Article Text

Abstract
Objective Reductions in paediatric unscheduled healthcare utilisation were seen during the COVID-19 pandemic, with concerns around their impact on children’s health. The reasons for these changes are not well described. This review aims to explore the factors reported by parents that influenced their decision-making around accessing paediatric unscheduled healthcare during the COVID-19 pandemic.
Design Mixed methods rapid review and thematic synthesis based on the Enhancing Transparency of Reporting the Synthesis of Qualitative research framework.
Data sources MEDLINE, Embase, Web of Science, PsycEXTRA, PsycINFO, Global Health, Global Index Medicus, Dissertations and Theses Global, Google Scholar and OAISter. Studies published from January 2020 to July 2023 were included.
Eligibility criteria for selecting studies Qualitative, quantitative and mixed methods studies that assessed the perspectives of parents on decisions to access or delay or avoid accessing paediatric unscheduled healthcare during the COVID-19 pandemic.
Data extraction and synthesis Nvivo 14.23.0 was used to code results the of the primary studies and develop themes, following a thematic synthesis approach.
Results Twelve studies were included, all from high-income settings, mainly in Europe. The studies were conducted across varying times and levels of COVID-19-related restrictions. The principal descriptive themes identified were (i) concerns about COVID-19 infection, (ii) balancing and navigating risks, (iii) perception of healthcare service status and conditions and (iv) perception of information and advice. These were developed into analytic themes to further describe the decision-making process.
Conclusions Parents balanced a range of risks, concerns, advice and responsibilities when considering accessing paediatric unscheduled healthcare during the COVID-19 pandemic. External sources of advice and information were important; misconceptions around public health advice may reflect the multitude of information sources and the rapidly changing circumstances of the pandemic. Public health policy and planning should consider parent perspectives when developing measures to ensure equitable access to appropriate paediatric healthcare services.
- COVID-19
- PUBLIC HEALTH
- Health Services
- PAEDIATRICS
- Health Services Accessibility
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This mixed methods review on unscheduled paediatric healthcare utilisation decision-making directly explored parent perspectives, which are an important but sometimes overlooked consideration.
A comprehensive and systematic search strategy was used, but with limitations due to resource constraints, such as limiting to the English language and screening being carried out by a single reviewer.
Thematic synthesis was applied, including inductive coding and the use of participant quotes to ensure the findings remained grounded in the context of the primary studies.
An explicit quality appraisal process was applied, which included the use of sensitivity analysis. This method and its rationale are transparently described, although the optimal approach in mixed methods or qualitative synthesis is debated.
This review considered unscheduled healthcare as a whole undivided system, but there was a potential bias in included studies towards the emergency department setting. There was also a bias in included studies towards high-income countries in Europe.
Introduction
Unscheduled healthcare is healthcare that is usually provided with less than 1 day’s notice through services such as emergency departments (EDs), general practitioners (GPs) and out-of-hours clinics.1 2 During the COVID-19 pandemic, significant reductions in paediatric unscheduled healthcare utilisation were recorded.3 Children as a group were generally less vulnerable to the direct impacts of COVID-19 but were disproportionately affected by indirect consequences.4 5 Important routine healthcare services were impacted; for example, disruptions to childhood vaccinations have increased the risk of future vaccine-preventable disease outbreaks.6 Certain groups, such as children with disabilities and chronic illnesses, faced additional challenges and disruptions to their usual care.7–10 Regarding children’s unscheduled care use, paediatric ED visits dropped significantly across various regions; the average reduction reported in the literature was previously estimated at 64%, with a range of 17–89%.3 There are concerns that delay or avoidance of acute presentations may have resulted in adverse health impacts for children,11 12 with paediatricians in multiple countries reporting their experience of delayed presentations contributing to avoidable harm.13–15 For instance, a survey of 4075 UK and Irish paediatricians in April 2020 estimated that delayed presentation had already contributed to nine deaths.13 These potentially avoidable harms may relate to issues such as delayed cancer diagnoses,16 delayed diagnoses of acute conditions such as appendicitis,17 increased complications for new presentations of chronic diseases such as diabetes18 and reduced access to acute mental health services.19
The factors influencing paediatric healthcare-seeking are complex, involving interactions between individuals and complicated health systems. In studying the reasons for these changes in healthcare utilisation, it is important to understand the decision-making processes of people accessing services. Parents’ perspectives are an essential but sometimes overlooked aspect in understanding this process.1 20 In addition, previous studies have shown that healthcare professionals explain healthcare use in terms of the clinical urgency of the medical issues, whereas patients focus on other practical issues as well, including accessibility, convenience and contextual factors.20 21 Together, these findings illustrate the importance of including service user perspectives in research on accessing paediatric unscheduled healthcare.
