Article Text

Abstract
Introduction Informed decisions to enrol in the clinical investigations of Alzheimer’s disease and related dementias (ADRD) require careful consideration of complex risks and uncertain benefits. Decisions regarding whether to receive information about biomarker status are complicated by lack of scientific consensus regarding biomarkers as surrogate endpoints for Alzheimer’s disease and how information about individual risk should be evaluated and shared with research participants. This study aims to establish stakeholder consensus regarding ethically optimal approaches to sharing individual results with ADRD research participants.
Methods and analysis This Delphi consensus-building study consists of multiple online surveys conducted with Alzheimer’s disease research experts, including neurologists, neuropsychologists, ethicists, research oversight specialists and clinical trialists. Panellists will be administered questionnaires developed from a synthesis of researcher- and participant-endorsed considerations and decisional needs identified in published literature and a decisional needs assessment conducted with support from an Alzheimer’s Association Research Grant. Panellists will also be asked their views on the content and implementation of processes for sharing individual research results. ≥75% agreement will be required to achieve consensus. Response rates, level of agreement, medians, interquartile ranges and group rankings will be analysed. Following each round of data collection, our research team will undertake qualitative content analysis of open-ended responses.
Ethics and dissemination Ethical approval will be obtained from the Cleveland Clinic Institutional Review Board (Study Number 22–766). Delphi panellists will receive participant information sheets describing the study before agreeing to participate in the Delphi process. Results from the data we anticipate will be generated through this research and will be submitted for peer-reviewed journal publication and presentation at international conferences.
- MEDICAL ETHICS
- Clinical Trial
- Dementia
- Dementia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A modified Delphi technique will be used with online interaction among participants, using iterative rounds of questionnaires to develop consensus about recommendations for returning results to participants in Alzheimer’s disease and related dementias (ADRD) research.
This study incorporates input from ADRD research participants partners through surveys and interviews to inform the study design and panellists, enhancing the relevance and applicability of the study outcomes to the target population.
Compared with the traditional Delphi methodology, the online modified Delphi process enables inclusion of participants from a wider range of professional disciplines and geographic diversity, ensuring representativeness of our expert sample.
While the study involves a diverse panel of experts, it excludes ADRD research participants as panellists due to the specialised expertise required, potentially limiting lived experience representation.
Introduction
Clinical investigations into Alzheimer’s disease and related dementias (ADRD) involve complex ethical challenges, particularly concerning the sharing of individual research results with study participants. The emergence of biomarker-based diagnostic tools has underscored the importance of addressing decisional needs and ethical considerations surrounding the return of research findings to individuals enrolled in ADRD studies. Despite growing awareness of these challenges, a systematic and multidisciplinary approach to establish expert consensus on best practices for sharing individual research results remains lacking.
Biomarkers, such as beta-amyloid, tau, amyloid imaging and the APOE genotype, play an increasingly central role in clinical research and evolving diagnostic criteria.1 The National Institute on Aging and the Alzheimer’s Association convened workgroups to generate guidelines for defining ADRD biologically rather than based on clinical symptoms, recognising the importance of biomarkers in diagnosis. The 2023 Revised Criteria for Diagnosis and Staging of Alzheimer’s Disease drafted by the Alzheimer’s Association Workgroup proposes that a single abnormal ‘Core 1’ biomarker, such as amyloid positron emission tomography or cerebral spinal fluid (CSF) assays, is sufficient to diagnose Alzheimer’s disease.2 The scientific capability of detecting CSF, imaging or genetic (nonfamilial) biomarkers for Alzheimer’s disease in cognitively unimpaired patients has paved the way for earlier detection and potential pre-symptomatic treatment of Alzheimer’s disease.3
These biomarker developments of the last decade underscore the centrality of biomarkers to Alzheimer’s disease in clinical and research settings. Consequently, more cognitively unimpaired people are involved in Alzheimer’s disease research studies where biomarker levels are measured before symptom onset. Existing literature highlights the variability in practices and perspectives regarding the return of research results to ADRD study participants. Empirical research has shown that Alzheimer’s disease biomarker research participants want to know their research results4 5 regardless of the availability of disease-modifying treatment.5 While participants often express a desire to receive individual research findings, researchers and clinicians face challenges in determining the types of information to share, the appropriate timing, and the necessary support and counselling for participants. Communicating limitations in clinical utility and the predictive power of the individual research results pose additional challenges.4 6 7 Importantly, empirical research has indicated that biomarker result sharing is not correlated with short-term, adverse psychological impact on the research participant.8 Research participants view learning biomarker research results as useful to know,9 though there may be social stigma associated with a potential Alzheimer’s disease diagnosis.10 Existing guidelines and policies do not provide empirically driven, specific recommendations for sharing clinical risk information and risk communication strategies applicable to sharing ADRD research results.11 This study seeks to address these gaps by fostering expert consensus on key aspects of the research results sharing process.
