Article Text

Abstract
Objective To identify physician perspectives on factors associated with physician burnout, protective factors against burnout, and to seek potential solutions for this pervasive problem.
Design A qualitative study with semistructured focus group interviews using a systematic framework analysis.
Setting and participants Physicians from general internal medicine (GIM) and the emergency department (ED) at two urban tertiary care hospitals in Vancouver, Canada, were recruited. Separate GIM and ED physician focus groups were conducted virtually from July 2021 to December 2022, led by an independent facilitator. Audio recordings from focus group sessions were then transcribed for analysis.
Results 41 physicians (29 GIM and 12 ED) participated in the focus groups. The dominant themes for organisational factors attributed to burnout that were highlighted by both groups included heavy workload and scheduling, frequent interruptions, interdepartmental conflict and feeling undervalued by leadership. Other contributing factors that were only emphasised by GIM physicians were pressure to work out-of-scope of their practice, pressure to admit and discharge patients quickly, as well as sexism in the workplace. Factors unique to ED physicians included experiencing violence in the workplace and having to assess patients in waiting rooms. Protective organisational factors included time to build rapport with patients, staff collegiality, working within their scope of practice, and feeling rewarded and valued by leadership. Interventions suggested by physicians included improving channels of communication between staff, increasing flexibility in scheduling and strengthening hospitalists’ services.
Conclusions Most organisational factors driving burnout were common to both GIM and ED physicians, including heavy workload and scheduling, frequent interruptions, interdepartmental conflict and feeling undervalued by leadership. Leveraging protective factors and intervening on organisational factors attributed to burnout such as improving communication and enhancing support services may be effective in addressing the physician burnout epidemic.
- Professional
- Physicians
- Burnout
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Multiple standardised focus group interviews were carried out, providing physician perspectives on specific systems issues in a hospital setting driving physician burnout.
Comparison and contrasting systems issues experienced by physicians that provide significant services in hospitals, the emergency department and general internal medicine.
Physician perspectives on possible solutions to systems issues were collected that may be helpful in organisational initiatives for improving physician wellness.
Systematic framework analysis was applied to identify themes converging from each focus group.
Findings may not be generalised to other non-teaching hospitals or health systems or to other specialties.
Introduction
The burnout phenomenon is defined by Maslach et al as a syndrome characterised by depersonalisation, emotional exhaustion and perceived low sense of accomplishment.1 A systematic review of 33 qualitative studies on physicians’ perspectives on burnout ranked stress factors contributing to burnout as first organisational, then relational, and lastly, individual.2 Organisational factors included heavy workloads, high amount of paperwork and insufficient time for physicians to spend with their patients and to attend to their personal lives.3–5 Relational factors referred to the conflict between professionals in decision-making. These conflicts often arise due to differences in opinion and disagreements between different departments and services. Lastly, a few studies suggested individual factors such as burden of responsibility, feelings of guilt, helplessness and doubt about abilities also contributed to physician burnout.6 7
Increasing prevalence of physician burnout has been reported across the world, with a prevalence as high as 67% in 2022 at hospitals in Canada.8 Burnout contributes to the physician shortages observed throughout Canada.9 The Canadian Medical Association’s national physician health survey in 2021 reported that 49% of respondents considered reducing their clinical hours in the near future, and those who experienced more burnout were more likely to express their intention to reduce clinical hours compared with physicians who did not report burnout.10 Therefore, improving physician wellness is now a priority for healthcare systems. Although causes of burnout in physicians are multifactorial, organisational factors have been reported as more important than individual factors such as impaired coping skills or lack of resilience among physicians.11 Although most wellness interventions have focused on improving individual-level factors such as physicians’ personal behaviours and skills, organisational changes may contribute to greater and more long-term improvements in wellbeing.12 However, there are currently few published data about specific organisational factors that contribute to physician burnout13 and few institutions have employed a comprehensive approach to tackling physician burnout.14
Our group previously determined that at least 2/3rds of physicians working in the emergency department (ED) and in general internal medicine (GIM) experienced burnout, and systems issues were considered to be the most important factors underlying burnout.8 15 Here, we conducted a qualitative study to identify specific systems issues that contribute to burnout, organisational factors that are protective, and physician-derived solutions. We used focus groups of ED and GIM physicians, as less is known on the first-hand perspective of hospital-based physicians15 16 in comparison to general practitioners17 18 on specific systems causes of burnout. Additionally, we previously found that ED and GIM physicians experience high rates of burnout as front-line care providers who often collaborate. We report our findings from a framework analysis of focus group interviews to develop a comprehensive understanding of burnout in hospitals.
