Article Text

Abstract
Rationale and Objective Globally, the COVID-19 pandemic necessitated a rapid introduction of virtual care delivery via telephone or videoconference. The rapid advancements in e-health technology facilitated options for virtual care, including asynchronous data transfer in virtual clinic models and patient-facing smartphone applications for communications and self-care. However, the clinical benefits of virtual consultation have not been consistently demonstrated in all facets of kidney care, and the adoption of this innovation alters workflows and health professionals’ perceptions of care delivery. This study evaluated the integration of virtual outpatient consultation safely and effectively into the kidney care programme in Alberta.
Study design We leveraged a mixed-methods approach to collate data about clinicians’ experiences and opinions, forming the basis for the qualitative part of the study.
Data extraction Data were collected through surveys, interviews and focus groups of nephrologists and home dialysis nurses.
Analytical approach Focus group/interview transcripts for nephrologists and nurses were used to generate initial codebooks, which were iteratively refined throughout the analysis. Codes were categorised and analysed thematically, and data collected from nephrologists and nurses were analysed separately.
Results The findings demonstrated that clinicians support the use of routine virtual care. Clinicians’ opinions on implementation requirements emphasised logistics for routine virtual care integration, quality of care delivered, impacts on the therapeutic relationship and regulatory policy clarification.
Limitation The generalisability of the findings is limited in scope, as the study was conducted in a single nephrology programme in Canada, and may not apply to other provinces or settings.
Conclusions These findings inform recommendations for safe and effective virtual care delivery and can be leveraged to inform virtual care designs in kidney care programmes. Further study is required to clarify the impacts of virtual care on specific population demographics based on geography (rural vs urban) and age (elderly population) in the post-COVID-19 era, and determine how to effectively integrate patient perspectives into this model of care.
- Dialysis
- Nurses
- Chronic Disease
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The use of virtual consultation in kidney care has evolved over the last few years, particularly during the pandemic era. It is, therefore, imperative to understand the barriers and facilitators for effective integration into care programmes.
This is the first attempt in the province of Alberta, Canada, to explore the requirements for a safe and effective integration of virtual outpatient consultation in the Alberta Kidney Care (AKC).
We explored the integration of virtual outpatient consultation safely and effectively into the AKC Programme leveraging a mixed-methods approach.
The unique approach to data collation, analysis and interpretation in this study yielded significant insights into clinicians’ perspectives and facilitated the development of theoretical concepts to guide a safe and effective virtual consultation in kidney care programmes.
The stakeholders’ opinions on implementation requirements pointed to logistics for routine virtual care integration, quality of care delivered, impacts on the therapeutic relationship and regulatory policy enactment.
Introduction
Across kidney care programmes worldwide, outpatient consultations typically involve in-person visits, despite increasing patient numbers, travel burdens and co-morbidity.1 However, the COVID-19 pandemic required the rapid introduction of virtual care delivery in patients’ homes via telephone or videoconference. Additionally, options for virtual care are expanding, including asynchronous data transfer in virtual clinic models and patient-facing smartphone applications for communication and self-care.2
Clinical benefits of virtual consultation (defined in this context as real-time communication between patients and clinicians via portals such as telephone, Skype or videoconferencing) can include improved access to care and potentially reduced costs for individual patients and the healthcare system. The clinical benefits of virtual consultation have not been consistently demonstrated in nephrology; however, the adoption of this innovation can significantly alter workflows and professional roles.3 Acceptance by clinicians has been shown to be of primary importance in the adoption, scaling and sustainability of such technologically driven care platforms. This makes it imperative to explore the understanding of clinicians’ perspectives on virtual consultation in order to facilitate the introduction of best practices.4 In prior research, clinicians have expressed concerns regarding the routine use of virtual care, including possible diagnostic limitations, a need for additional technology and an absence of legal and professional policies to support best practices. Importantly, research on physicians’ attitudes and emerging implementation frameworks demonstrates a need to evaluate context-specific challenges to scale up and sustain this change.5 Such findings could inform policymakers and help them draft best practice recommendations for nephrologists and other kidney care professionals in Alberta and beyond.
We, therefore, aimed to undertake this study in order to explore the perceptions of healthcare professionals involved in kidney care in the province on the (1) utility of virtual care in enhancing access to and quality of care, (2) common barriers to its integration and (3) requisite policy changes towards successful implementation and scale-up within the province and beyond.