The primary aim of this Delphi study is to establish expert consensus on recommended approaches to sharing individual research results with ADRD research participants. The specific objectives include the following:
Reaching consensus on the types of research results that should be shared with participants.
Determining the appropriate timing and methods for disclosing individual research findings.
Developing recommendations for decision support and counselling processes to accompany the return of research results.
Methods and analysis
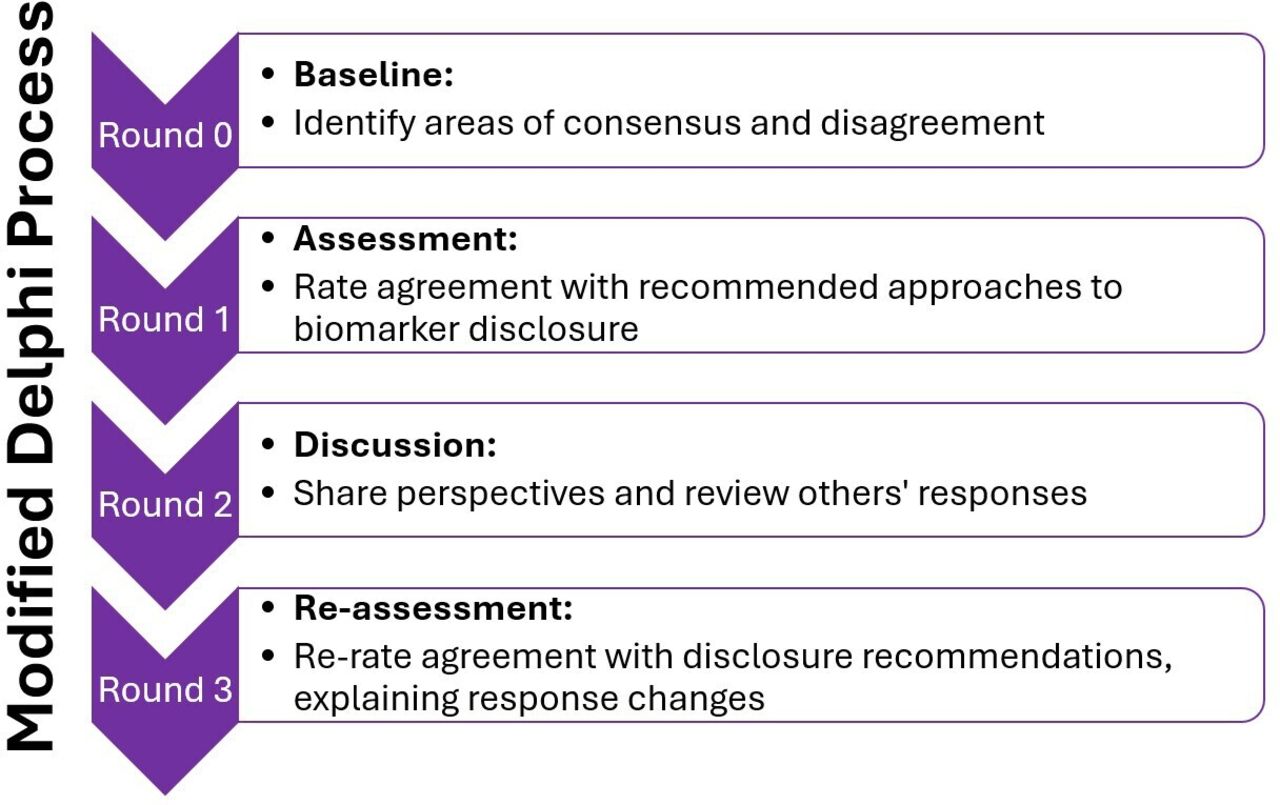
The Delphi technique aims to develop an ‘expert’ consensus through iterative rounds of structured questionnaires.12 Interaction among participants distinguishes the modified Delphi from the traditional Delphi methods.13 We chose an online, modified Delphi process as it offers anonymity and enables participation from a demographically and geographically diverse group of experts. We developed this protocol in accordance witgh the Recommendations for the Conducting and REporting of Delphi Studies (CREDES) (see online supplemental figure 1). Given the importance of multidisciplinary engagement and representativeness of the expert panel, our research team identified this approach as the most appropriate methodology for generating consensus on standards in research. For the purpose of this study, our Delphi process will consist of one baseline round (Round 0) and three subsequent rounds of assessment, discussion,and reassessment (Rounds 1, 2 and 3, respectively) (figure 1).