Regarding evidence on parents’ decision-making specifically, a systematic review before the pandemic identified several important factors associated with unscheduled care use, such as the perception of the condition’s urgency, a need for reassurance, waiting times and the availability of services.1 In the context of previous pandemics and epidemics, the 2003 severe acute respiratory syndrome (SARS) pandemic and the 2015 Middle East respiratory syndrome (MERS) outbreak were associated with reduced paediatric ED visits.3 Suggested reasons for the reduction during the SARS epidemic included fear of infection, media influence and public health advice that people with symptoms should stay at home.3 22–24 In contrast, the 2009 influenza A (H1N1) pandemic was associated with increased paediatric ED use,3 possibly related to parents’ fears and media coverage at the time.3 25 26
How parents made these kinds of decisions during the COVID-19 pandemic is not currently clear. Some proposed causes for the reductions include fears around COVID-19 infection when attending hospitals or primary care, changes in infectious disease incidence with reduced social contact and perceptions around healthcare availability.14 27–29 Changes in the provision of hospital care may have also contributed; for example, some services required the redeployment of paediatric staff to adult services, restructuring of EDs and cancelling outpatient care.30
We aimed to gain a greater understanding of parent decision-making around accessing paediatric unscheduled healthcare during the COVID-19 pandemic to inform planning for future public health emergencies to ensure safe access to paediatric healthcare services. Our specific objectives were (i) to describe which factors were important to parents in decisions to access paediatric unscheduled healthcare during the pandemic, (ii) to describe which factors were important to parents in decisions to delay or avoid accessing paediatric unscheduled healthcare during the pandemic and (iii) to describe differences in these results across different geographic regions and country economic classifications. Of note, various terms for parents, caregivers and guardians may be applied in this area. For this review, we use the term ‘parent’ to include a range of individuals responsible for care and decision-making for children, including biological parents, legal guardians and other primary caregivers.
Methods
This mixed methods review and thematic synthesis were conducted and reported based on best practice guidance, adapted from the Joanna Briggs Institute (JBI) recommendations for mixed methods systematic reviews, the Enhancing Transparency of Reporting the Synthesis of Qualitative (ENTREQ) statement and the updated PRISMA statement.31–35 The mapping of ENTREQ items to specific sections of the report is provided in online supplemental table S1.
Supplemental material
Search methods
We applied the Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) tool to the research aims and objectives to develop the research question, identify search concepts and define a comprehensive search strategy.36 The SPIDER tool was chosen as it is designed specifically for qualitative and mixed methods research.36 The research question was: ‘What factors were reported by parents to influence their decision-making regarding accessing paediatric unscheduled healthcare during the COVID-19 pandemic?’ Potential search terms were initially identified from a previous systematic review on the topic before the COVID-19 pandemic.1 COVID-19-related terms were identified from the Royal College of Surgeons in Ireland library guide website.37 Further search terms were identified by examining the title, abstracts and subject indexing of three studies, which were known to be relevant to this review.21 38 39 Inclusion and exclusion criteria were developed by applying the SPIDER tool to the research question, aim and objectives. These criteria are outlined in table 1. The search concepts and the strategy for each source are included in online supplemental tables S2 and S3.
Inclusion and exclusion criteria
The searches were carried out in July 2023, and the sources accessed were MEDLINE, Embase, Web of Science, PsycEXTRA, PsycINFO, Global Health, Global Index Medicus, Dissertations and Theses Global, Google Scholar and OAISter. Forward and backward citation searching was also carried out on included articles using citationchaser.40 We screened the title and abstract of all studies returned against the above inclusion and exclusion criteria and then examined the full text of any potentially relevant articles for inclusion. A single reviewer carried out the screening.
Data extraction
Initial categories for data extraction were identified based on a previous review and the JBI guidance1 34 and incorporated into a standardised data collection tool (online supplemental table S4). These categories were chosen primarily to provide background on the study design and context. The results section of all included reports was entered into Nvivo 14.23.0 to facilitate thematic synthesis.
Data synthesis and analysis
This review followed a convergent integrated mixed methods design,34 which has the benefit of producing results that consider the entire range of evidence together and may provide more detailed insights.41 We applied the thematic synthesis approach outlined by Thomas and Harden.33 35 Quantitative results were transformed by coding the data into ‘textual descriptions’, also described as ‘qualitising’.34 41 This approach has been used in several other reviews that applied thematic synthesis to the combined results.42–45
This synthesis process initially involved inductive line-by-line open coding using Nvivo 14.23.0. Relevant text for coding included any text in the ‘Results’ sections of included studies that described parent-reported factors in decision-making around accessing paediatric unscheduled care during the pandemic. This text could include direct quotes from participants, the authors’ interpretations and the authors’ reporting on quantitative results.