Methods
Setting
This study was conducted in the province of Alberta, Canada, under the auspices of Alberta Kidney Care (AKC), which is part of Alberta Health Services (AHS). This kidney care programme is one of the largest individual programmes in Canada, providing care to over 4.5 million people residing in Western and Northern Canada. The programme provides comprehensive kidney care covering areas in Northern Alberta, as well as parts of British Columbia and Saskatchewan. The 24 nephrologists working in the programme are remunerated under two funding models: private fee-for-service and alternative funding (salary-based) plans. Nursing staff remuneration is largely salary-based in the province. The study was approved by the University of Alberta Health Research Ethics Board.
Population of study
With the onset of the COVID-19 pandemic in March 2020, under direction from AHS, outpatient consultation in AKC-North (AKC-N) was rapidly transitioned from in-person visits to virtual formats (telephone or videoconferencing). This transition specifically involved outpatient clinics that serve patients with needs related to general nephrology, advanced chronic kidney disease and home-based dialysis. Two clinician stakeholder groups in AKC were most directly affected by the transition:
Nephrologists working in both private practice and academic settings with alternative funding practice models.
Nurses in the home dialysis therapies programme administering peritoneal dialysis and home haemodialysis.
Informed consent was sought from the physicians and nurses.
Design and approach
We studied how to integrate virtual outpatient consultation safely and effectively into the AKC Programme. Adopting a mixed-methods approach, we collected and analysed data about clinicians’ experiences and opinions on facilitators and barriers to the use of virtual care. It is well established that surveys are a useful tool in evaluating the characteristics, attitudes and behaviours of a population under study at a high level.6 Findings can then be used to inform subject matter and sampling for more in-depth explorations of attitudes through interviews and focus groups. The inclusion criteria for involvement in the study were as follows:
Participants had to be practising clinicians (nephrologists or home dialysis therapy nurses) in the AKC programme. Regulatory policies for virtual care are under the jurisdiction of the provinces; hence, the survey was confined to clinicians in Alberta rather than other provinces to standardise practice conditions.
Clinicians had to be involved in the routine care of outpatients. Particularly in academic centres, a few clinicians predominantly work in research or administrative roles. The perspectives of clinicians who work with outpatients are the most relevant to inform future practices.
Clinicians had to have over 1 year of experience in the AKC programme. This requirement ensured clinicians had experience in outpatient consultation in the AKC programme both prior to and during the COVID-19 era.
Survey sampling (recruitment) strategy and rationale
The population of nephrologists and home dialysis nurses in Alberta has a history of close collaboration on clinical, research and administrative initiatives. To obtain as complete a narrative as possible, it was feasible to survey all nephrologists and home dialysis nurses (ie, total population participation). Purposeful sampling of all virtual care users was the most appropriate approach,6 as the ultimate purpose of this study is to inform the utilisation of virtual consultation within a group practice. Thus, it was important to seek as large a representative sample of opinions within the group as possible. Surveys were distributed between April and May 2021. Surveys were disseminated to physicians using publicly available email addresses and to nursing staff via paper copy and were returned to a locked collection box in the home dialysis units.
Interview and focus group sampling criteria and rationale
Surveys included a question requesting permission to contact informants for interviews and/or focus group participation. Informants were selected based on two criteria:
Participants had agreed to be contacted for interviews or focus groups on the survey.
Participants were selected based on age and reimbursement model to introduce an element of maximal variation sampling.
Interview and focus group sampling (recruitment) strategy and rationale
Participants satisfying the criteria described above were contacted by email to verify participation and confirm interview times. Up to 20 responses were sought as this number was expected to give adequate breadth or less if data saturation was reached. Focus group members were selected by convenience sampling at the University of Alberta hospital site, using a pre-existing clinical meeting. During these regularly scheduled meetings, clinicians review clinical, research and administrative issues. As new topics are frequently sought, two of these sessions during the study period were available to be used for focus group purposes. The nephrology division is small (25 nephrologists), and rounds are generally well attended by a cross-section of divisional members.
Data collection and instrumentation
Two approaches to data collection were used in this study: a questionnaire survey and focus groups/interviews. Analysing themes in these complementary data yielded insights into clinicians’ perspectives and facilitated theoretical development to determine the requirements for safe and effective virtual consultation in AKC-N.
