Article Text

Abstract
Objective The objective was to analyse the associations of intensive care unit (ICU) and high care unit (HCU) organisational structure on in-hospital mortality among patients with sepsis in Japan’s acute care hospitals.
Design Multicentre cross-sectional study.
Settings Patients with sepsis aged ≥18 years who received critical care in acute care hospitals throughout Japan between April 2018 and March 2019 were identified using the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB).
Interventions None.
Participants 10 968 patients with sepsis were identified. ICUs were categorised into three groups: type 1 ICUs (fulfilling stringent staffing criteria such as experienced intensivists and high nurse-to-patient ratios), type 2 ICUs (less stringent criteria) and HCUs (least stringent criteria).
Primary outcome measure The study’s primary outcome measure was in-hospital mortality. Cox proportional hazards regression analysis was performed to examine the impact of ICU/HCU groups on in-hospital mortality.
Results We analysed 2411 patients (178 hospitals) in the type 1 ICU group, 3653 patients (422 hospitals) in the type 2 ICU group and 4904 patients (521 hospitals) in the HCU group. When compared with the type 1 ICU group, the adjusted HRs for in-hospital mortality were 1.12 (95% CI 1.04 to 1.21) for the type 2 ICU group and 1.17 (95% CI 1.08 to 1.26) for the HCU group.
Conclusion ICUs that fulfil more stringent staffing criteria were associated with lower in-hospital mortality among patients with sepsis than HCUs. Differences in organisational structure may have an association with outcomes in patients with sepsis, and this was observed by the NDB.
- quality improvement
- adult intensive & critical care
- mortality
- retrospective studies
- cross-sectional studies
Data availability statement
Data are available on reasonable request. The data are provided from the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB), included in the article or uploaded as online supplemental information and strictly regulated. The dataset used in this study is available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- quality improvement
- adult intensive & critical care
- mortality
- retrospective studies
- cross-sectional studies
STRENGTHS AND LIMITATIONS OF THIS STUDY
The cross-sectional study design enables an investigation into whether the organisational structure of intensive care units and high care units is associated with in-hospital mortality in patients with sepsis.
The data were collected through the use of standardised and validated procedures and instruments, which increases the internal validity of the data.
Data were obtained from the National Database of Health Insurance Claims and Specific Health Checkups of Japan.
One limitation of our study is the lack of information on each patient’s physical and laboratory examination results and Sequential Organ Failure Assessment scores.
The large number of cases excluded from the analysis should be treated with caution when interpreting the results.
Introduction
Sepsis is a dysregulated host response to infection resulting in potentially fatal organ dysfunction1 and is associated with heavy clinical and economic burdens.2 3 Due to the high risk of rapid deterioration, this syndrome requires prompt and intensive treatments such as antibiotic therapy, fluid resuscitation and supplemental oxygen.4 Optimal sepsis treatment is, therefore, dependent on the availability of an effective and rapid healthcare provision system with adequate resources.
Donabedian’s structure-process-outcome model is a well-established framework for assessing healthcare quality5 and has been widely applied in the fields of critical care and emergency care.6–10 The organisational characteristics of intensive care units (ICUs) can be analysed as part of the ‘structure’ component of Donabedian’s triad. Among Japan’s acute care hospitals, critical care is provided in ICUs and high care units (HCUs). While HCUs share some similarities in organisation and function with the high-dependency units of other countries, which are designed for critically ill patients who are less severe than those in ICUs, many Japanese hospitals that lack ICUs treat critically ill patients in HCUs. The definitions of ICUs and HCUs are set by Japan’s medical fee reimbursement system and are based on the units’ organisational structure, such as the availability and experience of medical staff, nurse-to-patient ratio and the evaluation criteria for medical and nursing care needs (table 1). Under this system, ICUs are divided into two types, with type 1 ICUs fulfilling more stringent staffing criteria and receiving higher reimbursements than type 2 ICUs. Moreover, both ICU types are entitled to receive higher reimbursements than HCUs, which fulfil even less stringent criteria. Despite these differences in organisational structure, studies have yet to explore the differences in the quality of care provided to patients with sepsis among these units.
