Article Text

Abstract
Introduction Guidelines are important tools for supporting quality management in the care of patients with cancer. However, in clinical practice barriers exist to their implementation. Consequently, Quincie aims at: (1) gaining a comprehensive picture of the implementation of quality indicators from the national guideline on palliative care for patients with incurable cancer in palliative care units and (2) describing the factors that facilitate and hinder their implementation to develop recommendations.
Methods and analysis The Quincie study follows a mixed-methods approach across two study phases. In phase 1, routinely collected data of 845 patients with incurable cancer from eight palliative care units in the commuting area of the Comprehensive Cancer Centre Lower Saxony will be analysed, regarding the implementation of 10 quality indicators from the national guideline on palliative care. Structural characteristics of the palliative care units will also be collected. In phase 2, recommendations for the practical implementation of the quality indicators, focusing on the achievement of the quality objectives identified in phase 1, will be developed in an implementation workshop. These recommendations will be subsequently agreed on via a Delphi survey.
Ethics and dissemination Ethical approval has been given by the ethics committee of the Hannover Medical School (first vote, No. 10567_BO_K_2022) and other relevant institutions. The results will provide urgently needed insights on the implementation of the national guideline on palliative care in clinical care and on the factors that facilitate and hinder this implementation. The results are expected to promote better care for patients with incurable cancer. The results will be directly reported to the participating palliative care units and will be published in relevant peer-reviewed journals. They will also be presented at national conferences.
Trial registration number German Clinical Trials Register (DRKS00029965).
- PALLIATIVE CARE
- Adult palliative care
- Health Services for the Aged
- Quality in health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Quincie is the first study that investigates the implementation of quality indicators of the S3 guideline for palliative care on palliative care units in Germany.
For each palliative care unit, an individual procedure for data collection has to be developed depending on the individual respective documentation systems, which may limit comparability but allows for an individual feedback for the participating wards and leads to a novel approach for data collection.
The retrospective analysis of routinely collected data that were not explicitly documented for the purpose of evaluating quality indicators from the S3 guideline on palliative care results in the need for a cautious interpretation.
Given the limited scientific evidence on the proposed inclusion and exclusion criteria for patient data from the palliative care units (eg, length of stay more than three nights), deviations of about 10% may occur from the estimated number of 845 cases.
Introduction
Background
In 2015, the first S3 guideline on palliative care for patients with incurable cancer, including chapters on breathlessness, cancer pain, constipation, depression, communication, the dying phase and care structures, was developed.1 Following amendments and extensions, the revised S3 guideline on palliative care was published in 2019, covering the definition of goals of care and decision-making, fatigue, sleep-related illnesses/nocturnal restlessness, nausea and vomiting (not tumour therapy-related), malignant bowel obstructions, malignant wounds, anxiety and the desire to die.2 3 The current version of the S3 guideline on palliative care includes 11 quality indicators, which were developed in accordance with the Oncologic Guideline Programme.4 These indicators can be used to assess the quality of care structures, processes or results of care and serve as a gold standard in the German palliative care community.3
The main aim of this guideline on palliative care is to improve symptom control and the quality of palliative care for adult patients with incurable cancer, irrespective of the implementation of tumour-specific measures. Additionally, the S3 guideline on palliative care includes the involvement of relatives in all care settings (ie, outpatient and inpatient, general and specialised palliative care).3 Palliative care practice in Germany would benefit from further professionalisation and the development of standards, also by means of the S3 guideline, in order to better complement and integrate clinical experience with scientific evidence. Within medicine, guidelines are considered important instruments for quality assurance and quality management in patient care.3 5 6 Thus, there is a need to integrate the S3 guideline on palliative care into everyday care in a targeted and sustainable manner.
The literature clearly shows that the mere development and existence of guidelines does not necessarily lead to their implementation and application in practice.7 Consequently, guidelines may not always influence (the improvement of) patient care.8 In particular, several factors may reduce the acceptance and application of medical guidelines. Studies have shown, for example, that some physicians have reservations about guidelines that either limit or completely obstruct their practical implementation.9–11 Further evidence suggests that other healthcare professionals may also hold critical attitudes towards guidelines, which may hinder their effective implementation.12 One observational study found a negative correlation between the number of deviations from guideline recommendations and the survival of patients with breast cancer.13 Interestingly, there is also scientific evidence that, while many oncologists are very positive about the guideline on breakthrough pain and believe that these are based on the best available scientific evidence, they do not necessarily follow the guideline in their daily clinical practice.14 At the same time, there are encouraging results from individual disciplines: a German analysis from 2013 on the implementation of the S3 guideline on lung cancer found almost complete conceptual adherence to the guideline in inpatient pneumological and pneumological-thoracic surgical facilities.15 The authors argued that participants’ high pneumological-oncological specialisation was probably decisive in determining their adherence.
