Article Text

Abstract
Objective This study aimed to assess the informed consent practice process and associated factors among healthcare workers for major surgical procedures at Gurage zone hospitals, in 2022.
Methods and materials Institution-based cross-sectional study was employed.
Settings This study was conducted in Gurage zone hospitals.
Participants All healthcare workers who have been working in Gurage zone hospitals of surgical, operation rooms and obstetrics/gynaecology wards had exposure to patients who had undergone surgery during the study period
Outcome The primary outcome of the study was the practice of informed consent practice among healthcare workers in Gurage zone hospitals.
Result A total of 448 study participants were involved in this study giving a response rate of 98%. The mean (±SD) age of the study participants was 29.16 (±4.06) years. The mean score of study participants towards the surgical informed consent was 19.5, and 260 (58%, 95% CI: 53.7, 62.5) of them had good practice in the surgical informed consent. In multivariable logistic analysis model, factors like favourable attitude towards informed consent 2.4 (1.556, 3.596), work experience participants 4.9 (2.8, 8.7), adequate knowledge of informed consent 2.5 (1.6, 3.9) and communication challenge 1.6 (1.07, 2.50) were independently associated with the practice of informed consent at a p value of <0.05.
Conclusion More than half of healthcare providers had good practice towards the surgical informed consent process. The practice of informed consent is low, and it is better to work on healthcare providers’ in-service training, knowledge and attitude towards informed consent.
- ETHICS (see Medical Ethics)
- Health Services
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data set used or analysed during this study is available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THE STUDY
We used a multicentre study setting which is crucial for conclusion for the study area.
We used a validated tool to assess the practice of informed consent.
Since the study design is cross-sectional, cause-and-effect relationship cannot be established.
Self-reporting bias might affect the outcome of the study since some respondents may not report what they practice.
Introduction
Informed consent is a core concept in the process of communication between a patient and healthcare provider.1 Surgical informed consent is not only putting a signature on a piece of paper but is also an ongoing process that begins in initial contact with the patient and continues through surgery and postoperative care.2 3 It is an established ethical and legal requirement for surgical treatment with paramount importance to protect both the patient and healthcare providers from unnecessary accusations.3 4 It is the healthcare professional’s obligation to disclose information to the patient to undergo a specific medical intervention that is fundamental to the proper care and treatment of patients.5
Putting a signature on the informed consent form does not by itself constitute informed consent; it is the whole complex process of gaining information, deciding and consenting.2 5 According to the Canadian Medical Association, informed consent is the primary paradigm for protecting patients’ rights and guiding ethical practice.4 Surgical informed consent is vital for acknowledging patients’ autonomy and self-determination as well as for promoting shared decision-making by shifting the care from physician-centred to patient-centred.2 The updated World Medical Association Declaration stated that the consent process should respect the patient’s right to refuse or agree to any diagnostic procedures or treatments.6
The information given is the most determinant factor for decision-making in the consenting process.2 The reason for surgery, the proposed type of surgery, the risks and benefits of the proposed surgery, alternative treatments and the benefits of refusing therapy should be incorporated into the consent.2 4 A legal and ethical context of informed consent requires five key elements to establish validity which include competence, voluntariness, information disclosure, understanding of information disclosed and authorisation or consent to the medical procedure.7
The informed consent is the cornerstone of shared decision-making, legal requirement and ethical obligation for all surgical procedures if it is properly practiced.8 Despite this fact, it is inconsistently practiced and rarely achieves the theoretical ideal. Without a basic understanding of the nature of the procedure, risks, benefits and treatment alternatives, the patient cannot meaningfully participate in decision-making. Therefore, to provide safe, quality, patient-centred healthcare, it is important to emphasise the proper informed consent process.9
Studies conducted in different countries of the globe (the UK, Pakistan and the Netherlands) showed that the practice of surgical informed consent among healthcare providers did not meet the minimum standard when they performed informed consent with their patients.10–12 A study done in Iran showed that only 12.6% of nurses give sufficient information to their patients to assure suitable practice of informed consent.13
Studies conducted in the African region showed that the practice of proper informed consenting practice is poor. For instance, in studies done in Uganda and Egypt, only 50% of surgeons obtain informed consent with adequate information before major surgical procedures.14 15 Similarly, 65.7% of the clients reported that they are not being informed about their procedure and instead simply ordered to put their signature on the informed consent sheet.14 A study that was conducted in Bale Zone hospitals showed that only 50% of healthcare professionals practice the proper informed consenting process.16
Previous studies in different countries of the world mainly focus on informed consent from patient perspectives and showed that there is a gap in the informed consenting process. However, factors affecting the informed consent process are not yet addressed. There is also scarce information on the practice and factors affecting the informed consent process from a healthcare perspective in the study area and even in Ethiopia. Therefore, this study aimed to assess the informed consent practice process and associated factors among healthcare workers for major surgical procedures at Gurage zone hospitals in Ethiopia.