ICU and HCU classifications under Japan’s medical fee reimbursement system
Insurance claims data comprise transactional records for episodes of care and are widely used in healthcare research. In 2009, Japan launched the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB) to collect and maintain claims data and medical data from throughout the country for the purpose of research. These data are formatted according to Japan’s Diagnosis Procedure Combination (DPC) casemix system, which dictates reimbursements for acute care hospitals. As of 2017, the NDB has covered over 95% of hospitals participating in Japan’s reimbursement system.11 However, the NDB has yet to be applied in critical care research. Using data from the NDB, this study aimed to analyse the impact of the organisational structure of ICUs and HCUs on in-hospital mortality among patients with sepsis in Japan’s acute care hospitals.
Methods
Study design and data source
We conducted a multicentre cross-sectional study of adult patients with sepsis who were admitted to an ICU or HCU in acute care hospitals throughout Japan between 1 April 2018 and 31 March 2019. The patients were divided into three groups according to the unit in which they received critical care: type 1 ICUs as ICUs staffed by physicians with long intensive care experience (≥5 years) and high nursing density (minimum nurse-to-patient ratio of 1:2), type 2 ICUs as ICUs staffed by physicians regardless of their intensive care experience and high nursing density (minimum nurse-to-patient ratio of 1:2) and HCUs as HCUs staffed by physicians regardless of their intensive care experience and low nursing density (minimum nurse-to-patient ratio of 1:5). In addition to staffing criteria, these units are also categorised based on the monthly proportion of admitted patients who fulfil specific evaluation criteria for medical and nursing care needs (online supplemental appendix table 1). ICU and HCU lengths of stay were calculated for each case, and if an ICU stay was identified, the case was included in the ICU group. It was assumed that the initial treatment of sepsis would be initiated in the highest level of wards in each hospital. Priority was given to type 1 ICUs, followed by type 2 ICUs.
Supplemental material
The data source was a DPC database extracted from the NDB. DPC data comprise clinical information and claims data and include patient demographics (eg, age, sex, height and weight), primary and secondary diagnoses, dates of admission and discharge, comorbidities, treatments (eg, mechanical ventilation, renal replacement therapy and vasopressor administration) and discharge status. Information on ICU and HCU utilisation is also included.
Patient selection
Patients with sepsis were identified as those with the relevant International Classification of Diseases, 10th Revision codes on admission (online supplemental appendix table 2). The dates of ICU/HCU admission were determined based on Japanese treatment codes provided in the claims data. We excluded patients who were admitted before the study period or who were not yet discharged from hospital during the study period, patients aged below 18 years and patients with missing age data.
Supplemental material
Patient characteristics and treatments
We collected information on the following patient baseline characteristics: age, sex, hospital admission course (emergency or non-emergency) and major diagnostic category. Age variables were stratified into four groups: 18–59 years, 60–69 years, 70–79 years and 80+ years. Using Japanese procedural codes, we also identified the use of the following treatments: mechanical ventilation, noninvasive positive pressure ventilation, high-flow oxygen therapy, renal replacement therapy, endotoxin adsorption, tracheotomy, vasopressors (epinephrine, norepinephrine and vasopressin). Patients with acute respiratory distress syndrome were identified using the International Classification of Diseases, 10th Revision code J80.
Outcome measures
The study’s primary outcome measure was in-hospital mortality, and the secondary outcome measures were ICU/HCU stay (days) and overall hospital stay (days).
Statistical analysis
Continuous variables were calculated as means and SD, and categorical variables were calculated as frequencies and percentages. One-way analysis of variance and the χ2 test were used to compare the continuous and categorical variables, respectively, among the three ICU/HCU groups (type 1 ICUs, type 2 ICUs and HCUs). We plotted Kaplan-Meier survival curves to examine the differences in survival among the three groups.
Bivariate analyses were performed to identify patient characteristics and treatments that were significantly associated (p<0.05) with in-hospital mortality. Our previous study used DPC data to develop a model for predicting in-hospital mortality in ICUs and showed that even a model with a small number of variables excluding the primary diagnosis was sufficient to predict in-hospital mortality.12 Referring to our previous study,12 age, vasopressors, mechanical ventilation, renal replacement therapy and hospital admission (non-emergency or emergency) as patient factors were included as covariates in a Cox proportional hazards regression model with in-hospital mortality as the dependent variable and the ICU/HCU groups as the main independent variable of interest. The HRs and 95% CIs were calculated for the independent variables. The ICU/HCU groups were treated as a stratum of the hospital factor. In addition, subgroup analyses were performed for patients with sepsis with blood, blood-forming organs and immunological disorders.