Evidence suggests that guidelines are more consistently followed when implementation strategies are tailored to address previously identified barriers and facilitators.16–19 Barriers may include reservations about the use of guidelines,20 as well as organisational barriers, including structural, personnel and possible financial factors.14 21 For example, a lack of easy access to (good) guidelines has been shown to be a central barrier to implementation.22 With regard to the S3 guideline on palliative care, it is not yet known how widespread it has become in practice, and the extent to which it is considered by palliative care providers. Accordingly, there is a need to investigate the facilitating and limiting factors to its implementation.
In 2019, a doctoral thesis was published that aimed at describing the attitudes and opinions of professionals working in palliative care towards guidelines, in general, and the particular S3 guideline on palliative care, more specifically.23 The core findings were that most professionals were very positive about the guideline and, in daily practice, the guideline was widely applied by both physicians (87%) and nurses (70%). Nevertheless, the quality and practical relevance of the guideline were criticised, but the discrepancy between the guideline and palliative care values was considered small.23 These specific findings on the S3 guideline on palliative care in Germany are congruent with national and international findings related to guidelines in other medical disciplines. Although this doctoral thesis provided information on the opinions and perceptions of professionals in palliative care, it did not quantitatively analyse whether—and to what extent—the S3 guideline on palliative care is implemented in palliative care practice, and the extent to which specific quality indicators are documented. To date, there has been no systematic evaluation of the implementation of the national guideline on palliative care for patients with incurable cancer in clinical practice within palliative care units in Germany. The Quincie research project will investigate the frequency and manner in which data concerning quality indicators are documented, as well as the frequency with which quality indicators are fulfilled in clinical practice.
Study aims
The overall objectives will be (1) to gain a comprehensive picture of the practical implementation of the quality indicators in the national guideline on palliative care for patients with incurable cancer in clinical practice within palliative care units in the commuting area of the Comprehensive Cancer Centre Lower Saxony (CCC-N) and (2) to identify factors that hinder and facilitate implementation to formulate consented recommendations.
Specifically, the research will aim at answering the following questions:
Which quality indicators from the guideline on palliative care for patients with incurable cancer are practically implemented within palliative care units in the commuting area of the CCC-N?
How frequently are the quality objectives (according to the indicators) achieved with patients with incurable cancer?
How are the quality indicators and/or their fulfilment documented within palliative care units (eg, in which electronic and/or manual documentation systems, and by which instruments)?
How do the implementation of the quality indicators and the achievement of the quality objectives of individual palliative care units compare to the average for all participating palliative care units, and how does this comparison relate to structural characteristics?
What recommendations can be derived from the analysis of the clinical implementation of the quality indicators, the achievement of the quality objectives and the facilitating and limiting factors for the implementation of the guideline on palliative care units?
With regard to the research questions, the authors have the following hypotheses:
At palliative care units in the commuting area of the CCC-N, some but not all of the ten quality indicators from the S3 guideline on palliative care for patients with incurable cancer are practically implemented.
It is unclear how often the quality objectives according to the quality indicators in the S3 guideline for palliative care are met in patients with incurable cancer.
The data necessary to address the quality indicators and the achievement of the quality objectives are documented in the palliative care units using different documentation systems and by means of different assessment instruments.
There is a heterogeneous picture in the palliative care units in the commuting area of the CCC-N with regard to the implementation of the quality indicators, the achievement of the quality objectives and their respective structural characteristics.
The care for patients with incurable cancer in palliative care units can be optimised by empirical results on the practical implementation of the quality indicators and achievement of the quality objectives of the S3 guideline on palliative care as well as on facilitating and limiting factors for the guideline implementation.
Methods and analysis
Quincie is a 30-month project, ranging from February 2023 to July 2025.