Methods
Study design
We used a qualitative research design with semistructured independent focus group interviews analysed using the Framework Method.19 20 The consolidated criteria for reporting qualitative research (COREQ) were followed.21
Setting, participants and recruitment
All physicians from GIM and ED groups at two tertiary care urban academic hospitals in Vancouver, British Columbia, Canada were invited to participate in the study. Given that the interviews were meant to provide a safe space for discussing organisational issues, six physician leaders were excluded from participating in the focus groups from both groups. The division of General Internal Medicine includes 55 physicians (40% women, 75% less than age 50 years), and the Department of Emergency Medicine includes 43 physicians (36% women, 68% aged less than 50 years) who work at one or both of these hospitals. Physicians were sent an initial email from physician peers within each group inviting them to participate and two reminder emails over a 6–8-week period. All physicians who agreed to participate in the focus groups were included (29/51=57% GIM and 12/41=29% ED response rate excluding physician leaders). All physicians received remuneration for their time at standard physician remuneration rates at our hospitals.
Interview guide and focus group interviews
The interview guide was developed by a review of the literature22 23 including drawing from the Institute for Healthcare Improvement Framework for Improving Joy in Work,24 and Mayo Clinic work on organisational strategies to improve wellness,25 and content experts in physician wellness, moral distress, and qualitative research methodology from the research team. The guide was further refined with feedback and pilot tested with peer physician members from GIM and ED who later joined the project to enhance recruitment, and to improve reliability, clarity and answerability of the guide. The interview guide asked questions on (1) organisational factors that are perceived to drive burnout, (2) organisational factors that bring joy and satisfaction to work and (3) actionable interventions to reduce physician’s burnout. The interview guide is included in the supplementary material (online supplemental appendix 1).
Supplemental material
There were 5 focus groups held with 6 to 13 physicians in each group (three independent GIM physicians and two ED physicians focus groups) from July 2021 to December 2022 in a staggered fashion. An experienced female facilitator (Elizabeth Stanger, MSc.) was responsible for facilitating the focus groups. The facilitator was a project manager working at the health authority in British Columbia with expertise in operations and programme planning across multiple hospital-based programmes and facilitation in focus groups. The facilitator was not known to the participants. A peer physician who was a member of the project team was also present at each of the focus groups. Focus groups were held virtually via the Zoom platform during the COVID-19 pandemic. Participants provided verbal consent for the session recording at the beginning of the focus group interview. Participants were informed that quotes from the data analysis will not be linked to the individuals and no identifying information will be recorded or shared. The study was approved by the Providence Healthcare Research Ethics Board. The duration of each interview session was approximately 90 min. Interviews and number of focus groups were continued until no new themes emerged; this was determined by the facilitator and physician present at the session. Audio was recorded and transcribed using Otter.AI, Inc. (Mountain View, California). Transcripts were reviewed and validated by the facilitator and the peer physicians, a process through which they were de-identified and checked to ensure accurate recording and true reflection of the discussion. No repeat interviews were conducted. Transcripts and framework analyses were returned to each of the peer physicians who attended each focus group for any corrections, validation, and to ensure appropriate meaning. The identifying information of individual physicians and their expressed opinions remains confidential.
Framework analysis
Written transcripts recorded from focus group sessions were systematically analysed using framework analysis, as described by Ritchie and Spencer.26 The five key steps of framework analysis are data familiarisation, framework identification, indexing, charting and mapping/interpretation.27–30 De-identified transcripts were initially reviewed thoroughly by two independent data coders and key concepts and patterns were highlighted. Reflective notes and impressions were made based on the depth and recurrence of the topics discussed. After this data familiarisation step, the highlighted themes by the reviewers were cross-referenced and core themes were selected. The broad categories were defined from our research questions and the themes emerged from reviewing the transcripts. Once the themes were selected and agreed on by the reviewers, a table was made for each of the broad categories where the rows listed the selected themes, and the columns were labelled GIM and ED. Findings from the three GIM and two ED focus groups were compiled respectively, and differences and similarities between the GIM and ED groups were tabulated. Direct quotes from all transcripts in support of each theme were selected and assigned in corresponding cells of the tables. This organisation also allowed for a more objective comparison of evidence gathered from the two groups of physicians. Lastly, interpretation of the framework matrix was done based on contributions of the entire research team through multiple revisions and impressions. Framework analysis was conducted manually. The most frequently recurring themes were reported as major themes listed in order of decreasing frequency in the tables.