The codes emerging from this process were then organised into descriptive themes. This was done by repeatedly reviewing the initial codes and the text of the studies and associating related codes, thinking deductively about the themes occurring in multiple reports.46 Direct quotes are included where relevant to ensure the original context and meaning are represented.
We then developed analytic themes by examining how the descriptive themes explain the research question. This involved abductive and retroductive reasoning in inferring general conclusions about the results across the included studies.46 It is important to note the distinction between the descriptive themes and the analytic themes, in that the descriptive themes aim to ‘stay close to’ the primary studies and use their own terms, whereas the analytic themes seek to ‘go beyond’ the primary studies in an attempt to answer the research question.33 This separation aims to create a synthesis result that includes ‘abstract and formal theories’, which are still ‘empirically faithful’ to the primary studies from which they were developed, as described by Sandelowski and cited by Thomas and Harden.33 47
Regarding different regions and economies (Objective (iii)), we categorised studies according to their WHO regional groupings and The World Bank classification.48 49 We then compared and contrasted the contribution of studies from different regional groupings and income classifications to different themes and subthemes.
Analytical model
We followed a similar approach to that used by Houghton et al to create a model to convey the key analytical findings.50 The purpose of this model is to provide a simple visual representation of the main analytic and descriptive themes, as opposed to a detailed framework of all potential factors identified. First, considering the research question, we examined the relationships between the descriptive and analytic themes in an iterative process. Then, abductive and retroductive reasoning were again used to organise factors into those that encouraged or discouraged attendance. Following this, we created multiple mind maps to design an optimal way of displaying the core results and then adapted these into a final overarching analytical model. These steps were repeated until it was felt that the model accurately provided a simple visual representation of the main descriptive and analytical themes.
Quality appraisal of included studies and sensitivity analysis
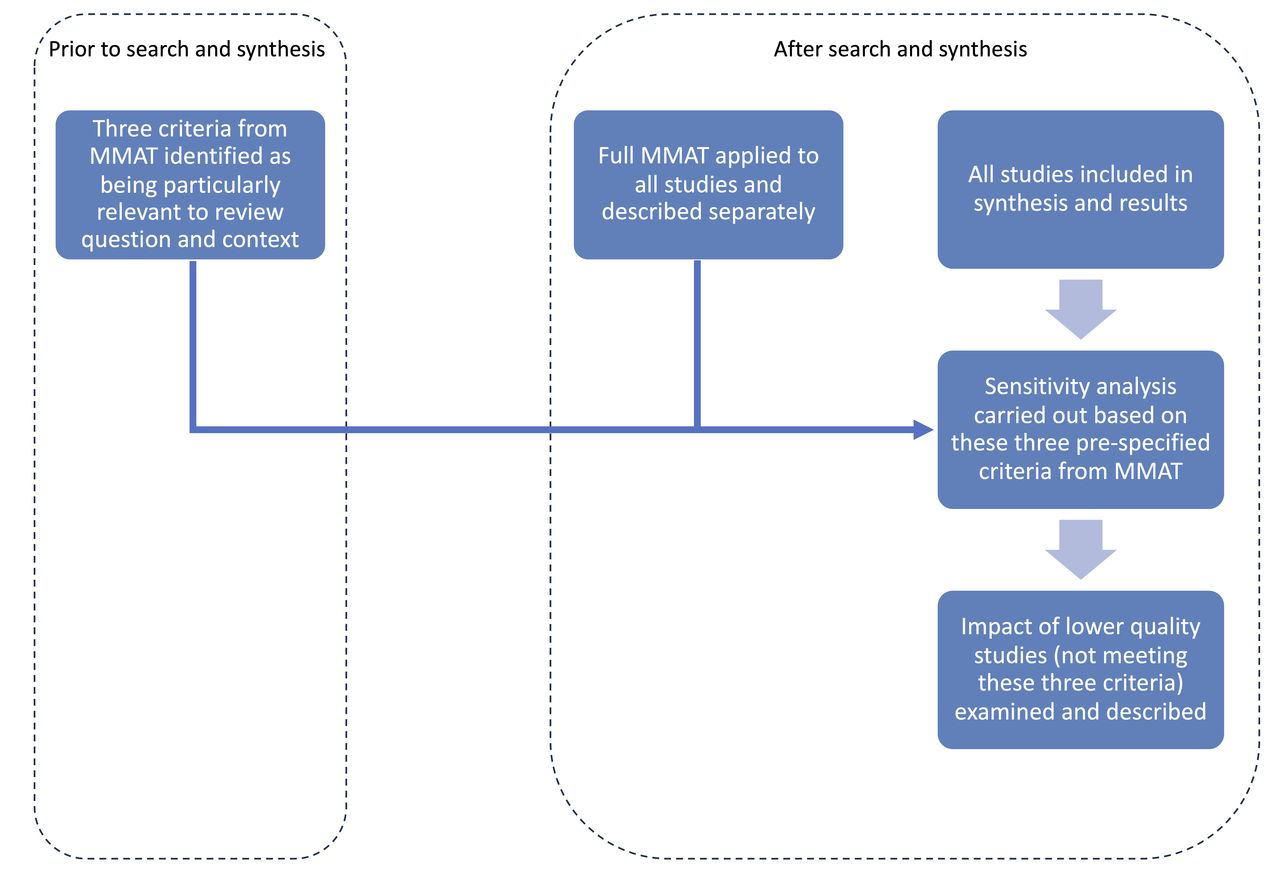