Questionnaire surveys
The survey enabled utilisation patterns and preferences to be identified and provided a high-level view of common implementation barriers and facilitators.6 As all clinicians used electronic means of communication, online surveys were administered (online supplemental appendix 1). The Select Survey instrument was used as AKC members were familiar with this tool, and an institutional license was in place. The survey content was developed based on a literature review of the determinants of innovation acceptance by clinicians. These determinants have often been structured using the Technology Acceptance Model and its derivatives. Although many such models exist, chief characteristics include perceived ease of use and perceived effectiveness of technology.7 Later models have shown an increased capacity to explain up to 80% of the variation in attitudes when demographic factors and social determinants are considered.8 Hence, the survey included items pertaining to:
Supplemental material
Demographic factors.
The usefulness of virtual consultation.
Facilitating conditions.
Attitudes towards emerging communication technologies.
Several steps were taken to ensure the validity and reliability of the survey instrument. First, to minimise the number of non-responders, the survey was embedded in a personalised email that outlined study aims and privacy protection measures and included a reminder that participation was voluntary. The survey length aligned with published recommendations, and responses were not mandatory for any questions.9 Reminders were sent every 2 weeks. Because physician response rates may improve if surveys are distributed in association with a recognised professional organisation,10 the survey was deployed by the AHS Renal Strategic Clinical Network (SCN), a clinician-led initiative within AHS that promotes and sustains evidence-informed patient care.11 Due to the purposive sampling of clinicians, who were using virtual consultation, survey content was anticipated to be familiar and of interest to respondents.9 Finally, instrument reliability was improved by piloting the survey content on three nephrologists working within AKC who were representative of the study population. The survey questionnaire is included in the online supplemental appendix 1.
Interviews and focus groups
Interviews were built on survey data, enabling themes to be explored in detail, thereby developing a richer narrative (online supplemental appendix 2).6 Potentially sensitive subjects such as comfort level with technology and perceptions of support from management might be explored more readily and openly. Interviews were conducted remotely via videoconferencing to facilitate social distancing and recording. Interviews with up to 20 clinicians were anticipated, or less if data saturation was reached. A semistructured approach was undertaken to ensure preidentified themes were covered while enabling deeper discourse. Interview questions were modelled after a framework covering experiences, feelings and knowledge.6 Focus groups enable a constructivist aspect of data collection by sharing opinions and facilitating consensus (online supplemental appendix 3).6 This aspect was anticipated to help fulfil a key study objective to inform best practices for routine virtual care procedures in AKC. To maximise participation and, hence, the validity of our conclusions, focus groups were conducted via videoconferencing in timeslots already established for divisional group activities with a well-documented record of high attendance. Focus group questions were less personal in nature and related to two themes requiring group consensus:
What clinical scenarios are best suited to the routine provision of virtual care?
How might AKC use emerging virtual care modalities, such as patient-facing smartphone apps and remote monitoring?
Transcripts were coded manually, and NVivo software was used to organise the data. Transcripts were sent to participants to ensure content validity.6 Separate focus groups were held for physicians and nurses. This decision was made for several reasons. Physician and nursing outpatient workflows in AKC do not overlap completely. Furthermore, it has been suggested that nurses’ perspectives on facilitators of and barriers to effective virtual care may differ from those of physicians.12 However, given the tendency for nurses to defer to physicians’ opinions and leadership on quality improvement initiatives,13 we anticipated that separate focus groups would facilitate a more valid discussion. Interview and focus group question scripts are included as online supplemental appendices 2 and 3.
Data analysis
Qualitative data collected during interviews and focus groups were analysed for each of the two groups under study (nephrologists and home dialysis nurses). We anticipated that two focus groups (one per study group) of approximately 6–8 people and up to 20 interviews would be sufficient to provide meaningful and transferable descriptions. Data analysis began during data collection via analytic memos. Qualitative data from focus groups and interviews were recorded and transcribed verbatim. NVivo, a software application designed to support qualitative data analysis, was used to organise the data and emerging codes. The first focus group/interview transcripts for nephrologists and nurses were read and reread to generate initial codebooks, which were iteratively refined throughout the analysis. Codes were categorised and analysed thematically, and data collected from nephrologists and nurses were analysed separately.