P values lower than 0.05 were considered to be statistically significant. All analyses were performed by using SPSS V.26.0 (IBM).
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Figure 1 shows the flow chart of patient selection. From among 671 425 patients admitted to an ICU or HCU in 900 hospitals, we identified 32 690 patients with a recorded diagnosis of sepsis. Patients excluded were 3391 patients whose date of admission and date of discharge did not both fall within the study period; 16 565 patients who did not enter type 1, type 2 or HCU; 161 patients under 18 years of age and 1605 patients with missing age data. After applying the exclusion criteria, we obtained a final study population of 10 968 patients. Of these, 2411 patients (178 hospitals) were treated in a type 1 ICU, 3653 patients (422 hospitals) were treated in a type 2 ICU and 4904 patients (521 hospitals) were treated in an HCU.

Flow chart of patient selection. HCU, high care unit; ICU, intensive care unit.
The patient characteristics and treatments are summarised in table 2. The mean ages of the patients in the type 1 ICU group, type 2 ICU group and HCU group were 72.1 years, 73.6 years and 76.8 years, respectively (p<0.001). There were also significant intergroup differences in sex and emergency admissions. In all groups, men accounted for the majority of patients (57%–61%), and emergency admissions comprised more than 80% of cases. Among the treatments, the use of mechanical ventilation was significantly higher (p<0.001) in the type 1 ICU group (58.4%) and type 2 ICU group (55.0%) than in the HCU group (28.2%). Similarly, the use of renal replacement therapy was significantly higher (p<0.001) in the type 1 ICU group (36.3%) and type 2 ICU group (31.7%) than in the HCU group (14.4%). Vasopressors (norepinephrine, epinephrine or vasopressin) were administered to the majority of patients in the type 1 ICU group (78.0%) and the type 2 ICU group (72.2%), but to less than half of all patients in the HCU group (48.7%) (p<0.001).
Patient characteristics, treatments and outcomes (n=10 968)
Table 2 also presents the outcomes of each group. There was a statistically significant difference in unadjusted in-hospital mortality (46.3% in the type 1 ICU group, 48.5% in the type 2 ICU group and 37.7% in the HCU group). There was no statistically significant difference (p=0.05) in ICU/HCU stay among the groups. Similarly, there was no statistically significant difference (p=0.12) in overall hospital stay among the groups.