Patient and public involvement
None.
Results
Baseline characteristics
There was a total of 41 GIM (n=29) and ED (n=12) physicians participating in focus groups with 44% women participants (table 1). The emerging themes from focus group interviews were organised in three major categories of (1) organisation factors that are perceived to drive burnout, (2) organisational factors that reduce burnout by bringing joy and satisfaction to work and (3) actionable interventions to reduce physician’s burnout.
Focus group participants demographics by hospital
Organizational factors that are perceived to drive burnout
Issues in the work environment, relational issues between other physician colleagues and leaders, and workload were found common themes highlighted by both GIM and ED physicians. The four major themes within this category are listed below, with corresponding key quotes from focus group interviews presented in table 2.
Major emerging themes and associated key quotes for organisational factors that drive burnout
Interruptions and noise
Physicians found frequent interruptions while seeing patients or arranging care plans as a major challenge that affects their workflow as well as the quality of care they can provide to patients. Physicians working in hospitals experience frequent interruptions from needing to answer calls for tests, respond to or need to make requests to nursing or other physicians and trainee questions about patients. Additionally, occupational noise exposure is found to be highly disruptive. The internal ambient noises for example can be derived from crowded spaces, equipment and acoustics of the building.
Interdepartmental conflict
Frequent disputes and disagreements between different hospital services were another major contributing theme identified. Examples include disputes over which physician or admitting service would admit patients as most responsible physician or arguments about performing tests or consultations on patients. Physicians found the time and energy spent on resolving discrepancies in opinion on consultation and admission decisions to add extra unnecessary pressures to their roles.
Heavy workload and scheduling
Heavy workload, poor working hours and conflicting schedules constituted another major theme that was frequently noted by both GIM and ED physicians. Long and poorly scheduled working hours prevent physicians from attending to their personal lives and interests. GIM physicians work variable schedules with unpredictable hours which may include weekends, while ED physicians work in fixed shifts that may be scheduled during workdays, evenings, nights, weekends or holidays. ED physicians also report pressures from needing to rapidly assess, manage, and potentially discharge their case load during fixed time shifts or possibly stay late to continue caring for sick patients.
Feeling undervalued