Methods
Study setting and study design
This study was conducted in public hospitals in the Gurage zone, South Ethiopia. The Gurage zone is one of the 11 administrative zones and four special woredas in the Southern Nation Nationality People Region (SNNPR). Wolkite town is the capital city of the Gurage zone. It is found 153 km southwest of Addis Ababa, the capital city of Ethiopia. According to the Ethiopian national census of 2007, it has a total population of 1 279 646. There are six hospitals (five public and one non-governmental) serving the catchment population in the zone. An institution-based cross-sectional study was employed.
Participants
The source populations were all healthcare workers (nurses, midwives, GPs, surgeons, gynaecologists and anaesthetists) working at Gurage zone hospitals. All healthcare workers who have been working in Gurage zone hospitals of surgical, operation rooms and obstetrics/gynaecology wards and had exposure to patients who had undergone surgery during the study period were the study populations.
Inclusion and exclusion criteria
All healthcare workers (nurses, midwives, doctors and anaesthetists) who worked for at least 6 months in the hospital were included. Healthcare workers who were on annual leave, sick leave or training were excluded from the study. Those who have not been working in surgical, labour, emergency, obstetrics and gynaecology wards and operating rooms in the last 6 months were excluded.
Goals of study
To assess the practice of informed consent among healthcare workers for major surgical procedures of Gurage zone hospitals, 2022.
To identify factors affecting informed consent practice among healthcare workers for major surgical procedures of Gurage zone hospitals, 2022.
Sample size determination and sampling procedures
Sample size calculation
The minimum required sample size was calculated by using a single population proportion formula, assuming the prevalence of informed consent practice as 50.1% based on a study conducted in southeastern Ethiopia,16 5% margin of error at 95% CI as follows:

n=Sample size
p=Proportion =0.501
d=Margin of error=0.05
q=1 p = 0.499
Z=1.96 at a 95% CI
n= (1.96)2 × 0.501 × 0.499/(0.05)2= 0.960/(0.05)2 ~384
By adding 10% for possible non-response rate, the total sample becomes 423.
Sampling procedure
There were six hospitals in Gurage zone: Wolkite University Comprehensive Specialised Hospital, Butajira General Hospital, Gunchirie Primary Hospital, Agena Primary Hospital, Buie Primary Hospital and Atat Lord Maryam Primary Hospital. There were 457 healthcare providers involved in the informed consent in the last 6 months in Gurage zone hospitals. Since the total population (457) was small enough to apply the sampling technique, all (457) were included in this study.
Measurement of variables
Thirteen structured Likert-type questions with options of ‘never’, ‘sometimes’ and ‘always’ which scored 1, 2 and 3, respectively, will be used to assess the practice of informed consent, and the total score for practice was dichotomised into good and poor practice using the mean score as the cut-off point.
Good practice: A score greater than or equal to the mean score for the practice questions.
Poor practice: A score below the mean score for the practice questions.
Adequate knowledge: A score greater than or equal to the mean score for the knowledge questions.
Inadequate knowledge: A score below the mean score for the knowledge questions.
Favourable attitude: A score greater than or equal to the mean score for the attitude-related questions.
Unfavourable attitude: A score below the mean score for the attitude-related questions.
Covariates
Sociodemographic characteristics (age, sex, educational profession and communication barrier).
Organisational factors (lack of standard consent form, in-service training, time constraints, availability of interpreter), workload and working unit.
Healthcare worker-related factors (knowledge, attitude) and work experience.
Data collection tool and procedure
Data were collected by using a pretested structured questionnaire developed after the review of different kinds of literature. The questionnaire contains five parts: socio-demographic characteristics, organisational related, knowledge part, attitude section and informed consent practice assessment-related items. Data were collected by six BSc nurses and two supervisors after 1 day of training by the principal investigator. Data were gathered using a self-administered structured questionnaire.
Data quality control
A pretest was done on 5% of the samples. The 1-day training was given by the principal investigator to the data collectors and supervisors before data collection. The training was focused on understanding the meaning of each question, obtaining consent, keeping the confidentiality of the information they gathered and quality of data collection. Emphasis was given on the significance and the appropriate meanings of each question as well as how to explain to the participants in an understandable manner if required. On top of this, supervisors were following data collectors and the investigator was also checking for the collected data clarity and completeness. The double data entry method was used by two data clerks, and the consistencies of the entered data were cross-checked by comparing the two separately entered data.