The major diagnostic categories of the patients are presented in online supplemental appendix table 3. In all groups, the most prevalent category was ‘digestive system, hepatobiliary system and pancreas’. This was followed by ‘circulatory system’, ‘respiratory system’ and ‘blood, blood-forming organs and immunological disorders’.
Supplemental material
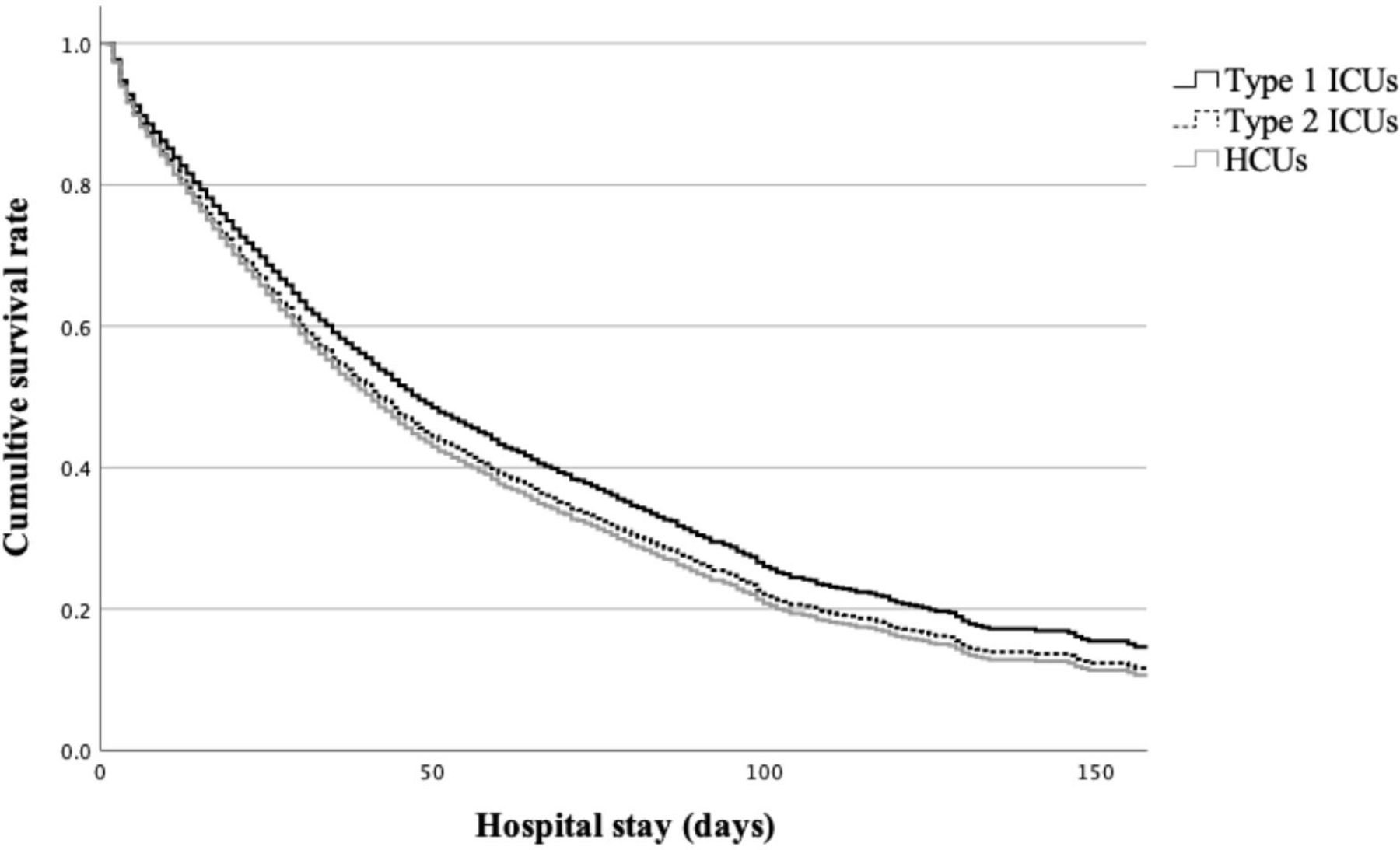
Before statistical adjustment, the HCU group had the highest survival rate. However, the HCU group had the highest hazard of death after adjusting for the covariates using the Cox proportional hazards model (figure 2). The results of the Cox proportional hazards analysis of in-hospital mortality are summarised in table 3. The ICU/HCU groups were significantly associated with in-hospital mortality after adjusting for the covariates (p<0.001). When compared with the type 1 ICU group, the HRs for in-hospital mortality were 1.12 (95% CI 1.04 to 1.21) for the type 2 ICU group and 1.17 (95% CI 1.08 to 1.26) for the HCU group.

{kind=link}
{kind=link}
Adjusted survival curves of the ICU and HCU groups using the Cox proportional hazards model. Type 1 ICU group (black line), type 2 ICU group (black dotted line) and HCU group (grey line). After adjusting for the covariates, the type 1 ICU group had the highest survival rate, followed by the type 2 ICU group. HCU, high care unit; ICU, intensive care unit.
Results of the Cox proportional hazards analysis for in-hospital mortality (n=10 968)
The subgroup analysis results are provided in online supplemental appendix table 4. ICU/HCU groups remained a significant determinant of in-hospital mortality for cases of sepsis with blood, blood-forming organs and immunological disorders. The HRs for in-hospital mortality were 1.19 (95% CI 0.89 to 1.58) for the type 2 ICU group and 1.58 (95% CI 1.19 to 2.10) for the HCU group, compared with the type 1 ICU group.
Supplemental material
Discussion
In this large-scale analysis of national-level claims data, we comparatively examined in-hospital mortality in patients with sepsis among ICUs and HCUs in Japan. The type 2 ICUs and the HCUs were associated with significantly increased hazards of in-hospital mortality when compared with the type 1 ICUs, with HCUs (fulfilling more lenient criteria) demonstrating a higher hazard than type 2 ICUs. Previous studies have reported that health insurance systems are associated with patient outcomes.13 14 These studies demonstrate the relevance of telehealth within the health system for sepsis or critical care cases. Our study also suggests that the Japanese health insurance system’s staffing criteria for these units may affect patient prognosis.