Data integrity and quality assurance
Several steps were taken to ensure the study findings accurately reflect clinicians’ perspectives on virtual care. First, multiple methods and data sources were used to mitigate concerns about conclusions being drawn from a single source. Data from surveys, interviews and focus groups contributed to an increasingly rich narrative and provided opportunities to explore issues that surfaced through overlapping themes identified in earlier stages of inquiry. Because responses may reflect a majority opinion, interview transcripts were reviewed for data saturation. It has been noted that smaller sample sizes may be feasible in qualitative research involving physicians due to a tendency towards conformity in opinions.10 Additionally, member checks were conducted with interview and focus group participants, who were asked to review transcripts to verify accuracy.6 The lead investigator also maintained field notes of thoughts and insights during interviews and focus groups to demonstrate reflexivity. Moreover, a nephrologist outside Alberta was asked to perform a peer review of conclusions to screen for researcher bias.14 Furthermore, generalisability of qualitative findings can be limited because social circumstances are constantly evolving. Transparency in data collection and analysis methods should demonstrate that this study’s findings are consistent with the data collected. The use of multiple methods contributed to the breadth of description and conclusions drawn. The surveys, interviews and focus groups included items for additional suggestions on important areas that had not been addressed. An attempt was also made to employ maximum variation by interviewing participants from different practice areas who received compensation via different reimbursement methods.6
Patient and public involvement statement
There was no involvement of patients or the public in this study.
Results
General characteristics of participants
A total of 46 nephrologists and 20 nurses completed the survey questionnaire. The characteristics of participants are summarised in table 1. Interviews were conducted with 12 nephrologists from across Alberta before data saturation was achieved. We also conducted two focus groups with 9 nephrologists and 15 home dialysis nurses at the University of Alberta.
Survey participant demographics
General perceptions regarding the utility of virtual care
Overall, clinicians support the ongoing utilisation of virtual care for outpatient consultation (table 2). Only 10% of nephrologists and 4% of home dialysis nurses indicated they would never offer virtual consultations in the future (online supplemental figure 1). Nephrologists’ and nurses’ views on facilitators of and barriers to routine use of virtual care were generally very similar. Surveys enabled a broad assessment of clinicians’ opinions, which are useful to inform policymaking. The interviews and focus groups enabled the exploration of survey trends and contributed to a richer narrative that informed the study recommendations. Indeed, interview and focus group data refined and on occasion, contradicted survey conclusions. As suggested by the literature review, basic technology acceptance models do not sufficiently explain clinicians’ attitudes regarding virtual care. Surprisingly, for practitioners accustomed to decision-making autonomy, AKC clinicians identified a need for consensus on methods for care delivery and outcome assessment while remaining wary of overly prescriptive policies. It appears that some policy direction from the College of Physicians and Surgeons of Alberta (CPSA) and the Canadian Medical Protection Association (CMPA) is required immediately, rather than later in the cycle. Consensus on quality metrics for outpatient care in nephrology is also needed. Opportunities to incorporate virtual care routinely have been identified, as have challenges to the traditional model of care. These findings mandate the revision of AKC outpatient clinic workflows to respect patient autonomy while enabling safe and effective care.
Supplemental material
Clinician consensus on indications for in-person and virtual consultation
Key themes
Four themes identified by this study best characterise clinician perspectives: logistics of routine virtual care integration; quality of virtual care and metrics; challenges and revisions to the therapeutic relationship; and clarification of regulatory and medico-legal policies for best practice. Codebooks of clinician quotes that informed these themes appear in the online supplemental appendix 4.
Logistics of routine virtual care integration
Clinicians in AKC had little experience using virtual care prior to the pandemic. Over half had typically engaged in virtual consultations with patients less than once a month. Clinicians had opinions about indications for and the modality of virtual care, as well as potential barriers and facilitators for routine use. Ongoing provision is specifically motivated by perceived patient demand and convenience. As shown in figure 1, survey data show that most clinicians perceive that patients prefer virtual consultations to in-person visits. Focus group data confirm this insight:
I’ve found almost universal acceptance of virtual care by patients. If we give them the choice, essentially, they’ll want to do their entire experience with us virtually (physician focus group).

Clinicians’ perceptions about patients’ preferences for virtual consultation.
Ultimately, clinicians feel strongly that decisions regarding consult modality should be the clinician’s prerogative, based on diagnostic requirements (figure 2). One paradox is the perceived need for some consensus among clinicians:
When there’s disparity, it creates problems. When one physician does things one way and another does things differently, it pulls patients apart: ‘I don’t want to see Dr. X because I have to come in. I want to see Dr. Y because he does everything over the phone’ (physician focus group).

Clinicians’ responses regarding decisions about consultation modality. AKC-N, Alberta Kidney Care-North.