Data management and analysis
Before data entry, questionnaires were checked for completeness and clarity. Cleaned and coded data were entered using Epidata 3.1 and exported to SPSS Windows version 25 for analysis. Percentage and frequency were calculated. The findings of the study were presented by using tables, graphs, charts and narration. The bivariate analysis was used primarily to check which variables have an association with the dependent variable individually. The goodness of fit was tested by the Hosmer-Lemeshow statistic which is greater than 0.05. All variables with p≤0.25 in the bivariate analysis were included in the final model of multivariate analysis to control all possible confounders. The multicollinearity test was carried out to see the correlation between independent variables by using SE and collinearity statistics (VIF>10 and SE>2 were considered suggestive of the existence of multicollinearity). The degree of association between independent and dependent variables was assessed using an adjusted OR with a 95% CI. Finally, the variables that have a p-value of <0.05 were considered statistically significant.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Results
From a total of 457 sample sizes, 448 study participants were involved in this study with a response rate of 98%.
Sociodemographic characteristics of the study participants
The mean (±SD) age of the study participants was 29.16 (±4.06) years. More than half of 241 (53.8%) of the study participants were male health professionals. Regarding the marital status of respondents, half 228 (50.9%) of them were married. Nearly three-fourths 327 (73%) of the study participant’s professional experience was greater than or equal to 5 years. Regarding the specialty of respondents, more than half 249 (55.6%) of them were nurses (216 (48.2%) BSc and 33 (7.4%) clinical nurses) and one-quarter of the participants were midwifery (table 1).
Sociodemographic-related factors of the informed consenting process for major surgical procedures among Gurage zone hospitals healthcare providers, Southern Ethiopia (n=448)
Organisational related factors
Among the participants, nearly one-third of them were working in surgical (146, 32.6%) and operation rooms (162, 36.2%). Regarding the number of patients cared for per day, more than 40% (196, 43.8%) of the study participants were given to care for about 6-10 patients per day. More than half of (238, 53.1%) the study participants reported that there is administrative support. Of the study participants, two-thirds (300, 67%) of them had no training regarding the surgical informed consent process. The majority of the study participants (369, 82.4%) reported that the informed consent form contents were not adequate and standard in their setup. Nearly three-fourths (329, 73.4%) of the study participants reported that they had specific policies or regulations of informed consent in their institution (table 2).
Organisational related factors of the informed consenting process for major surgical procedures among Gurage zone hospitals healthcare providers, Southern Ethiopia (n=448)
Knowledge, attitude and practice of respondents
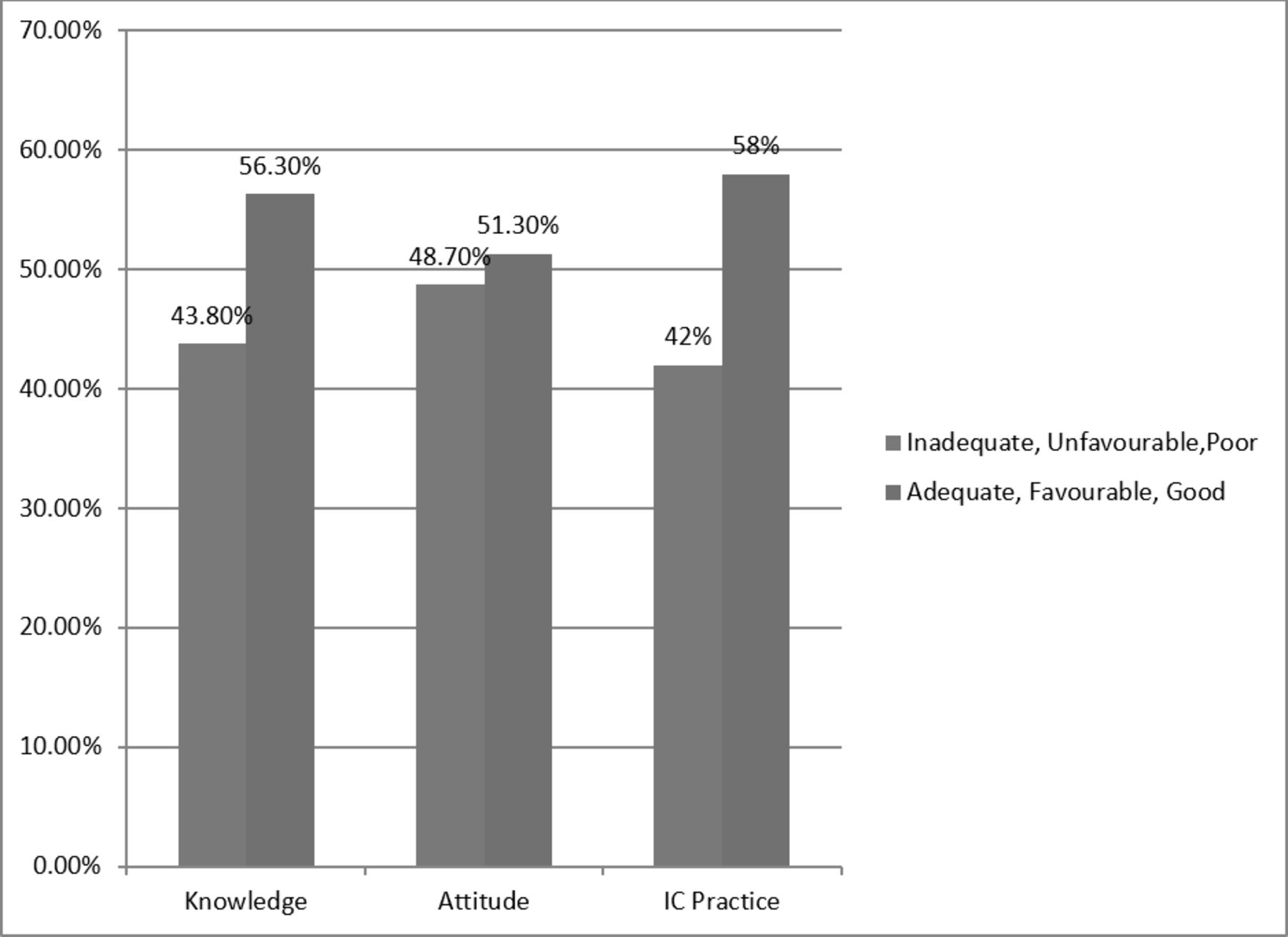