We used the Mixed Methods Appraisal Tool (MMAT) to appraise the quality of individual studies, applied by a single reviewer.51 Regarding incorporating critical appraisal into the results and conclusions, there is a lack of consensus on the best method for qualitative and mixed methods reviews.52 In addition, the MMAT advises against calculating an overall score, instead recommending that the individual scoring is presented. Consequently, we included all studies in the synthesis and results, presented the full MMAT results for each study and also conducted a sensitivity analysis after synthesis to examine the contribution of potentially lower-quality studies to the results. This process is similar to the approach described by Carroll and Booth, which has previously been applied to qualitative syntheses of mixed methods research.53 54 For this sensitivity analysis, we selected three criteria from the MMAT that were identified as being particularly relevant for accurately capturing parent perspectives, and studies that did not meet these three criteria (where applicable) were classified as being potentially of lower quality. These three criteria are outlined in online supplemental table S5, along with the rationale for their selection. We then examined the contribution of the potentially lower-quality studies to the results by assessing what themes and subthemes would have remained without the evidence from these studies. This overall quality appraisal and sensitivity analysis process (figure 1) serves to transparently and explicitly examine the impact of potentially lower-quality studies on the results; at the same time, it does not exclude any studies based on criteria that may be considered controversial and unvalidated. Similar approaches have been previously described elsewhere.53 55 56

Quality appraisal and sensitivity analysis process.
Patient and public involvement
This rapid review was conducted without patient or public involvement.
Results
A total of 14 reports relating to 12 studies were ultimately included in the review (figure 2, table 2 and online supplemental table S6).38 39 57–68 This includes studies with potentially lower quality, as described in further detail in the Methodological quality appraisal and sensitivity analysis section below. The studies were mainly conducted in Europe, and all were in high-income economy countries.48 The studies were performed over various periods and with various pandemic restrictions, with data collection occurring in 2020 for most.

Preferred Reporting Items for Systematic Review and Meta-Analysis flow diagram. Adapted from Page et al.82
Summary of included studies
Descriptive themes
We described four key descriptive themes: (i) concerns about COVID-19 infection, (ii) balancing and navigating risks, (iii) perception of healthcare status and conditions and (iv) perception of information and advice. The contribution of each study to the various themes is demonstrated in table 3.
Contribution of studies to themes
Concerns about COVID-19 infection
Concerns about COVID-19 infection were directly described in eight studies.38 39 57 58 60 62 65 68 This is mainly related to concerns that the child or family would acquire COVID-19 infection while attending healthcare services.