Nephrologists predominantly used telephone consultation, and survey responses indicated intentions to continue doing so postpandemic in the majority of cases. However, in interviews/focus groups, both nephrologists and nurses expressed a strong interest in consulting with patients via videoconference rather than by telephone.
I prefer the Zoom. I think you get a little bit more out of that body language and conversation with video calls (Physician interview).
In-person can’t be beaten for a thorough assessment. As an intermediate tool, videoconferencing is far superior to just telephone assessment (Nurse survey).
During interviews, some clinicians highlighted several barriers to videoconferencing related to:
Patient capabilities/engagement: there were mixed opinions on patient preferences or abilities to use videoconferencing due to perceived issues with dexterity, comprehension or internet access. One nephrologist said, “I prefer the phone because I don’t think my patient population will be very adept with video consults and it would lead to longer appointments.” Another offered a different perspective: “I actually think people are using these things to talk to their grandkids or do their internet banking so it reflects more our attitude towards them than their attitude towards technology. The number that don’t have access is probably less than we think. So I think our misconceptions are a barrier as well.”
Availability of equipment: clinicians, particularly nurses, noted insufficient availability of videoconferencing equipment in AKC clinic spaces.
Administrative support: clinicians also highlighted administrative barriers, including a lack of technical support and troubleshooting assistance for clinicians and patients who encounter problems when scheduling, initiating and conducting videoconferences.
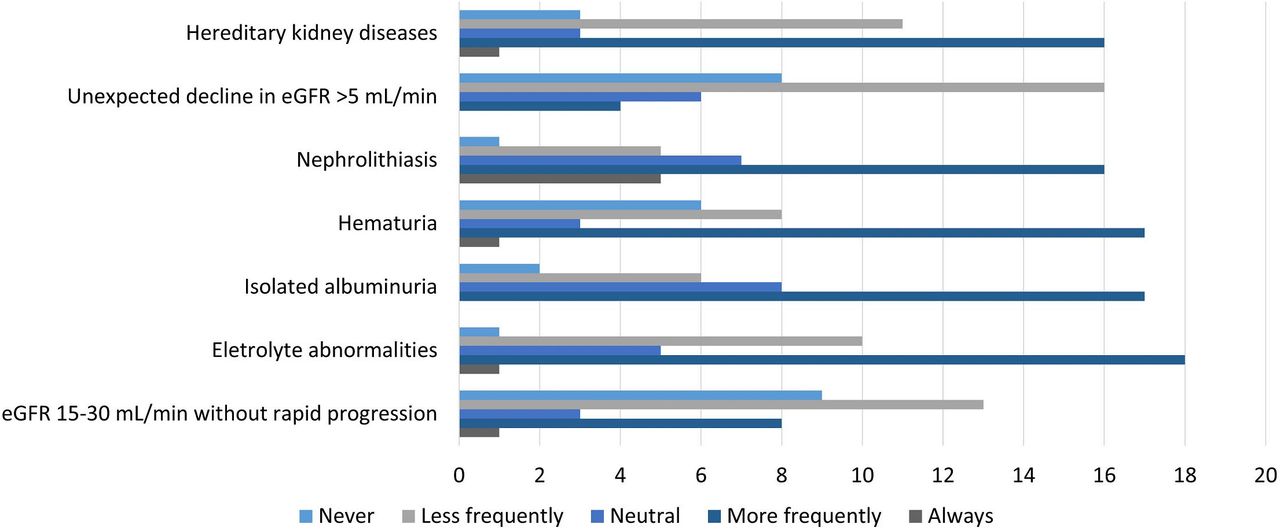
AKC clinicians felt that new patients should be seen in person as much as possible. In-person visits were also preferred to evaluate deteriorating renal function or to discuss transitions in care (dialysis initiation/transplantation assessments), procedural risk (renal biopsy) or therapeutic risk (immunosuppression initiation). It was, however, acknowledged that virtual consultation might be appropriate for some referrals (figure 3). These included patients with lower-risk presentations with mild renal insufficiency, haematuria or proteinuria with normal renal function and nephrolithiasis. Nursing staff perceived that in-person visits were more effective when teaching home dialysis patients’ self-care practices.

{kind=link}
{kind=link}
{kind=link}
Nephrologists’ survey responses regarding virtual consult indications by diagnosis.