Feeling undervalued by leadership and other consulting services was a key factor that was suggested as a contributing factor to burnout. Physicians perceived that they were not being heard by leadership as issues that they faced were not addressed.
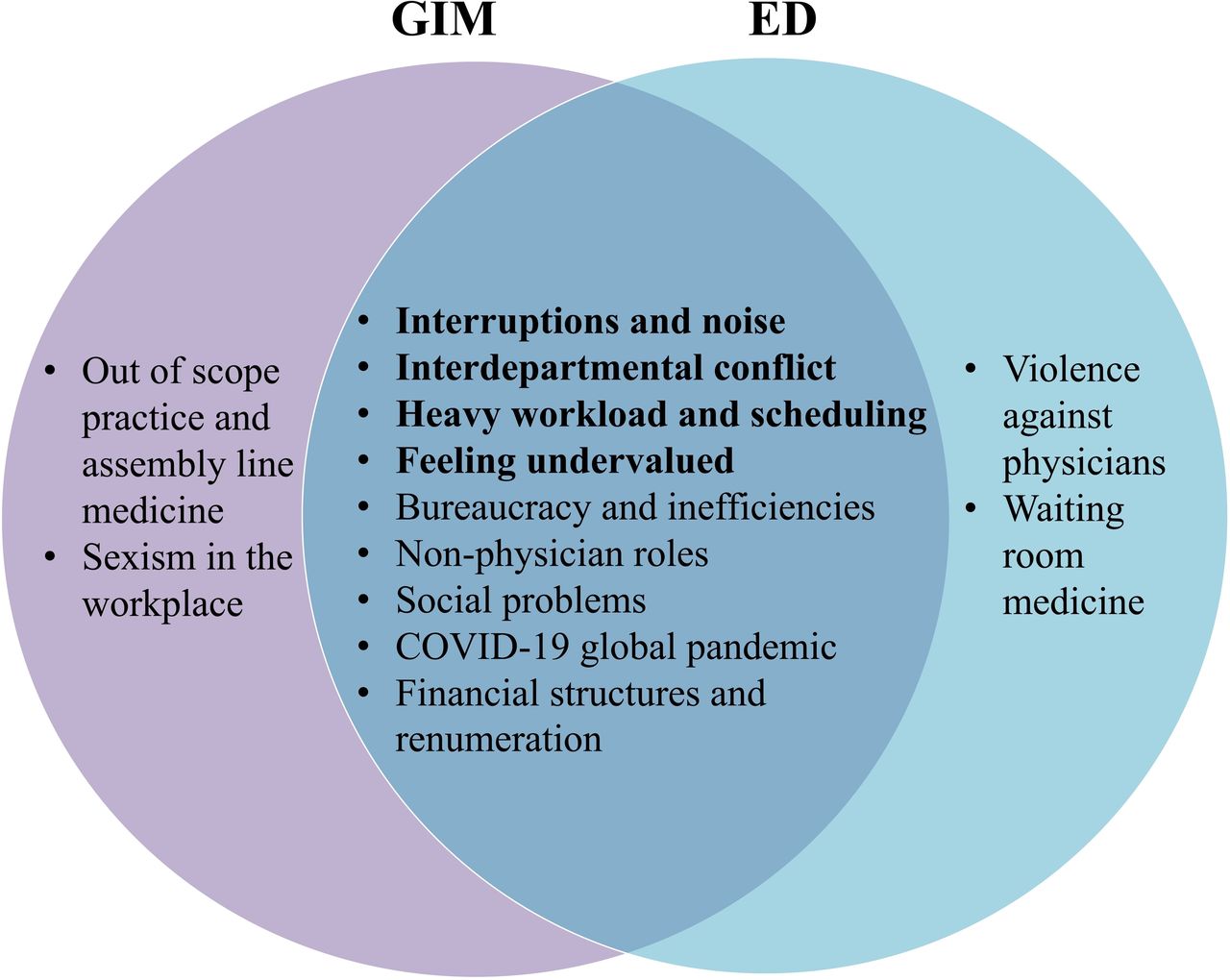
Other less prominent themes that were found to be reported by both GIM and ED physicians included (1) bureaucracy and inefficiencies, (2) non-physician roles like order entry into the electronic medical record (EMR) or portering patients within the department, or changing bedsheets, (3) moral distress from not being able to address the social determinants of health for marginalised populations, (4) COVID-19 global pandemic and (5) financial structures and remuneration where physicians are asked to perform work that is either underpaid or not paid such as administrative work. All emerging themes have been summarised in figure 1, illustrating the factors that were common to both GIM and ED specialties as well as those that were unique to each. Online supplemental appendix 2 includes a list of all associated quotes for each of the major and minor themes.

{kind=link}
Organisational factors that are perceived to drive burnout as reported by GIM and ED physicians. The four major common themes are listed in bold. ED, emergency department; GIM, general internal medicine.
Organizational factors that reduce burnout by bringing joy and satisfaction at work
The four major themes within this category are listed below, with corresponding key quotes from focus group interviews presented in table 3. Online supplemental appendix 3 includes a list of all associated quotes for each of the major and minor themes.
Major emerging themes and associated key quotes for organisational factors that reduce burnout by bringing joy and satisfaction at work
Feeling valued
Both GIM and ED physicians reported that feeling valued by patients, colleagues and leaders was a major factor bringing joy to work. Physicians reported having a sense of accomplishment and meaning through skilled patient care.
Having sufficient time to build rapport with patients
This theme was reported more frequently in GIM than in ED groups. Physicians found having enough time with patients to build a connection was a one of the satisfying aspects of their job.
Collegiality
This theme was reported more frequently in ED than in GIM groups. Physicians reported that supportive work environment and positive interactions with colleagues as major factors that bring joy to their role.
Doing physicians’ work
Being able to focus on physicians’ work such as patient examination, interacting with patients, as opposed feeling occupied by non-physician roles such as entering orders, note-taking, portering patients or making phone calls for testing as examples was another identified theme. This theme was reported by both GIM and ED groups. Physicians found the opportunity to focus on practising what they trained for to be another satisfying aspect of their jobs.