Exposure to COVID-19 in healthcare settings
The risk of COVID-19 exposure was a key finding in a number of quantitative surveys and was the most commonly reported concern for parents in some.57 58 62 68 Similarly, qualitative studies demonstrated related concerns and expanded on parents’ reasoning and understanding. The hospital environment, including the physical setting and behaviour of others (staff and patients), appeared to influence parents’ perceptions of COVID-19 risk. Some parents reported feeling reassured when they noted ‘how well everything was managed’60 and specifically due to COVID-19 measures in place including social distancing.39 60 67 The concept of trust in health professionals and their practices to reduce this risk was apparent; some parents were reassured that they had ‘things in place keeping everyone safe’.39 In contrast, other parents were concerned about being in confined spaces where they witnessed people not following precautions,39 60 such as in waiting rooms where they noted ‘the majority of people not wearing masks and people coughing’.39 In some studies, this concern of acquiring COVID-19 extended further to exposure while travelling to or from the healthcare setting, particularly with public transport.39 57 65 67
Concern about acquiring COVID-19 was noted to change over time in three studies, with a reduction in concern being the main finding.39 57 60 Some parents were reassured that healthcare settings would be better adapted to reduce the risk of infection as the pandemic progressed: ‘I imagine now that the hospital is so slick’.60 Others were reassured by their previous experience attending during the pandemic.39 60
Sources of fears and concerns
Some parents described the media as contributing to their fears,38 39 such as through ‘scaremongering tactics’ associated with social or mainstream media and a ‘hyperawareness of mortality’ due to media reports.39 Another stated outright that the media ‘gives you the impression that the corona is coming from the hospital’.38 In one study, reports from parents about fears were felt to reflect comments by the UK Health Secretary at the time, of ‘don’t kill your gran by catching coronavirus and then passing it on’.38 In addition to the media, some participants in this study described concern and advice not to attend coming from family members,38 and others noted the fact that the virus was new and not fully understood as being a cause for concern in itself.39 60
Balancing and navigating risks
Balancing and navigating risks relates to other themes but was also reported by parents as a process in its own right.39 59 60 63 68 This could include weighing up COVID-19 concerns, the severity of the child’s illness and different responsibilities. Some parents explicitly described this process of weighing up risks, depicting going to the ED as a ‘judgement call’ based on their assessment of how unwell a child was or after seeing a GP.39 This weighing up of risks was sometimes described as a challenging process by parents.60 Some described attending ED when they found it was a difficult decision to make and were uncertain: ‘it was a very sort of, “do I take him, do I not”…(but) I would never forgive myself if I didn’t take him.’60
Risk to children versus risk from children
Some parents also explicitly differentiated the infection risk to children versus from children; the risk to children was mainly felt to be ‘minimal’, whereas passing on COVID-19 to others was a worry.60 Parents reported concern that children would acquire COVID-19 in the hospital and pass it on to ‘vulnerable’ people afterwards39 60 and concern that children would pass on COVID-19 to ‘vulnerable’ people in the hospital while attending.60 62
Severity of the child’s illness
The severity of the child’s illness was another factor in decision-making in several studies.38 39 59 60 65 Parents described seeking care when they judged the illness sufficiently severe38 39 60 and avoiding seeking care when they did not feel it was severe enough.65 Some tried to manage things at home but sought help when the potential severity of the condition meant it was something they were not confident dealing with themselves, such as a head injury.60 Others referred to the ‘parent’s instinct’ or their ‘gut feeling’, which allowed them to decide when help was needed and could outweigh other concerns.39
.so you have that instinct, if you think that your son or daughter …is poorly… You know … then you don’t think of anything else apart from getting them the treatment he needs or she needs.39
There was some divergence of opinion among parents regarding changes in the threshold for seeking care during the pandemic. Some described being more cautious in their decision-making around accessing care during the pandemic and discussed the concept of ‘raising the bar’ for when to attend in terms of the severity of the illness.60 Conversely, others described how they only used services when needed, but that this was the same as before the pandemic60 or how they continued seeking help early when needed.59 There was similar divergence in the surveys, with some supporting an unchanged threshold,68 and others indicating reduced attendance rates for the same level of illness during the pandemic.63
Responsibility
The concept of responsibility was noted in two studies, which both described two contrasting issues: responsibility to their child to get healthcare and a broader social responsibility to follow the rules or guidance.39 60 Some parents discussed the responsibility to act in the child’s best interests, regardless of other factors, and an obligation to protect or negotiate care for one’s children.39 60 Conversely, several parents in both studies reported concern with ‘breaking the rules’ and feeling responsible for ‘following the rules’ and acting in a ‘socially responsible’ way.39 60 These feelings of social responsibility supported decisions to delay or avoid seeking healthcare. Some parents reported a reluctance to seek healthcare due to fear of judgement by others, which may have contributed to this concern about social responsibility and following the rules.39 57 Fear of judgement by professionals was a prominent reason for not attending in one survey.57 In addition, several parents found the rules and changes to be ‘confusing’ and ‘unfair’.39 As a result, they did not know what they should be doing and how best to follow the rules and fulfil their social responsibilities. This ultimately ‘undermined trust and left participants feeling frustrated’.39
when we were in the initial lockdown there was less confusion and I think that most people were aware of what was happening and then suddenly we’re in another lockdown and everything was rushed and nothing was really broadcast very, very well shall we say and… a lot of the time people are unclear as to what they should be doing’39
Perception of healthcare service status and conditions
Perception of the status of and conditions in healthcare services was identified as a theme from most studies.38 39 57 59 60 64 65 68 Parents frequently raised this as a reason for avoiding care, and parents’ understanding of whether healthcare services were open influenced their decision-making.