Nephrologists and nurses had limited experience with the use of smartphone applications and expressed concern about additional data inputs and privacy risks. They acknowledged a potential role for patient-facing functions, including medication reminders or educational tools, and noted that research with the patient population is warranted. Many felt current AHS electronic medical records (EMRs) should be leveraged instead. They proposed a nephrology-specific patient portal with three elements:
Patient educational resources for self-care.
Reporting reference instruments for upcoming appointments, for example, symptom scales.
A tool to upload blood pressure measurements and medication lists.
We underuse our EMR with respect to opportunities to communicate with patients and to engage them in their care. We could have a nephrology-specific patient portal built where the patient has already been able to update and answer questions. Better preparation, but also information for the patient (Physician focus group).
Quality of virtual care and metrics
In this study, many clinicians perceived that virtual consultations improve access for patients who are unlikely to travel to Edmonton for initial visits or follow-ups, specifically due to distance or other accessibility issues. Nurses noted that virtual care improved access to assessment and teaching of rural patients, many of whom selected the home dialysis modality because of geography.
Virtual care allowed me to virtually teach a patient how to change his transfer set and mix antibiotics who otherwise would have had to drive hours to have this done (Nurse survey).
Over 60% of survey respondents noted that they spent less or the same amount of time with patients in virtual consultations; however, almost half of the respondents noted a concurrent increase in preadministrative work or postadministrative work, and an increased volume of patient calls between appointments. The absence of reliable blood pressure data and medication reconciliation were frequently cited as time-consuming aspects of virtual consultations. In interviews, nephrologists felt they were not seeing more patients since the transition to virtual care. Clinic templates were unchanged, so it was not apparent to many clinicians that virtual care improved wait times to see a nephrologist (online supplemental figure 2). A majority felt that virtual consultations impaired the quality of assessments (online supplemental figure 3). This was particularly true for physicians who had been practising for more than 10 years. In interviews, it was clarified that this specifically referred to the inability to perform a physical exam or assess visual cues, given the physicians’ tendency to use telephone consultations.
Supplemental material
Supplemental material
I find seeing someone’s face is so important. You miss visual cues due to poor health, like skin color (Nephrologist interview).
Nephrologists frequently expressed concerns about ‘missing something’.
Specifically, they frequently articulated a major fear of misdiagnosing volume overload/congestive heart failure. “It’s really about the volume status. I can’t tell on the phone what’s fluid or not” (Nephrologist interview).
Measures are required to evaluate the accuracy of these concerns. Published guidelines outline a general framework for virtual care quality improvement measures,15 however, reporting in AKC is limited. Potential metrics were suggested by clinicians in this study.
Outcome measures: patient satisfaction was a frequently suggested measure. Hospitalisation/emergency room visit rates were implied, given the concern with virtual volume assessments, as were dialysis-related complications of infection and home modality failure. Biometric data targets, specifically blood pressure control, as well as prescription rates for risk-reduction measures, including statins, antihypertensives and diabetic medications, were also suggested.
Process measures: these measures included wait times to see a clinician and visit attendance rates, stratified by location to assess access for remote-dwelling patients.
Balancing measures: these included total clinical encounter time, including preclinic and postclinic administrative work, administrative support staff satisfaction and frequency of patient-initiated contact.
During an interview, one nephrologist noted the ambiguity in current quality measurement and the need for change:
We prioritize efficiency so highly in the clinical encounter and I’m not sure that’s the most patient friendly approach.
Addressing the redefined therapeutic relationship and professional roles
Patient preference and convenience were cited as both motivations for and metrics of virtual care. However, the data reveal a profound awareness of—and in some cases, discomfort with—evolving roles in the clinician-patient relationship. Physicians noted uncertainty in relying on patients to relate vital information without corroborative physical examinations:
I worry because it’s a lot on them, and do they really know when to reach out to us? I don’t have a great sense of what the general public’s knowledge is and how good they are at this. I feel the public needs more training in terms of what information to have available when the doctor calls you (Nephrologist interview).
Nephrologists felt that prolonged periods of virtual care had enabled them to identify a subset of patients who could be monitored virtually without apparent negative consequences. This led some to conclude that the current tendency to automatically schedule in-person visits for new referrals should be revisited. They also noted implications for consultation criteria, whether virtual or in-person. During an interview, one nephrologist articulated these implications:
How often should I see someone in-person then? Should I say every two years? Do you even need to see the nephrologist in that case?
Notably, nephrologists and nurses disclosed that patients tended to take a more informal approach to virtual consultations than in-person visits. Some questioned the level of engagement/preparedness of patients for these encounters.
