go forward. Many of these stakeholders are also experts, but they are so strong and influential that they may stop the country or national program. (P7, Academic Member/ Healthcare Professional)
Health system capacity
Interviewees emphasised the strong health system with good infrastructure and the PHC network as vital facilitators to address the microbial threats in Iran. Nevertheless, they believed that the PHC network potential and the existing information technology platform were underutilised in addressing microbial threats:
In the past, we did not face such a heavy crisis that challenged our health system. …, but we did not see much failure in this path. Of course, the reason was not having a plan, but it was because of having a strong health system with good infrastructure. (P6, S. policymaker)
Our interviewees identified two main issues within the human resources subtheme. First, they noted that the insufficient and improper distribution of quality human resources, leading to low number of skilled professionals in the right places to effectively address the threat. Second, they highlighted the fatigue and exhaustion of human resources, referring to overworking and struggling professionals to keep up with implementing policies against the threats. Together, these two issues illustrate the human resources challenges against microbial threats in Iran.
In the past several years, we have been facing severe problems such as lack of human resources, especially in the areas that are supposed to perform duties in the field of tackling diseases. (P10, Academic Member)
Monitoring and evaluation
We identified two themes and six subthemes in the M&E of policies against microbial threats in Iran (table 5).
Content analysis of monitoring and evaluation of the policies to combat microbial threats in Iran (Tehran, Iran, 2022)
Discrepancies in monitoring and evaluation
Some interviewees noted several discrepancies in the M&E of policies to tackle microbial threats in Iran. These discrepancies were particularly evident across different types of policies and programmes. They indicated that some programmes, like those funded internationally, had M&E regularly performed and reported. For instance, programmes supported by organisations such as the Global Fund required consistent updating of guidelines and systematic evaluations. This led to a more structured and reliable M&E framework within these internationally funded initiatives. In contrast, for other plans, including international health regulations commitment, the country does not comply with the joint external evaluation (JEE) as a level of M&E. The lack of adequate M&E mechanisms to ensure adherence to these regulations was highlighted as a critical issue. Participants noted that while some international commitments were met, others were neglected, resulting in varied effectiveness of M&E practices. This inconsistency posed significant challenges in ensuring comprehensive M&E of microbial threats.
The fact is that in the case of three diseases, including malaria, HIV, and tuberculosis, for which we used the Global Fund [GFATM] budget for years, …, we were obliged to update our instructions periodically and perform regular M&E [systematic data collection, analysis, and reporting] programs. (P3, M. manager)
At the diagnostic and therapeutic level, there was a disparity in data collection and evaluation. While certain diseases had robust data management systems due to international support, other areas lacked comprehensive diagnostic and therapeutic data. This inconsistency affected the overall ability to monitor and respond to microbial threats effectively.
These systems are diffused. They work in parallel. Their information is not precise. The systems are not connected, the information is not used in time, there is no access to the data. (P10, Academic Member)
Barriers to effective monitoring and evaluation
Participants outlined several barriers to M&E against microbial threats in Iran, including inadequate access to data and information, limited information-sharing among sectors and inefficiencies of the M&E system. They highlighted the importance of addressing these challenges to track and measure policy effectiveness and ensure success in addressing microbial threats in Iran. These barriers restricted policymakers’ ability to conduct thorough evaluations and develop informed responses to microbial threats.
The next point was related to the M&E system based on the reporting and registration system. Our M&E system is not efficient enough … We gave up everything regarding the M&E. (P2, S. policymaker)
Discussion
Microbial threats were once a major cause of human mortality. Advancements in technology, healthcare, public health and lifestyle changes have reduced infectious disease burdens, while non-communicable diseases have become the main threats to human health.7 34 Infectious diseases require global policies against microbial threats.2 Iran, like other nations, has tackled this threat despite economic pressures from international sanctions.35 Nevertheless, Iran has been tackling the threat through a controversial process.