Perception of burden or capacity issues
Several studies described the concept of not wanting to attend healthcare to avoid adding to a healthcare system already experiencing a significant ‘burden’.39 57 60 68 Parents discussed in interviews how they ‘didn’t want to put any extra pressure on the doctors’60 or ‘don’t want to put additional pressure’ on the National Health Service (NHS).39 Others were advised by friends or family not to attend ED due to the conditions there, sometimes described as ‘horrible’.38
Some parents were worried that others believed they ‘don’t deserve an appointment’, leaving them in a situation of ‘potentially dying or becoming seriously ill with something that could be treated or prevented entirely’.39 In parallel, others described how limited services were likely needed by other patients:
that the doctors was probably, massively overly used at that point because of all this Covid so we were like we’re not going to get an appointment or, even if we do, there’s probably somebody who needs it more than us.60
Survey findings supported both of these concepts: concerns that the service would be busy or that others were in greater need were frequently reported by participants in two studies.57 67
Perception of whether healthcare was open or accessible
Interpreting government or public health advice as meaning to stay away from all healthcare was described in three studies.57 60 66 Several parents in an English study described their interpretation of the ‘Stay home, Protect the NHS, Save lives’ message as meaning people should not use health services: “protect the NHS” had that impact, if there’s any worries apart from Covid then stay away, quite a blunt message’.60 Despite this, most parents in the same study reported that they understood health services were available throughout the pandemic: ‘I think there’s been enough encouragement that if you’ve got an unwell child they should be seen. I certainly haven’t seen anything to say otherwise’.60 In addition to this divergence in understanding of the meaning of public health advice, other parents were concerned by a lack of clarity about how hospitals were operating during the pandemic.60 Survey results included similar beliefs about advice meaning to stay away,57 66 with a significant proportion of respondents interpreting government advice as meaning to ‘avoid health services’.57 Some parents in a US-based survey endorsed a more specific interpretation of the advice, with 43% of those who did not seek medical care when their children were sick noting that the government advice was not to go to the doctor for a minor problem.65
Some studies described a shift towards increased virtual attendances,59 65 67 which may be related to the perceived status of face-to-face services and the interpretation of public health advice.67 Experiences of virtual or remote services were mixed. Many parents reported satisfaction and positive experiences with virtual emergency clinics,64 virtual GP appointments67 and text information from GPs.39 Conversely, others reported negative experiences with telephone consultations and were concerned that they were insufficient to diagnose and treat their child’s illness, resulting in ED attendance: ‘I needed someone to look at him properly, to listen to his chest. You can’t do that over the telephone’.59 Some parents were concerned that language barriers would mean they would not be adequately understood over the phone and felt that an in-person review was essential.38
Perception of information and advice
The impact of information and advice on decision-making was apparent across seven studies.38 39 59–61 65 68 Parents commonly sought advice before attending unscheduled care, and their perceptions of the quality of information sources factored into the process.
When questioned on whether participants sought advice before attending the ED, most reported that they had, with complementarity between qualitative and quantitative studies; commonly used sources of advice were GPs and NHS 111.39 59–61 Parents described seeking advice for ‘validation’ or ‘reassurance’ that they were doing the right thing in seeking care.39 66 In addition to healthcare professionals and official sources, some sought advice from friends or family.38 39
Parents described a range of positive perceptions towards certain kinds of information and information sources.38 39 61 66 Some sources were identified as reliable by parents, including NHS 111,38 pharmacies, educators and medical professionals.39 This ‘trustworthiness’ of information sources directly influenced perceptions around COVID-19 and the pandemic.39 One study specifically examined the impact of an information leaflet for identifying when your child is seriously unwell and found that it increased confidence in recognising severe illness and sometimes caused parents to seek healthcare where they would not have otherwise.61 Similar to seeking advice for validation or reassurance, some parents described finding information useful because it was reassuring: ‘The information was useful since it reassured me, useful tips and information on when to seek medical help (again) were given’.66
On the other hand, negative perceptions around information or advice were also reported across several studies.38 39 60 66 67 These negative perceptions related to misinformation online,38 60 unclear or confusing information,67 delays and confusion with NHS 111,39 59 67 information not being child-specific66 and a lack of available information.67 Parents in these studies reported that this contributed to their confusion, upset and uncertainty; in some cases, this led to a decision that they would not consult information sources before attending ED in the future.
Analytic themes and analytical model
The studies had various perspectives and focus, and the findings underscore the complexity of this decision-making process. The following two overarching analytic themes are intended to summarise the main commonalities across the range of findings when considering the specific research question of this review. The proposed analytical model summarising the key factors identified and their impact is presented in figure 3.

{kind=link}
{kind=link}
{kind=link}
Analytical model.
Parents balance a range of different risks and competing responsibilities
Parents’ decision-making depends on their perception of various risks, including COVID-19 acquisition by the child or family, passing on COVID-19 to others, negatively impacting healthcare services or other users by attending and potential harm to the child from not attending. Parents balance and navigate these risks, and this process may be moderated by their perception of different responsibilities related to the parent role: the responsibility to look after their children and a broader social responsibility to follow the rules and behave conscientiously. This process of weighing up different priorities and concerns can be challenging; sometimes, the decision is made based on parents’ instincts or gut feelings.