Sometimes, I’ve called patients and they’re driving or at work. I had a patient who was playing video games. I think there should be very clear expectations, so people know this is an official appointment and not just a convenience (Nephrologist interview).
Clarifying uncertainties in best practice policies
In general, clinicians’ opinions in this study reinforced the multifaceted technology acceptance model suggested by Gagnon et al.8 The ‘lifecycle’ hypothesis of innovation states that regulatory and legal policies must be supported at later stages to sustain innovation.16 AKC physicians, however, described a need for clear direction from regulatory (ie, CPSA) and medico-legal organisations (ie, CMPA) prior to developing best practices themselves. Pathways developed locally by AKC may be rendered obsolete if contradictory directives from these organisations are later imposed. Physicians’ concerns included:
Validity of virtual consults: there is a need for a directive on whether virtual visits will be considered adequate by regulators or if a standard for in-person visits will be mandated. This will have implications for outpatient triage pathway development.
Medico-legal risk: physicians expressed concerns regarding liability and conflict resolution in instances of disagreements with patients regarding consultation modality.
Privacy legislation: although data security or privacy are cited as barriers to virtual care,17 many AKC clinicians perceived a lack of patient concern regarding the privacy of communication via telephone or videoconferencing. Directions regarding the recommended virtual platform are desired from the CPSA. Fee-for-service physicians expressed financial concerns if videoconferencing platforms require replacement.
“I’m still not convinced the government won’t pull the rug out from under us at some point and make virtual billing codes unprofitable” (Physician focus group)
Discussion
With the recent experience from the pandemic, it is very clear that virtual consultation has come to stay as an integral part of the ambulatory care continuum in all facets of chronic disease care. Adoption of this innovation on a large and sustainable scale can significantly alter clinic workflows and impact quality of care and patient safety. In several medical disciplines, virtual consultation improves access to care without affecting diagnostic accuracy.18 However, people with kidney disease often have complex presentations requiring longitudinal care, rather than solitary encounters.19 Self-awareness of renal disease is not prevalent in the general population,18 and an inadequately supported, patient-directed care model may expose an inherent vulnerability. In this mixed-methods study, we evaluated the requirements for the safe and effective integration of virtual outpatient care in one of the largest kidney care programmes in Canada. The key findings were that healthcare professionals in general were in support of the use of this modality of care but expressed important concerns about the logistics for integration, quality assurance, impacts on the therapeutic relationship between patients and care providers and the need for clarity on regulatory policies and medical-legal frameworks.
What are the implications of these findings? The transition to virtual care provides AKC with an opportunity to increase patient input in outpatient care delivery. This requires reimagining the traditional provider-led paradigm, as well as integrating emerging technologies that improve patient access to care. AKC clinicians have a responsibility to reconcile these requirements and enable effective patient participation. The themes identified through this mixed-methods study suggest essential components of a blueprint for the effective and safe integration of virtual care in AKC (online supplemental figure 4).
Supplemental material
Leadership should petition intermediary bodies, such as the CPSA/CMPA, for clarity on several policies. Clinicians specifically required minimum standards for in-person visits and recommended videoconferencing platforms prior to investment in revamped triage pathways and equipment purchase and training.
Revise current outpatient clinic triage practices. This study identified clinician recommendations on indications for virtual care. AKC nephrologists and nurses support some common standards of practice that are not excessively prescriptive. Table 2 outlines some basic principles that satisfy these requirements.
As virtual care may reduce AKC wait times modestly, and indeed, not noticeably to many clinicians, alternative strategies to improve this outcome should be pursued. Previous works in the field within and outside of Canada did note that innovations such as e-referral and online referral guidelines have not impacted referral volumes or wait times. However, during the pandemic, nephrologists occasionally identified patients who did not require an appointment or longitudinal follow-up. An ‘advice only’ triage category should be created. Consults not deemed to require a patient appointment would be assessed by a rotating physician or nurse practitioner, with advice provided directly to the referring doctor. Clinician workflows and booking templates should also be reviewed, perhaps by direct observation study, to identify inefficiencies.
Develop a nephrology-specific patient portal using the current EMR. This may address several concerns identified in this study:
Clinicians noted considerable delays in collecting biometric data and clarifying medications. This information could be uploaded in advance by the patient and their pharmacy.
Clinicians perceived a lack of patient understanding/preparedness regarding the significance of the appointment. Educational resources should be available on the portal to help patients with self-care (eg, the correct technique for blood pressure measurement).