Actionable interventions to reduce physicians’ burnout
Physicians identified a number of solutions to address the identified themes that contribute to burnout. The 26 key interventions recommended by ED and GIM physicians for each previously described theme are presented in table 4. Please see online supplemental appendix 4 for a complete list of all suggested direct quotes.
All 26 key actionable interventions suggested by GIM and ED physicians to reduce burnout, listed in correspondence to the emerging themes
Discussion
Organisational factors are thought to underlie physician burnout especially within hospitals but there are little data identifying these specific issues especially in GIM. Our study identified four main themes among GIM and ED physicians that contributed to feelings of burnout including (1) interruptions and noise, (2) interdepartmental conflict, (3) heavy workload and scheduling and (4) feeling undervalued. The factors that were considered protective were largely the inverse of these (1) feeling valued by leadership, (2) having time to build rapport with patients, (3) cultivating collegiality and (4) doing physicians’ work. Most organisational issues perceived by physicians were common to both groups. Physicians also identified multiple potential strategies to improve wellness.
The first objective was to identify organisational factors that are perceived to drive burnout in physicians. In line with the systematic reviews and meta-analyses on physicians’ perspective on burnout,11 22 23 we found organisational-level factors to contribute to physician burnout. Agarwal et al have previously described high quantity of work, non-physician roles and feeling undervalued by local institutions as contributing factors to burnout in primary care providers.31 They particularly described the perception of being undervalued as being rooted in lack of boundaries in responsibilities, inadequate communication and collaboration with leadership, and insufficient acknowledgement of the challenges faced by primary care providers.31 Heavy workload,3 5 32–38 difficult working conditions, lack of time3 33 35 38 39 and the constant pressure to perform tasks quickly are the most commonly reported organisational contributors to burnout.11 In a cross-sectional survey from practising oncologists, 73% reported symptoms of burnout that was driven by working in a chaotic atmosphere, feeling unappreciated, poor control over workload and discomfort in discussing workplace stress with peers.40 In our study, however, themes of interruptions and noise as well as interdepartmental conflict emerged as major stressors in the workplace. This is likely because qualitative studies on physician burnout in hospital-based medicine and particularly GIM and ED specialties are less common, leaving such fixable problems unidentified and unaddressed. One of the major sources of interdepartmental conflict is the frequent disagreement between services and the pressure to admit patients while both sides are overwhelmed and are not well supported. Although practically this issue arises between individuals, it is the organisational structure and process that places physicians on opposite sides of conflicts. Lastly, the other aspect of the interruption and internal ambient noise complaint is rooted in the over-stimulating and chaotic environment in which hospital-based care providers practice in, an issue that may be less of an issue in primary care settings. With regard to sexism in the workplace, female GIM physicians reported experiencing microaggressions and intimidation from older male staff which directly contributed to their experience of burnout. Gender bias has also been reported previously as a major barrier to career satisfaction by female surgeons and recognised as a risk factor for burnout.7
Second, when exploring protective factors, being rewarded and valued were emphasised by both groups equally. Previous research recognised primary care providers’ feelings of being undervalued by local institutions and healthcare systems as a major contributor to burnout.31 Another study also identified lack of recognition as a contributor to burnout among physicians in French hospitals.41 Interestingly, having time to build rapport with patients and reducing interruptions were more frequently suggested as protective factors by GIM physicians compared with their ED colleagues. GIM physicians often discussed having time to connect with patients and improving the quality of that time by reducing interruptions as factors that bring satisfaction to their jobs. Meaningful physician-patient relationships had previously been described as a protective factor against burnout in family physicians, including major themes of patient-centred care, continuity, effective care, trust and purpose.18 During the COVID-19 global pandemic, creating such meaningful relationships was further hindered by the widespread use of telehealth and reduced patient time.17 However, most studies were focused on family physicians and to our knowledge, these pertinent protective factors have not been previously reported from hospital-based providers. On the other hand, the last two identified factors of cultivating staff collegiality and doing physicians’ work were more heavily emphasised by ED physicians. They found positive interactions with the staff, interesting cases and good medicine as key factors that bring joy and satisfaction to their otherwise demanding roles. The concept of collegiality, teamwork and fostering community among physicians as an effective way to protect against burnout has also been reported previously.7 31 42 43 Although at face value collegiality may appear to be an individual-level factor, evidence suggests that organisational modifications are most influential in cultivating a satisfying and joyful environment for physicians. A recent qualitative study of job and life satisfaction among ED physicians suggests that regardless of physicians’ self-identification as introverted or extroverted personalities, those with better job satisfaction tended to be more socially connected.44 Overall, although protective factors that bring joy and satisfaction to physicians are often overlapping, it is important to consider the speciality-specific factors and to strengthen protective factors that are intertwined with the nature of each specialty. Moreover, augmenting areas where physicians find value in their roles and incorporating their perspective in organisational-level decision makings are fundamental in building resiliency against burnout.