There have been some reports on sepsis using ICD-10 in Japan. The in-hospital mortality is definitely higher than in other previous studies (18%–35%).15 16 The ICD-10 codes used to identify sepsis in the previous study15 included only codes for infectious diseases without the word ‘sepsis’, such as codes for ‘appendicitis-peritonitis’, ‘infectious diarrhoea’, ‘chronic viral hepatitis’ and ‘haemorrhoidal fistula’. In our study, we only included codes that contained the word ‘sepsis’. Another study16 used a combination of codes for severe infection and organ dysfunction as sepsis. The database also included a large number of patients with sepsis who were not admitted to an ICU that met the criteria of the facility. We understand that obvious sepsis cases are coded as ‘sepsis’ containing words because the coding physician diagnoses them as sepsis. In this study, we believe that these sepsis cases entering the ICU/HUC are more likely to be captured as eligible and do not have a lower mortality rate. On the other hand, studies using other approaches still have the potential to include cases of infections that are not sepsis and are likely to capture a broader range of subjects and have lower mortality rates than our study. Therefore, we consider it acceptable that the case frequency is lower and the mortality rate is relatively higher than in previous studies.
In 2015, the American College of Critical Care Medicine Task Force on Models of Critical Care recognised that improvements in ICU structure can lead to better patient outcomes and noted that a dedicated intensivist-led multidisciplinary team is integral to the effective delivery of critical care.17 ICUs can be categorised as ‘open’ or ‘closed’, with the key difference being that only ICU intensivists can direct care and write medical orders in a closed ICU.18 19 A US study reported that closed ICUs were associated with lower mortality in patients with acute lung injury.20 Similarly, a Japanese study of patients with sepsis found that closed ICUs were associated with increased survival and shorter ICU stays when compared with open ICUs.21 A meta-analysis of open and closed ICUs also found that the former had significantly higher mortality rates than the latter for a variety of health conditions.22 In our study, ICU/HCU organisational structure was mainly determined based on staffing criteria. However, while the criteria were met, we could not ascertain the actual staffing numbers or the authority of intensivists in each unit and were therefore unable to determine if each unit operated in an open or closed format. Nevertheless, the medical fee reimbursement system provides objective criteria that enable us to categorise the ICUs and HCUs according to organisational factors. These criteria include the availability and experience of medical staff, nurse-to-patient ratio and the evaluation criteria for medical and nursing care needs. Although previous studies reported that nurse staffing levels had no effect on in-hospital mortality,23 several studies subsequently reported that in-hospital mortality increased with each additional patient per nurse.24–26 In our study, the nurse-to-patient staffing ratio was included in the group criteria, but we could not identify the qualifications of the nurses except in type 1 ICUs. Previous study has shown that structural measures including registered nurse care were associated with improved outcomes for patients with sepsis.27 Japan also has a system of more trained nurses, but it does not operate under the same standards as other countries, so it is difficult to compare the situation with other countries. The SEP-1 Sepsis bundle, which targets processes including antibiotic administration, lactate measurement and fluid administration within 3 hours of sepsis onset; repeated lactate and vasopressor administration for hypotension within 6 hours of sepsis onset, has been shown to improve practice process but not mortality.28 Adherence to the SEP-1 Sepsis bundle was not better for hospital-onset sepsis than for community-onset sepsis.29 However, nurse-to-patient staffing ratios have been shown to have a greater impact than bundle adherence,26 and nurse-to-patient staffing ratios, which have been evaluated in previous studies, may be an important factor in assessing patient outcomes.24–26 Our analysis showed significant differences in in-hospital mortality among the unit types. These findings are consistent with those of previous studies on the organisational structure of critical care.30 31
Our previous study showed that the prognosis of ICU patients was relatively well predicted by age, admission course, mechanical ventilation, dialysis and vasopressors.12 Therefore, our study used these indicators to perform a multivariable analysis to adjust for severity of illness. Among our subjects, mortality was particularly high in patients with sepsis with blood, blood-forming organs and immunological disorders. This corroborates the results of a previous study where haematological malignancies were reported to be associated with an increased hazard for sepsis and 1 year mortality.32 Another study reported an association between haematological malignancies and higher 28-day mortality in patients with sepsis requiring ICU admission.33 Haematological malignancies had a strong prognostic impact in our previous study.12 Therefore, we performed a subgroup analysis of patients with blood and immunological disorders. Our present study found that treatment in type 1 ICUs was associated with reduced in-hospital mortality for such patients, suggesting that higher staffing levels with more experienced specialists can affect outcomes even in severe cases with blood and immunological disorders.