Supplemental material

Progression of Delphi rounds.
Patient and public involvement
Input from ADRD research participants and their trusted others (legally authorised representatives, study partners or caregivers) will be elicited at multiple stages of the research process. First, a survey and semistructured interviews were conducted with Cleveland Alzheimer’s Disease Research Center participants and their study partners to establish preferences and decisional needs related to return of research results. A summary of findings from this study as well as a systematic review of publications describing the perspectives of Alzheimer’s Disease Research Centre (ADRC) research participants and their trusted others regarding research results sharing will be provided to Delphi panellists to inform their contributions. However, research participants and patients are not included as Delphi panellists due to limitations imposed by the expertise required to address the research questions, limiting the lived experience represented on this panel.
Research steering committee
A research steering committee will guide and inform the development of the Delphi questionnaire. The research steering committee will be composed of an ethics researcher, two ADRC directors, a bioethicist specialising in neuroethics and a behavioural neurologist clinician researcher with experience conducting clinical trials in ADRD. This committee will be responsible for providing input on participant selection, Delphi questionnaire development and synthesis of recommendations and findings developed through the Delphi process.
Participant selection
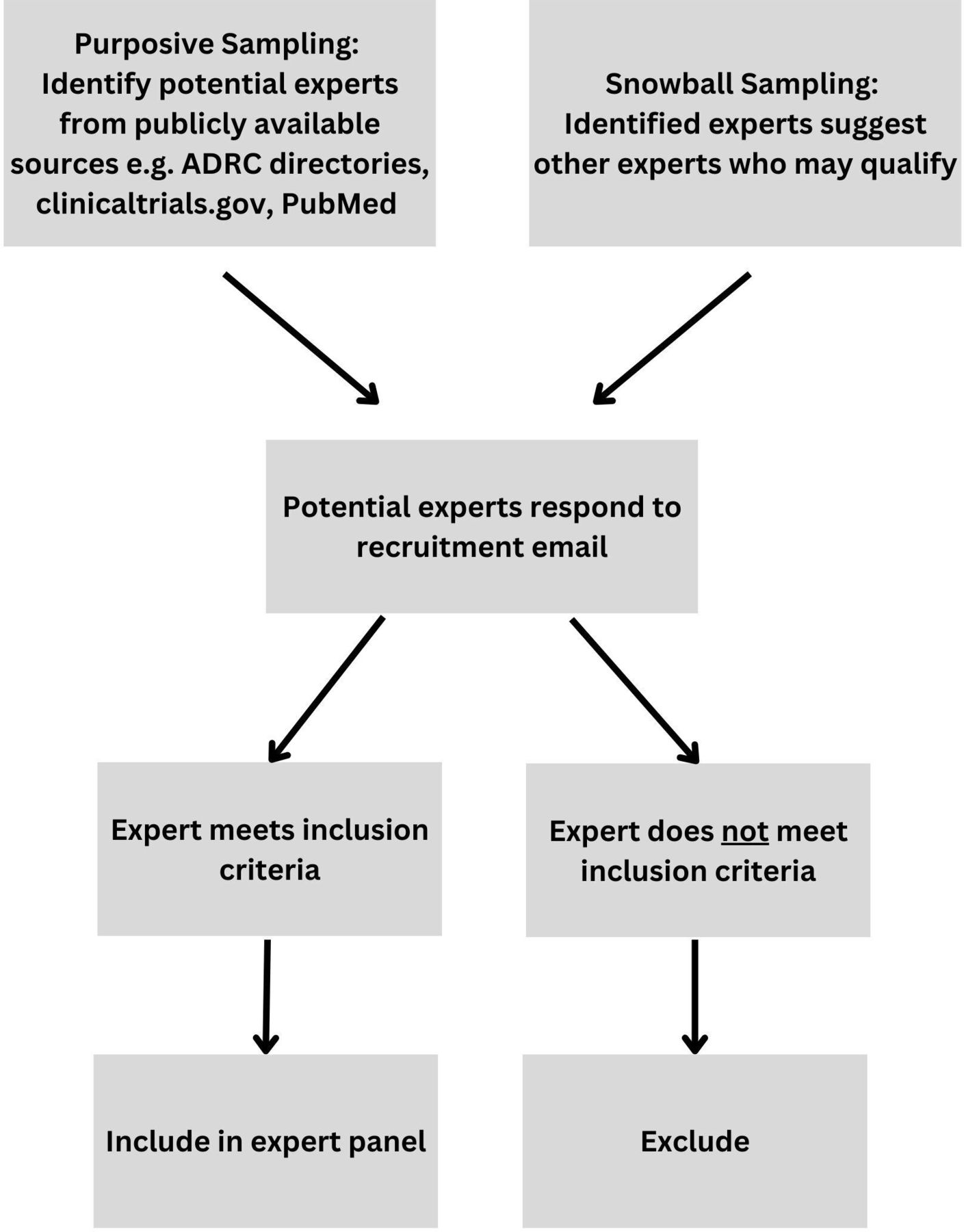
Purposive sampling of panel members representing relevant professional stakeholders will be conducted. A snowballing sampling approach will also be used to recruit panellists, asking the purposive sample of panellists to suggest names and contact information for other experts with relevant experience. Our selection of panellists will be guided by current practices for sharing individual research results with Alzheimer’s disease study participants as identified by Roberts et al.14 As different stakeholders may prioritise different aspects of informed consent based on personal areas of expertise and research experience, it is important to select a diverse panel of participants. To this end, our interdisciplinary panel will consist of Alzheimer’s disease experts who have experience in clinical practice and/or research pertaining to Alzheimer’s disease, including neurologists, neuropsychologists, geriatricians, genetic counsellors, ethicists, research oversight specialists and clinical trialists. Part of our expert eligibility criteria will be established through a screening questionnaire that will determine potential participants’ level of experience and expertise in their respective fields. We will also include questions specifically aimed at identifying potential participant conflicts of interest to minimise selection bias.
The inclusion criteria for panel participants will be as follows:
More than 3 years of professional experience in clinical research, clinical care, research ethics or research oversight related to Alzheimer’s disease.
Expertise in clinical research/care will be defined to include board certification or other credentialing in behavioural neurology, gerontology, geriatric psychiatry, neuropsychology, genetic counselling or another relevant discipline and direct involvement in research and/or clinical care for patients with ADRD.
Expertise as a research oversight specialist as experience reviewing at least one protocol related to ADRD or another brain disorder.
Expertise in research ethics will be defined as published scholarship, participation in task forces/committees and other academic work related to ethical issues in research or clinical care for patients with ADRD.
Able to read, write and converse in English.
Able to access a smartphone, tablet or laptop with Wi-Fi access.
Participants will be excluded if they do not meet inclusion criteria, if they present a conflict of interest, or at the discretion of the research steering committee.
Recruitment
Potential panellists will be identified through a multifaceted approach, outlined in figure 2 including review of professional directories and through snowball sampling.

{kind=link}
{kind=link}
Delphi recruitment process.
Alzheimer’s disease experts will primarily be identified using ADRC directories throughout the USA. Using publicly available information, we will select both ADRC directors and clinical core leaders to ensure a diversity of expertise related to clinical practice and research. Ethicists and research oversight specialists will be identified through publicly available information found on various professional directories and search tools such as the NIH’s RePORTER tool. A snowball sampling approach will also be used to further recruitment of panellists, asking already identified experts to suggest names and provide contact information for other relevant stakeholders in the field.
Participant level of expertise in the field will be verified through a review of prior experience with Alzheimer’s disease research. After potential panellists are identified, an invitation to participate will be sent out via standardised email template. Prospective panellists will be provided with an information sheet with comprehensive materials outlining the study design, objectives and a description of anticipated tasks and estimated time required.
Panel size and composition
There is a lack of consensus on what constitutes an adequate number of Delphi panel participants.15 Following guidelines set forth by Khodyakov et al, we aim to empanel approximately 45 participants, without setting an upper limit.13 We aim to include approximately 60% clinical researchers and clinicians and 40% ethicists and/or research oversight specialists. To achieve our minimum sample size and participation rate, we will identify and contact at least 120 potential participants. Oversampling panellists representing each area of expertise will optimise the Delphi process while accommodating possible attrition between rounds.