The mean score of study participants’ knowledge was 14, and more than half of 252 (56.3%) of study participants had adequate knowledge of the surgical informed consenting process. Regarding the attitude of respondents, the mean score of attitude was 37, and more than half of 230 (51.3%) participants had a favourable attitude towards the surgical informed consenting process. The mean score of study participants towards the surgical informed consenting process was 19.5, and 260 (58%, 95% CI: 53.7, 62.5) of them had good practice in the surgical informed consenting process (figure 1).

{kind=link}
Knowledge, attitude and practice of informed consenting process for major surgical procedure among Gurage zone hospitals healthcare providers, Southern Ethiopia (n=448)
Factors associated with the surgical informed consent practice
In this study, variables such as working experience, knowledge of informed consent, attitude towards informed consent, communication barrier, training on informed consent and content of informed consent were factors significantly associated with informed consenting practice in the bivariable logistic analysis model. In the multivariable logistic analysis model, factors such as attitude towards informed consent, work experience of participants, knowledge of informed consent and communication barrier were independently associated with the practice of the informed consenting process at a p-value of <0.05.
In our study, participants who had ≥5 years of working experience were 4.9 (2.8, 8.7) times more likely to practice the surgical informed consenting process properly compared with the respondents who had <5 years of experience. The odds of performing informed consenting practice properly were 2.5 (1.6, 3.9) times in healthcare providers having adequate knowledge compared with their counterparts. Similarly, those study participants who had a favourable attitude towards the informed consenting process were 2.4 (1.556, 3.596) times more likely to practice informed consent properly. Finally, healthcare providers who did not face a communication challenge in the consenting process were 1.6 (1.07, 2.50) times more likely to practice the informed consenting process compared with their counterparts (table 3).
Multivariable logistic regression analysis for factors associated with the informed consenting practice for major surgical procedures among Gurage zone hospital healthcare providers, Southern Ethiopia (n=448)
Discussion
The practical application of an interactive healthcare provider-patient relationship and respect for the patient’s autonomy is assured by obtaining surgical informed consent from patients before the procedure.17 18 In our study, the surgical informed consent process practice and factors associated with it were assessed. The findings of the study revealed that about 58% (95% CI: 53.7, 62.5) of healthcare providers had good practice towards the surgical informed consenting process. Our study finding is higher than the study conducted in Turkey (32.6%),12 Uganda (48.8%),15 southeastern Ethiopia (50.1%)16 and in another study in Ethiopia (32.7%).19 The possible explanation could be a difference in sample size (small sample size in Uganda and Turkey), study setting and study participants (only nurse professionals were involved in Turkey) as well as operational national definitions used to categorise as good and poor practice.