Short summary of main findings
Our research highlights that in Iran, the agenda-setting process for infectious disease policy is significantly influenced by the magnitude of the problem, the power of various actors and shifting national priorities. We found that underprioritisation of infectious diseases and fragmented governance present major barriers to effective implementation. These findings suggest an urgent need for a unified response strategy and a shift towards preventive measures.
Comparison with other studies
Our research found that problem magnitude, actor’s power and priorities are crucial factors in the agenda-setting process in Iran. Other studies have similarly shown their significance in shaping national and international policies for infectious diseases.36–38 A comparative analysis of the MERS outbreak policies in South Korea and Saudi Arabia revealed that varying levels of actor’s power and priorities led to distinct policy outcomes.37 In Saudi Arabia, insufficient political leadership and fragmented organisations hindered preventive measures, resulting in high cases and fatalities. Conversely, South Korea’s strong political commitment and collaborative efforts led to successful outbreak containment.37
Iran’s fragmented organisational structure is comparable to Brazil’s, which created the National Health Surveillance Agency (Anvisa) in 1999, a single regulatory agency for health products.38 Similarly, Thailand, a major tourist destination, has also implemented a centralised infectious disease control system to address increased risks of infectious disease threats. This system focuses on universal healthcare access, preventive measures and intersectoral collaboration.39 By examining these examples, we can better understand the importance of organisational coherence in effectively addressing microbial threats, highlighting the need for Iran to enhance its policy processes in a similar fashion.
Our findings revealed that underprioritisation of infectious diseases and a focus on curative measures are major barriers to combating microbial threats in Iran. Underprioritisation may be due to factors like poor awareness, ineffective monitoring and surveillance systems and limited resources.40 This suggests that Iran’s measures against microbial threats may not adequately address the risks of infectious diseases. The focus on curative measures also implies a reactive approach, attributed to resource constraints, limited early detection capacity and inadequate political will to invest in prevention.41 42
Our study showed that governance, coherence and integration and barriers to effective policy formulation, affect this stage in Iran. Regarding governance, our findings are consistent with another study that identified challenges with transparency, stakeholder engagement and the use of evidence in policymaking in Iran.43 Both studies emphasise the importance of scientific evidence to inform policy formulation for more effective measures against microbial threats. Insufficient transparency in the policy process in our study aligns with another study on AMR control in Iran,27 which identified inadequate transparency as the main challenge to stewardship in Iran. The insufficient openness and disclosure in decision-making can reduce trust in policymakers, affecting policy credibility and effectiveness against microbial threats. Transparency and conflict of interest management could enhance the success of Iran health system in combating microbial threats. In terms of coherence and integration, our study identified temporary and defensive policymaking with insufficient unity as a challenge, indicating that policies were not always designed with long-term goals in mind. In line with our study, Finland’s JEE in 2017 found ‘limited and fragmented’ policies in infectious diseases.44 45 Nevertheless, Finland’s approach to infectious diseases has improved, and the country is now skilful in pandemic preparedness.45 Finland achieved this by establishing a robust national infectious disease control system, enhancing coordination between various health authorities and investing in public health infrastructure. These changes have significantly bolstered Finland’s capacity to respond to infectious disease threats.46 In contrast, South Korea has a well-coordinated national infectious disease surveillance system, integrating policies across sectors.47 Understanding these specific improvements can offer valuable insights for Iran’s situation.
While the barriers to effective policy formulation in Iran include delayed policymaking, policy gaps in response to public needs and weaknesses in risk assessment and management, similar challenges have been observed in the USA, particularly during the COVID-19 pandemic. The fragmented health data collection and communication in the USA exemplify how systemic weaknesses can hinder timely and effective responses to public health crises.48 This comparison highlights how both countries struggle with systemic issues in policy formulation and implementation.