Previous studies have shown that ICU structural factors are also associated with other processes and outcomes of care. For example, staffing characteristics (including the presence of expert intensivists and dedicated pharmacists) have been linked with shorter mechanical ventilation durations.34 Furthermore, regular examinations by intensivists in ICUs were found to be associated with the achievement of lighter sedation goals.35 Another study determined that nurse-driven weaning from mechanical ventilation significantly reduced ventilation durations and ICU stay without adverse effects.36 In contrast to those previous studies, our analysis found no significant differences in mechanical ventilation duration among the ICU/HCU groups. This may be because our observational study was based on staffing criteria and did not account for the actual treatment strategies employed for each case. The presence and distribution of staff alone may not directly affect mechanical ventilation strategies in Japan’s ICUs and HCUs, but further research is needed to explore this relationship.
This study has several limitations. First, there was a lack of information on each patient’s physical and laboratory examination results. Due to the absence of physiological data in the DPC database, we could not assess indicators such as leucocyte count, C reactive protein levels, oxygenation levels and blood pressure. Second, we could not compare Sequential Organ Failure Assessment (SOFA) scores among the groups because these were only introduced into the DPC system in 2018. At present, only type 1 ICUs are required to record these scores, resulting in a lack of consistent data from type 2 ICUs and HCUs. In addition, we did not have access to patients’ comorbidities and were unable to account for their variations. And we could not distinguish between community-onset and hospital-onset sepsis, even though we should manage patients with hospital-onset and community-onset sepsis differently.29 Nevertheless, we were able to include major diagnostic categories in our analytical models. Third, our analysis was dependent on the accuracy of the DPC records, which may include cases of upcoding or miscoding. However, these claims are submitted to insurers for reimbursements and are, therefore, subject to stringent assessments for accuracy. Fourth, there is the problem of selection bias. In Japan, sepsis cases are concentrated in the ICU/HCU. Quick SOFA score is widely used. As a result, requests to the ICU/HCU have become common. In most cases, physicians are not involved in the choice of hospital for admission. This could reduce selection bias. Japanese hospitals rarely have all type 1 ICUs, type 2 ICUs and HCUs. The initial treatment of sepsis is assumed to begin in the highest level wards of each hospital. There might still be room for selection bias, but sorting by physicians and medical staff is unlikely. Finally, our ICU/HCU groups were categorised based on the availability and experience of medical staff, nurse-to-patient ratio and the evaluation criteria for medical and nursing care needs, but we did not have any information on hospital size, staffing numbers or ICU/HCU bed numbers. As a result, we could not determine the physician-to-patient ratio in each unit. It has been reported that an intensivist-to-patient ratio below 1:14 can detrimentally affect medical education, staff well-being and patient care in ICUs.37
This nationwide study is, to the best of our knowledge, the first to observe that the organisational structure of ICUs and HCUs is associated with in-hospital mortality in patients with sepsis in Japan. Staffing criteria, even if they are defined by the medical fee reimbursement system, may affect patient prognoses. Analysing and optimising the organisational structure of critical care units could contribute to the improvement of patient outcomes.
Data availability statement
Data are available on reasonable request. The data are provided from the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB), included in the article or uploaded as online supplemental information and strictly regulated. The dataset used in this study is available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The institutional review board of Kansai Medical University Hospital approved this study (Approval number: 2019078). The requirement for informed consent from patients was waived given the cross-sectional study and the use of anonymised patient and hospital data.
Acknowledgments
We are grateful to the National Database of Health Insurance Claims and Specific Health Checkups of Japan for providing the data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TU, KN and TK conceptualised the study. TU and KN collected the data. TU performed data cleaning and statistical analysis. All authors interpreted the analytical results. TU and KN drafted the manuscript, and all authors critically revised the manuscript for important intellectual content. All authors read and approved the final version of the manuscript. TU served as guarantor and accepted full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.