Clinicians had challenges obtaining reliable historical information on virtual visits. Structured previsit questionnaires completed online would give the consultation structure and context while enabling patients to prepare for their appointments. Several symptom questionnaires have predictive value for adverse events that may be superior to commonly used physical examination methods. Clinicians were particularly concerned about the risk of volume overload. The Kansas City Cardiomyopathy Questionnaire is a 12-item symptom scale that predicts congestive heart failure exacerbation factors, hospitalisations and mortality.20 A positive result could prompt an expedited in-person visit. Paper versions of these tools could also be distributed to those without internet access.
Clinicians should articulate requirements for effective virtual visits to patients, emphasising that they are official clinical encounters. During the first visit, it might be useful to formalise the expectations of both parties in a contract. Discussion should incorporate patient requirements for the modality of consultation.
There is significant interest in expanding the use of videoconferencing postpandemic. AKC-N should invest in videoconferencing equipment for clinics and train patients/support staff on how to initiate appointments.
Endpoints, such as hospitalisation, specifically evaluated in an outpatient population at high risk of healthcare utilisation, did not show the impacts of virtual care. It is probable that more immediately related endpoints are required to show effects. AKC should partner with the SCN to study markers more closely aligned with virtual care delivery, as suggested by this study.
Of note, this study has a few limitations worthy of note. First, a discrete choice experiment might facilitate a more accurate and unbiased measurement of clinicians’ preferences and attribute values versus a standard survey.21 However, this methodology is beyond the scope and resources of the investigator and the research parameters. Second, the generalisability of the findings is limited in scope, as the study was conducted in a single nephrology programme in Canada, so conclusions may not apply to other provinces or settings with different regulations pertaining to virtual care. Third, data collection occurred during a pandemic. It is possible that clinicians’ motivations to use virtual care may change in the future when social distancing measures are lifted. The ethics approval parameters did not permit the collection of patient identifiers, hence multivariate analysis of data sets could not be performed. The interrupted time series analysis, therefore, can only imply an association between virtual care and outcomes. Finally, due to limitations related to time, only clinician perspectives were considered. Patient and caregiver perspectives may greatly influence virtual care decisions and should inform future studies.
Conclusions
Our findings demonstrated that clinicians support the use of routine virtual care. Clinicians’ opinions on implementation requirements emphasise logistics for routine virtual care integration, quality of care delivered, impacts on the therapeutic relationship and regulatory policy clarification. Further work is required to clarify the impacts of virtual care for specific population demographics based on geography (rural vs urban) and age (elderly population) in the post-COVID-19 era and to integrate patient perspectives into this care model. Further work is also needed to determine patients’ perceptions about this model of care. This study was, by design, focused on clinicians’ attitudes and preferences. It is apparent that several assumptions are being made that require urgent clarification with patients. These include confirmation regarding their preferences on consultation modality, willingness to use or accept training/support for videoconferencing, the utility of smartphone applications and desired content and functionality of an EMR-based patient portal. Finally, it must be reiterated that this study was conducted during a pandemic. Data set review should be repeated under non-pandemic circumstances. Clinician opinions on the value of virtual care should be revisited. A discrete choice experiment would be a more robust methodology for this analysis.21 The use of virtual care has identified a need to revise traditional outpatient care paradigms. The recommendations of this study are intended to best support clinicians and patients in this endeavour while providing the safest and most effective care possible.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the University of Alberta Research Ethics Board (Pro00109399). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the Alberta Health Service Medicine Strategic Clinical Network for their support with the organisation and conduct of the focus groups and project management. The significant contributions of the care providers (nephrologists and nurses) who attended the sessions are greatly acknowledged. We also thank Sophanny Tiv (University of Alberta) for assisting with the figures and charts.
Footnotes
X @StephanieTh11
Contributors We were guided by the International Committee of Medical Journal Editors (ICMJE) guidelines in authorship selection. MC is responsible for the inception and design of the project and prepared the initial draft of the manuscript. ST, SK, FY, DZ, TJS and AKB provided methodological input and/or involved in the acquisition, analysis, interpretation and reporting of data. All authors read and approved the final version of the manuscript before submission. MC is the guarantor of the study.
Funding The work has received funding support from the Division of Nephrology, University of Alberta (Kidney Health Chair Funds) and AMGEN Incorporated Clinical Innovation Grant. The funders had no role in the design, collection, analysis, interpretation, writing or submission of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.