Parents are amenable to external information and advice influencing their decisions
The impact of external factors was clear from the studies, particularly concerning parents seeking information and advice from trusted sources, with most seeking advice before attending ED. Parents often found this advice reassuring or validating in that it confirmed that they were doing the right thing by deciding to attend when uncertain. On the other hand, many reported issues with some information sources, such as those found online, and with increased fear or uncertainty being driven by the media. Potential misconceptions around official public health advice were common in some studies. Patients’ perspectives on risks, roles and responsibilities may also be influenced by external agents and sources of information, including the media, healthcare professionals and the community.
Methodological quality appraisal and sensitivity analysis
The full methodological quality appraisal results for each study are shown in online supplemental table S7. Considering the pre-selected MMAT criteria for sensitivity analysis, one of the qualitative studies did not meet criterion 1.2.,64 one of the quantitative studies did not meet criterion 4.3.63 and the quantitative part of the mixed methods study did not meet criterion 4.3.39 Results from the quantitative part of the mixed methods study and all parts of the other two studies did not significantly contribute to the descriptive themes and subthemes, as shown in table 3 and the results presented above.
Discussion
Key findings
The included studies describe how parents balanced a range of risks, concerns, worries and responsibilities in their decision-making. They also show how external information or advice influenced the decision-making process and outcomes. Parents were concerned about the family acquiring or passing on COVID-19 while attending healthcare, but infection control measures and other experiences reassured some. Some described the contrast between responsibility to their children, related to the severity of illness and a broader social responsibility to follow COVID-19 rules and guidelines. Concern about adding to an already burdened healthcare service was a common theme. It was noteworthy how minimal reference there was to background child and family factors, such as sociodemographic aspects, influencing this process. In addition, most of the studies were carried out in Europe, and all were carried out in high-income settings, limiting comparisons across different geographical regions or economic contexts.
Comparison to other literature
Parents’ perception of the severity of the child’s presenting condition and their need for reassurance is evident from studies before the COVID-19 pandemic,1 and complementarity is seen with some of the results of this review. The concept of understanding and balancing different risks to make the decision has also been described in previous studies1 60 69 ; before the pandemic, these risks are related to the child’s health risks from their current illness, whereas this review adds additional risks to children, families and broader society from COVID-19 transmission within healthcare settings. These additional risks weigh into the mix of factors parents must consider and balance when deciding whether to attend unscheduled care with their children.
Interpreting and understanding information influenced decision-making in some studies before the pandemic but was not a prominent theme in a recent systematic review.1 In our review, however, this was a key theme; parents frequently reported that information and the quality and reliability of information sources directly influenced decision-making. For example, it is concerning that there was a wide variation in parents’ understanding of public health guidance, with many parents understanding official guidance to mean they should stay away from hospitals entirely. This contrast with the systematic review before the pandemic may point to the increasingly important role of trusted information sources today, especially with rapid changes in circumstances, rules and guidance, such as during the COVID-19 pandemic. Parents in included studies raised concerns about the vast amount of information available and about misinformation online, a concept described by others as an ‘infodemic’ and a significant public health issue to address.57 70 The critical importance of transparency and trust in risk communication and public health messaging was also apparent during the 2003 SARS.71 Although not reported in this review, health literacy has previously been shown to impact parental health-seeking behaviour and ED use for children,1 72 and it is an essential consideration in public health communications.
In this review, parents frequently highlighted hesitancy in attending due to concern about adding to already burdened healthcare services or due to others being in greater need of limited resources. In contrast, parents did not explicitly report this in the systematic review immediately before the pandemic.1 This may be related to public health and media reports on the disease burden and strains on healthcare services, which added to some parents’ worries.
Finally, in studies conducted before the pandemic, background child and family factors such as race, ethnicity and socioeconomic status were found to be important in influencing parents’ healthcare-seeking behaviour in accessing unscheduled care1 73–76 ; however, this is not evident in the current study. This is likely because the included studies focused on the impact of COVID-19 and, for the most part, did not directly aim to study differences due to background characteristics.
Strengths and limitations
Review methods
This review took a transparent approach to describing and justifying methodological decisions. We used a convergent integrated approach to combining the different types of research, which is appropriate to this specific research question, as outlined in the JBI guidance.34
Thematic synthesis is appropriate to the review question and inductive approach taken and is a thorough method that develops findings that are clearly connected to the results of the included primary studies.33 Separating descriptive themes from analytic themes differentiates between the primary studies’ data and our more analytical engagement with the evidence to apply it to the research question and develop original conceptualisations of the phenomenon, increasing transparency in the results.