Moreover, our findings revealed that effective policy implementation in Iran requires investment in governance and coordination, as well as health system capacity. Other studies emphasised the importance of coordination between the MoHME and other sectors such as environmental health, agriculture, veterinary services and education in infectious disease policy implementation.12 18 27 43 The European Observatory on Health Systems and Policies emphasised the importance of governance strategies in enhancing coordination to build resilient health systems.49 A report on Ebola preparedness and response plans in West Africa also found that the lack of governance and coordination was an implementation challenge to manage outbreaks.50 A robust and coordinated surveillance system was recommended to address the readiness and response capacity gaps.50 While our study focused on participants from the human health sector, the findings highlight the need for a broader ‘One Health’ approach. Integrating perspectives from the animal health and environmental sectors could enhance the effectiveness of policies against microbial threats. The One Health approach, which emphasises multisectoral collaboration, is crucial for addressing zoonotic diseases and ensuring comprehensive preparedness and response strategies.
In terms of ‘communication and accountability’, like ours, other studies emphasised the importance of increasing trust among public and other stakeholders. The intentional destruction of trust by policymakers, as highlighted by presenting false statistics and then denying them, stems from a complex interplay of political, social and bureaucratic factors in the current study. This approach may have been driven by a desire to maintain control over public perception, avoid panic or manage political fallout. Moreover, in some cases, misinformation can be a tactic used to buy time while more effective strategies are developed. However, this ultimately leads to a breakdown in trust and can undermine the credibility and effectiveness of public health efforts. Addressing these underlying motivations can provide a more comprehensive understanding of the challenges faced in policy formulation and implementation.51 In line with our findings, another study advocated for the Iranian policymakers to prioritise public trust to ensure maximum public compliance.43 Similarly, in Canada, during the SARS outbreak, a lack of coordination, coherent communication and accountability hindered the response to the outbreak.52 This aligns with our results, which highlight that inadequate transparency and stakeholders’ engagement have impeded the effectiveness of policies against microbial threats in Iran. These parallels suggest that enhancing trust, coordination and communication are universal strategies crucial for improving policy responses to microbial threats.
Participants mentioned a strong health system with proper infrastructure and PHC network in Iran is vital in tackling microbial threats. However, some argue that the PHC network and information technology were underutilised to manage microbial threats, particularly COVID-19, in Iran. Our findings support another study that highlighted the neglected potential of PHC network to fight COVID-19 in Iran,43 while WHO guidance emphasises strengthening PHC services to address COVID-19 effectively.53
Regarding the ‘human resources’, to strengthen health system resiliency during crises, we suggest utilising compensation mechanisms like retired staff, final year students and task shifting in the supply and distribution of human resources. Similarly, another study on human resources for health (HRH) challenges in Iran identified issues like insufficient unified governance and comprehensive planning, procurement and recruitment, maldistribution, weak retention and motivation of the HRH, their burnout and workload increase, laws formulation and implementation weaknesses, unbalanced geographical distribution of HRH and so on.54
Finally, Iran’s M&E approach is unclear and varies across different international plans and policies. In certain plans, Iran has displayed commitment to regular M&E activities, which include systematic data collection, analysis and reporting. However, this commitment is often neglected in other plans, such as the IHR. A review of the COVID-19 surveillance system in 13 African countries found varying levels of M&E, both between and within countries. The study indicated M&E challenges, including poor data management, impede timely outbreak detection and response.55 The study found barriers to effective M&E, including restricted data access for policymakers, limited information-sharing between public and private sectors and inefficiencies in the M&E system. Another study also identified these challenges as barrier to evidence-based policymaking in Iran.43 In terms of AMR, better surveillance systems and data collection are needed to support M&E efforts.27 By contrast, in response to the MERS outbreak, South Korea and Canada have implemented effective tracking and tracing systems. South Korea has a centralised control system using real-time data-sharing,56 while Canada has a robust surveillance system that tracks and informs policymakers on infectious diseases.57
Policy implications
This study underscores the need for Iran to prioritise infectious diseases through proactive measures and enhanced governance. Adopting a One Health approach, which includes perspectives from human, animal and environmental health sectors, is crucial for comprehensive policy responses. Addressing infrastructural and workforce limitations, improving transparency and strengthening M&E systems are also essential. These steps, along with learning from international best practices, can significantly enhance Iran’s capability to combat microbial threats, ultimately contributing to global public health efforts.