The findings of the study were lower than those of the study conducted in Italy 71%.20 The possible justifications could be study participant differences, study setting differences, as well as the socioeconomic differences between the studies. A study conducted in Italy incorporates only nurse professionals, whereas we included all healthcare providers, and our study included five different hospitals to select study participants which may vary in patient flow, healthcare provider-patient ratio as well as difference in hospital setup compared with a study done in Italy.
Our study findings showed that healthcare providers who had greater than or equal to 5 years of experience were five times more likely to practice surgical informed consent compared with those whose working experience is less than 5 years. The finding is congruent with a study done in Italy,20 the Democratic Republic of Congo,21 and southeastern Ethiopia.16 It is a fact that experience has the advantage to get in-service training related to the informed consenting process and practicing informed consent properly. Experience also has an effect on having good relationships and communication between patients; as a result, they can easily exercise informed consenting practice.
Healthcare providers who had good knowledge regarding surgical consent were 2.5 times more likely to practice surgical informed consent than those who had inadequate knowledge. This finding is consistent with the study done in Pakistan,22 the Cape Coast metropolis of Ghana23 and southeastern Ethiopia.16 Having a basic understanding of the surgical informed consent process aids in integrating the component of consent and practicing it effectively. It is also a fact that having a basic understanding of the components of informed consent, the implementation of the informed consenting process will become optimal and properly practiced.24 Similarly, healthcare providers with a favourable attitude were 2.4 times more likely to practice surgical informed consent compared with their counterparts. The finding is supported by studies done in Pakistan22 and southeastern Ethiopia16 and cross-sectional studies in Ethiopian health facilities.19 Having a favourable attitude is fundamental and enhances motivation to practice surgical informed consent as well as other procedures in the healthcare setup. The other possible justification might be the attitudes of healthcare personnel influence what they do, and those who have a positive attitude are more positive to perform activities positively.25
In this study, healthcare providers who did not face communication barriers with patients were 1.6 times more likely to practice surgical informed consent compared with those who faced communication barriers with their clients. The possible explanation might be taking informed consent from patients across language barriers can be very difficult and is often a source of major frustration both for patients and for healthcare providers.26 27 Studies suggested that language barriers and the absence of trained interpreters for effective communication have a negative impact on the process of informed consent as a result hinders the quality of patient care.28 Another previous study in South Africa revealed that the absence of appropriately trained interpreters is a major barrier to the surgical informed consent process for healthcare providers.7 29
As a limitation, our study design is a facility-based cross-sectional study, and cause-and-effect relationship cannot be established. Our study uses paper-based questionnaire, self-reporting bias might affect the outcome of the study since some respondents may not report what they practice.
Conclusions
More than half of healthcare providers had good practice (answered above the mean) towards the surgical informed consenting process. The finding of this study showed that the practice of informed consent is low. In this study, participants who had ≥5 years of working experience, healthcare providers having adequate knowledge, participants who had a favourable attitude towards the informed consenting process and healthcare providers who did not face a communication challenge in the consenting process were factors independently associated with the surgical informed consenting practice. It is better to work on healthcare providers’ knowledge related to informed consent, communication challenges as well as attitude towards informed consent. For future researchers, we recommended considering a multidimensional approach that includes observations as well as interviews with healthcare providers at different levels across the country. We also recommend that researchers use triangulations (to add a qualitative aspect). Future researchers are also recommended to conduct longitudinal research to confirm a definitive cause-and-effect relationship between the practice of informed consent and the independent variables.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data set used or analysed during this study is available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Institutional Ethical Review Committee Board of Wolkite University with reference number (Ref no. RCSUIL024/14). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge Wolkite University for funding this research. We would like to acknowledge all data collectors and respondents. The authors also extend acknowledgments to the hospital administrators of the Gurage zone to allow us to conduct this research.
References
Footnotes
Contributors Authors’ contribution: BTZ (guarantor of the research): contributed in the conceptualisation, investigation, supervision, resource, validation, writing the original draft, and writing-review and editing. SG: contributed in the conceptualisation, supervision, resource, validation, writing the original draft, and writing-review and editing. BC: contributed in the conceptualisation, investigation, resource, validation, writing the original draft, and writing-review and editing. TL: contributed in the conceptualisation, data curation, formal analysis, investigation, resource, and writing the original draft. MAE, YM, DT, TS, YS, and HA: contributed in the conceptualisation, formal analysis, investigation, methodology, and writing-review and editing. SG, AA, and ZM: contributed in the conceptualisation, formal analysis, investigation, methodology, and writing-review and editing.
Funding The study was financially supported by Wolkite University with reference number (RCSUIL024/14).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.