Few previous studies have sought the perspective of the practising physicians on interventions to prevent burnout. Additionally, few institutions have employed a comprehensive approach to tackle physician burnout as an organisational priority.14 Lack of physician input into interventions to improve wellness may also underlie the lack of physician engagement in wellness interventions. Broad recommendations such as reducing and also compensating physicians for the time they spend documenting in the EMR, expanding support staff, and increasing positivity and collegiality have been described to improve the well-being of healthcare providers.42 Others suggested a cultural change from stigmatisation and competitiveness to compassion and collaboration, starting from medical school training.45 Primary care physicians also recommended solutions in another qualitative study around the general themes of fostering community among colleagues, advocating for reforms beyond institutions, promoting the primary care providers’ voice, and recalibrating expectations and reimbursement levels.31 In this study, we sought specific solutions from physicians, leading to a list of 26 actionable recommendations to be implemented (table 4). As supported by the literature, we believe that direct discussions through similar repeated focus groups and ongoing facilitated peer support sessions46 with input from physicians are fundamental to identifying contributors to burnout. To address the root causes at an institutional level, Shanafelt et al proposed four fundamental components of promoting foundational programmes, cultural transformation, rapid iterative experimentation and sustainability.25 47 Future studies should also integrate qualitative interview findings from physicians and operations leaders, and late career physicians, to comprehensively address the organisational factors driving burnout.
Although several informative themes have emerged from this study, our findings are not without limitations. One of the limitations is that while our study provided rich information on organisational factors in the ED and GIM at two urban tertiary care academic hospitals, our findings may not be generalised to hospitals, departments or healthcare models or specialties different from those under study as organisational issues may reflect local environments, available resources and the patient populations. However, it is likely that the highlighted issues are common and would resonate with other groups and urban hospitals. Second, given the qualitative nature of the study, it is challenging to assign value to each of the themes identified from focus groups or individuals within each group. Even though most themes were selected because they were more frequently mentioned, it is unclear which organisational factor contributes the most to burnout and ultimately, which intervention would be most effective in reducing burnout. Third, physician leaders were excluded from participating in the focus groups in order to provide a safe space for discussing organisation issues, and the peer physician involved in the development of the interview guide also participated in the focus groups to ensure its adequacy. It should be noted that leaders may have additional perspectives on organisational issues.48 There are also demographic limitations that should be considered including the relatively small sample size, discrepancies in the number of participants in each of the groups, and the fact that the majority of the participants were younger than 50 years old. Additionally, burnout was not objectively evaluated for each participating physician in this study, and the focus group participants may have had varying levels of prior or ongoing experience with burnout. Lastly, although the vast majority of challenges reported in the focus groups appeared to precede the global pandemic, it must be noted that the interviews were conducted during the pandemic. Nonetheless, identifying contributing factors to burnout during or prior to the pandemic is crucial and physician burnout is likely an overlooked issue that was particularly brought to attention during the COVID-19 pandemic.
Conclusion
Organisational issues that contribute to high rates of burnout in frontline physicians in hospitals include interruptions and noise, interdepartmental conflict, heavy workload and feeling undervalued by leadership. Most of these contributing factors to burnout are resolvable, many of which can be addressed at low cost. Achieving wellness for healthcare providers must be a priority focus for healthcare systems, and organisational change is an important path to improving wellness.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Providence Health Research Ethics boards H018-02999. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Contributors NK, AP, PD, HL, DL, ES and AS contributed to the design of the study. NK, ES, DR, ER, VV, KR, AS, AP, AT and DL contributed to data collection and FG, ES and NAK contributed towards analysis. All authors contributed to interpretation of the results, and meaningful contribution to writing and accepting the final manuscript. NK had full access to all the data in the study and is responsible for the overall content as guarantor.
Funding Providence Health Care Medical Staff Association.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.