Policy recommendation
Our study revealed some key policy recommendation for addressing microbial threats in Iran, which are presented in figure 2.

{kind=link}
{kind=link}
Key policy recommendation for addressing microbial threats in Iran. MoHME, Ministry of Health and Medical Education.
Study limitations
This study has several limitations that need to be acknowledged. First, the study participants were exclusively from the human health sector, excluding perspectives from the animal and environmental health sectors. This limitation might affect the comprehensiveness of the findings, as it does not fully encompass the One Health approach, which is critical for addressing zoonotic diseases and other microbial threats.
Additionally, the qualitative nature and specific context of Iran may limit the generalisability of the findings to other settings. The unique sociopolitical and economic conditions in Iran might not be directly applicable to other countries, thereby affecting the transferability of the results.
Furthermore, there is a potential for response bias. Key informants might have provided socially desirable responses or withheld critical information due to their positions or relationships with other stakeholders, potentially impacting the depth and accuracy of the data collected
Future directions
Further research is required to incorporate diverse perspectives from the animal and environmental health sectors, ensuring a more comprehensive One Health approach to tackling microbial threats. This would provide a holistic understanding of the interconnectedness of human, animal and environmental health.
Additionally, conducting similar qualitative studies in different geographical and sociopolitical contexts could help determine the generalisability of the findings and uncover unique challenges and strategies relevant to other regions. Comparative analyses between Iran and other countries could also offer valuable insights into global policy processes against microbial threats.
Finally, employing mixed methods that combine qualitative insights with quantitative data could further validate the findings and provide a more robust evidence base. This approach would help mitigate potential biases inherent in qualitative research.
Conclusions
This study represents a significant contribution to the understanding of policy processes against microbial threats in Iran. Unlike many other studies that focus solely on the outcomes of policy decisions, this research delves into the ‘how’ and ‘why’ behind these decisions, offering a more holistic view of the policy landscape. It offers a comprehensive analysis through the stages heuristic framework, providing valuable insights into the complexities of policymaking in the face of such threats. While Iran has made some progress tackling the infectious diseases, significant gaps still remained, requiring a comprehensive, long-term and multisectoral approach involving collaboration among all stakeholders, including the government, private sector and civil society. This requires more resources allocation, efficient surveillance systems, consistent political will to prioritise infectious diseases and a shift from curative to preventive measures. Good governance, including transparency, accountability, conflict of interest management and effective communication among stakeholders is essential, we advocate, for policy success. Addressing these policies is crucial for a more effective response to microbial threats in Iran. Furthermore, our findings underscore the importance of governance, coordination and health system capacity in combating microbial threats. For clinicians and policymakers worldwide, this study serves as a reminder of the critical need for integrated and coherent policies that are responsive to the magnitude of microbial threats. It also highlights the necessity for robust M&E mechanisms to ensure the effectiveness of such policies. Finally, this study not only adds to the body of knowledge on policymaking in the context of microbial threats in Iran but also offers practical implications for global public health. By highlighting both the strengths and areas for improvement, it paves the way for enhanced policy responses to infectious diseases, ultimately contributing to a safer and healthier world.
Data availability statement
Data are available upon reasonable request. The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. This article is a part of the PhD thesis of the first author (AR), approved by the Ethics Committee of Tehran University of Medical Sciences (TUMS) (approval ID: IR.TUMS.SPH.REC.1400.059). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This article is extracted from a PhD thesis (AR) supported by the Tehran University of Medical Sciences (TUMS), Tehran, Iran. We would like to express our gratitude to Dr Haniye Sadat Sajadi for her valuable comments on data interpretation of the study. We also acknowledge all of the key informants and experts who accepted our invitation and participated in the interviews.
References
Footnotes
Contributors AT conceived and supervised the study, contributed to data interpretation and critically revised the manuscript. AR (the first author) collected data, initially analysed and interpreted data and drafted the manuscript. AAS and MY provided experts’ opinion, contributed to data interpretation. All authors read and approved the final draft. AT is guarantor. We have used AI for grammar checking.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.