Due to time and resource constraints, we could not consult with experts in the area or pilot the search strategy to ensure its completeness, and screening was carried out by a single reviewer. While using the SPIDER tool is a strength of this study, in that it is appropriate for the type of research synthesis and research question, we note that it has been found to have a lower sensitivity in searches in some circumstances.77 Again due to time and resource constraints, we did not conduct independent validation of the inclusion and exclusion criteria with multiple reviewers, which would have added to the reliability of the findings. In addition, only English language studies and the selected data sources were included, and significant studies in other languages or sources may be missed. Further to this, there is a potential for publication bias to have impacted on the findings of this review, and this was not formally assessed.
We have described the contribution of different studies to themes and outlined the strengths and weaknesses of the included studies and the review methods. However, we did not conduct a formal, comprehensive assessment of confidence in the review findings. It has been noted that there is a need for the development of a GRADE approach to assessing confidence in the findings of mixed methods reviews.78 Quality assessment was carried out by a single reviewer.
Finally, in this study, we conceptualised unscheduled healthcare as one system, as this is thought to reflect how patients view and navigate services more accurately.1 2 57 79 However, most of the included studies were based on a specific type of service, commonly the ED. Thus, the results may be biased towards ED access decisions instead of unscheduled care in general. We also did not assess how different healthcare systems may have impacted parents’ perspectives of what was the most appropriate course of action, outside of that which was explicitly described in the results sections of included studies.
Included studies
The included studies were biased towards high-income, European settings; this limits generalisability to other settings. In addition, two studies carried out in similar settings in England contributed heavily to the descriptive themes.39 60 Participants were mainly recruited in healthcare settings, which may bias the results by excluding people who could not access mainstream healthcare during the pandemic. Most of the included surveys were carried out online or circulated through social media, which again may risk excluding certain vulnerable groups.80 Only three studies did not meet the pre-specified quality criteria; when the contribution of the parts of these studies in question was examined in sensitivity analysis, they did not significantly contribute to the review findings.
As discussed above, background child and family factors were previously found to influence parent decision-making. However, they were not consistently reported in this review, likely due to the focus of the included studies.
Implications and future research
In terms of public health communications, this review has demonstrated that different parents may understand the same public health advice differently. Of particular concern was the potential misconception of the ‘stay-home’ type of advice as meaning not to access healthcare services at all. This finding highlights the importance of research that directly explores parent perceptions, including factors that contribute to the differences in understanding, to inform public health policy.
Furthermore, understanding what parents find reassuring and their perception of risks is important in developing messaging that illustrates how healthcare is safe during times of uncertainty, such as the COVID-19 pandemic. In addition, ensuring that healthcare systems can meet the needs of the populations they serve and that the public understands this capacity exists is necessary to prevent potentially harmful delays or avoidance.
Specific measures that may improve public health communication in this area include involving parents in developing messaging and ensuring a transparent and unified communication approach.81 Of note, parents identified social responsibility and responsibility to their child as potentially competing aspects in decision-making; this could be an area to further explore in terms of achieving a balance with parents understanding to attend when they are concerned about their child while also taking into account the current public health guidance.
Conclusion
This mixed methods review and thematic synthesis describes the factors influencing parent’s decision-making when considering accessing paediatric unscheduled healthcare during the COVID-19 pandemic. Parents balance a range of risks, concerns, advice and responsibilities; this can be a complex process with multiple competing priorities. External sources of advice and information are important, and parents are amenable to these influencing their decisions if they are perceived as trustworthy and are correctly understood. Potential misconceptions around public health advice may reflect the multitude of information sources and the rapidly changing circumstances of the pandemic. Public health policy and planning should consider parent perspectives in developing measures to ensure equitable access to safe and appropriate paediatric healthcare services.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
In particular, we would like to thank Mr Richard Little, who provided supervision, feedback and input into the project's conceptualisation, design and methods development phase. We would also like to thank the London School of Hygiene and Tropical Medicine MSc in Public Health Project Module Organisers, Dr Anna Foss and Dr Sarah Smith, for their support throughout the project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CD-C conceived the study idea; CD-C designed the search strategy, synthesis method and quality appraisal plan; CD-C and DS reviewed and revised the search strategy, synthesis method and quality appraisal plan; CD-C screened studies for eligibility, extracted data and initially synthesised the data; CD-C and DS reviewed and revised the synthesis results; CD-C wrote the first draft of the manuscript; CD-C and DS critically reviewed and revised the manuscript. CD-C and DS both reviewed the results and approved this final version of the manuscript. Responsible for the overall content as the guarantor: CD-C.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.