Development of Delphi questionnaire
The Round 0 questionnaire was developed with input from a research steering committee consisting of behavioural neurologists with experience leading observational and interventional research studies, bioethicists and a neuropsychologist.
Literature review
Delphi questionnaire development will be informed by a systematic review of decisional needs and psychological contraindications to sharing ADRD biomarker results and recommendations for disclosure and counselling related to ADRD biomarker results. We conducted a targeted literature review of existing guidelines and qualitative studies characterising decisional needs of ADRD research participants related to receiving individual biomarker results. We searched four databases (PubMed/MEDLINE, EMBASE and PsycINFO) to identify relevant published studies using a SPIDER search tool framework published separately.16
Definition of consensus
We will define consensus as the proportion of participants who rate they agree with each item. If at least 75% of participants rate an item as 5, 6 or 7 (agreement), we will consider consensus reached. If we reach consensus about an item in Round 1, we will remove the item from subsequent rounds to reduce participation burden. We will notify participants when we reach consensus about an item. Items that do not reach consensus by the end of Round 3 will be dropped. In Round 1, if 50–75% of participants rate an item as 5, 6 or 7, we will consider this inconclusive and include the item in subsequent rounds. If less than 50% of participants rate an item as 5, 6 or 7 in Round 1, the item will be dropped.
Education for panelists
Prior to Round 0, the Delphi panellists will receive an informational sheet highlighting current research standards, consensus statements and recommendations for how to best counsel patients and research participants about biomarker results. Following data analysis of each round, and prior to panellists beginning the proceeding round, we will generate feedback reports containing aggregated quantitative and qualitative data. In these feedback reports, we will summarise key reasons for agreement and disagreement, as well as communicate results for items that failed to reach consensus and provide a basic summary of items that reached consensus and were subsequently removed. To prevent bias, the research steering committee will evaluate all preround materials before they are shared with participants.
Rounds
The Delphi method relies on iterative data collection.13 Consequently, multiple rounds will be conducted to achieve expert consensus. We will adhere to guidance from Khodyakov et al for the online modified Delphi approaches to engaging patients in research guideline development.13
Our consensus building Delphi method will consist of multiple rounds of online surveys administered to our expert panellists. We will conduct one baseline round (Round 0) where we will establish a baseline of areas of consensus and disagreement and three subsequent rounds of assessment, discussion and reassessment (Rounds 1, 2 and 3, respectively) (figure 1).
Participants will rank their agreement with statements using a seven-point Likert scale. Response rates, level of agreement and overall consensus will be analysed. Following each quantitative round of data collection, our research team will undertake qualitative content analysis of any open-ended text responses and discussion interactions.
Round 0
The purpose of Round 0 is to establish a baseline for existing areas of consensus and disagreement between panellists. All panellists will be provided with a summary of existing consensus statements and recommendations on best practices for counselling patients and research participants about biomarker results. Expert participants will rank their agreement with statements about decisional needs of research participants and study partners, screening for psychological contraindications to sharing biomarker results, decision support needed when disclosing ADRD research results and considerations for follow-up actions after sharing individual results. We will also include space for open-ended responses to solicit any additional recommendations that experts may recognise as valuable. Both ranked and open-ended responses to Round 0 will be used to inform the quantitative portions of the proceeding Round 1 of the Delphi.
Round 1 and subsequent rounds
In Round 1, panellists will rank their agreement with statements about the decisional need of sharing individual research results with research participants. Rankings will be structured as seven-point Likert scales. In Round 2, participants will compare their Round 1 ratings to those of other panellists via a summary of interim results in which other panellists are classified only by area of expertise. The results will be analysed for agreement and degree of consensus to determine group consensus on priorities for informed consent support. In Round 3, panellists will then rerank their agreement with statements regarding decisional needs and features of decision support, explaining response changes.
Data analysis
Quantitative data analysis
We will use descriptive statistics following Rounds 1 and 3 to determine when consensus has been reached for individual statements. In Round 0, we will calculate the proportion of agreement; however, all items above the threshold will be included in Round 1. We will only use the proportion of agreement in Round 0 to provide a holistic understanding of participants’ perspectives about each item. Items with below 50% of agreement will be heavily revised or removed by the research steering committee following the end of Round 0. Following Rounds 0, 1 and 3, response rates, level of agreement, medians, interquartile ranges and group rankings will be analysed.
Qualitative data analysis
Following each round of data collection, our research team will undertake qualitative content analysis of open-ended responses.17 We will code free-text survey answers to describe how participants express qualities or viewpoints related to their quantitative rating of each item. Throughout data analysis, we will use methods that maximise trustworthiness, as defined by Graneheim and Lundman to promote credibility, dependability and transferability.18
Coders will read through all the responses to become familiar with the content. During the coding process, each coder will identify and label meaning units relevant to agreement or disagreement with each item, generating a coding list. We will code in vivo as often as possible to avoid loss of meaning and conduct coding checks of responses to ensure no relevant concepts were left unlabeled. After each coding session, coders will complete an audit trail and a reflective memo about contextual factors apparent from the content (such as differences in interpretations of an item). The analytic team will meet regularly to discuss ongoing data analysis and ensure consistency.
We will use triangulation techniques to integrate qualitative and quantitative data.19 Immediate analysis of qualitative data will inform the interpretation of quantitative results and vice versa. We will develop a comparative framework to systematically compare quantitative scores with key qualitative themes. For example, quantitative items with high agreement will be cross-referenced with qualitative feedback to identify supporting narratives and nuances. Discrepancies between quantitative and qualitative data will be identified and addressed. For instance, if a quantitative item shows high agreement but qualitative feedback indicates significant concerns or divergent views, this will trigger review and potential revision of the item. Iterative feedback loops will be integrated where findings from one round inform the next. Integrated findings will be presented in feedback reports, highlighting areas of convergence and divergence to participants. To ensure comprehensive reporting, we will align qualitative codes with quantitative items, validate quantitative themes using qualitative data and conduct contextual analysis to understand the reasons behind quantitative ratings. We will maintain thorough documentation of the triangulation process, including decision-making rationales and integration steps, to enhance credibility.
Feedback reports and recommendations
Following data analysis, we will generate feedback reports for participants containing aggregated quantitative and qualitative data and a summary of key reasons for agreement and disagreement. In feedback reports, we will communicate results for items that fail to reach consensus and provide a basic summary of items that reached consensus and were removed. After consensus has been analysed, we will synthesise a list of recommendations for ethically optimal approaches to sharing individual research results with ADRD research participants from consensus statements. The final draft of recommendations will be approved by the research steering committee and an external source of validation. This approach ensures that the study’s outcomes are practically applicable and ethically sound, reflecting the comprehensive insights gained from both quantitative and qualitative data.
Discussion
This protocol details the design of a study using the online, modified Delphi process to establish consensus regarding priorities for decision support for ADRD research participants and key features and content of ethically optimal biomarker results sharing processes. The results of this study will be used to develop consensus-based recommendations for ethically optimal approaches to sharing individual research results with ADRD research participants. Our reporting of results will include statements on which our Delphi panel did not achieve consensus.
The Delphi technique is appropriate for developing consensus between diverse stakeholders because of its ability to offer anonymity to participants and minimise bias. Due to the multidisciplinary nature of ADRD management and ADRD research, guidelines often require input from clinicians, researchers, ethicists and other professional disciplines who may be attentive to different aspects of the process of sharing individual research results. The online, modified Delphi process allows us to empanel a broader range of stakeholders and experts from geographically diverse institutions and organisations, where traditional Delphi methods would not.
The recommendations developed and validated through this Delphi process will aid in establishing consensus-based guidelines to improve research processes for return of valued information to ADRD research participants. These guidelines may help to reduce researcher hesitations regarding returning individual results and enhance standardisation of research practices. Identifying research results sharing practices for which there is not currently consensus will help to direct future guidelines development. We expect the results of this study to aid in establishing new standards for sharing individual research results with ADRD research participants, cultivating increased trust in research and enhancing the recruitment and retention of research participants.
Ethics and dissemination
Ethics approval has been obtained from the Cleveland Clinic Institutional Review Board (Study Number 22–766). Delphi panellists will receive participant information sheets describing the study before agreeing to participate in the Delphi process. Results from the data we anticipate will be generated through this research will be submitted for peer-reviewed journal publication and presentation at international conferences. Delphi panellists will be invited to contribute to an additional manuscript outlining recommendations developed through this process after expert and stakeholder validation.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @DementiaUpdate
Contributors LRS conceived the protocol with input from MZ, AJL, KM, BT, PJF and JL. LRS took the lead in writing the manuscript, with support from VR and HSW. All authors provided critical feedback and helped shape the research and manuscript. LRS is responsible for the overall content as guarantor.
Funding This work was supported by the Alzheimer's Association Research Grant (AARG-22-974462).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.