Study design
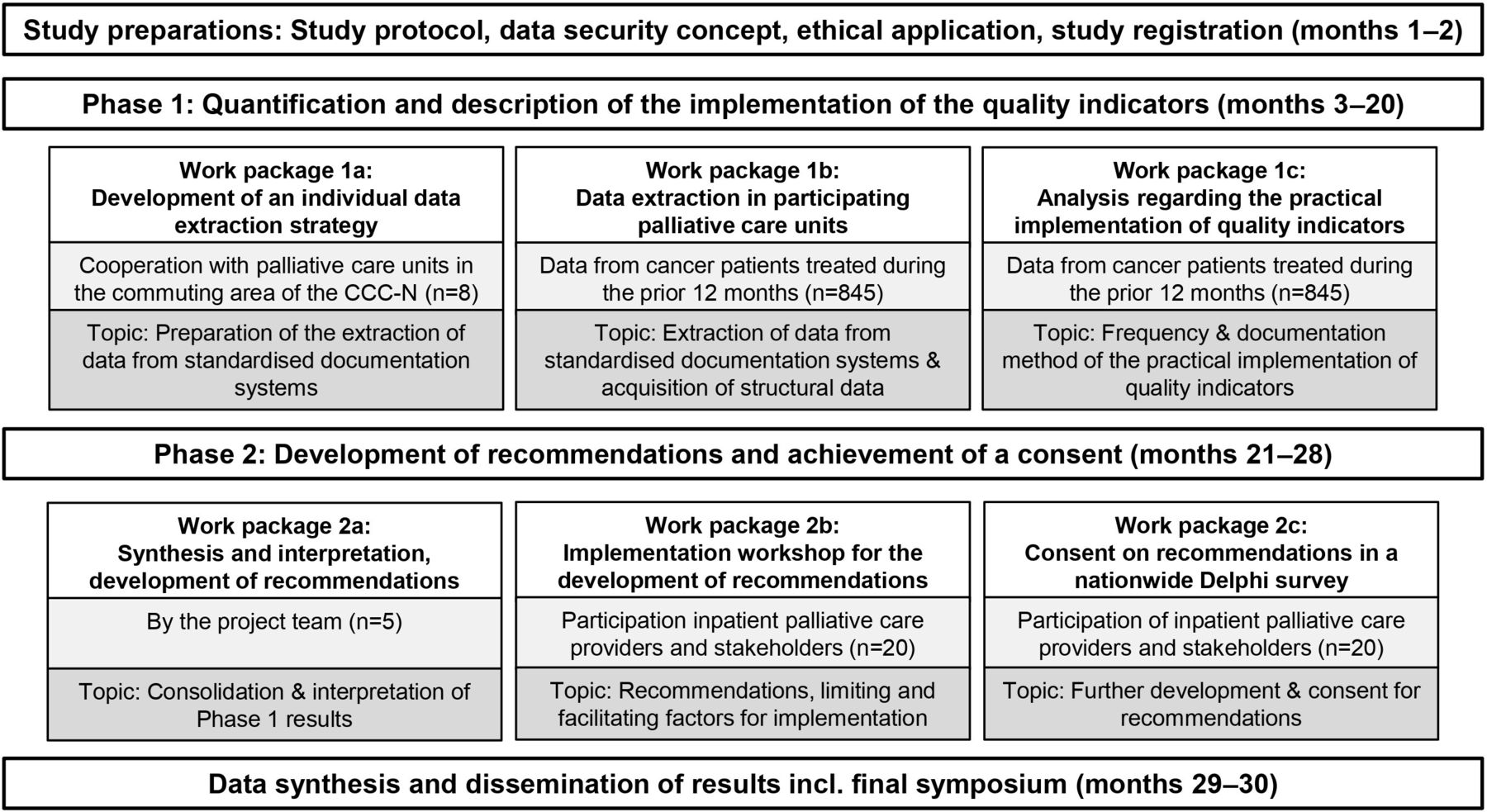
The Quincie study will follow a mixed-methods approach, spread across two research phases, each with three work packages (WP) (figure 1). In phase 1, a retrospective, secondary analysis of routinely collected data from hospital data management systems will be performed through a cross-sectional data collection. Phase 2 comprises an expert workshop and a Delphi study.

{kind=link}
Study design and study phases. CCC-N, Comprehensive Cancer Centre Lower Saxony.
Study setting
In phase 1 of the Quincie study palliative care wards in the commuting area of the CCC-N are addressed. It can be assumed, that palliative care units are well-informed on the recommendations of the S3 guideline for palliative care and that data collection regarding the quality indicators is generally possible. Most of the indicators are especially relevant for inpatient palliative care, which is why the authors focus on this setting.
Two university hospitals in Lower Saxony form the CCC-N since November 2019. The merge of these two university hospitals aims to advance innovative cancer research and to provide cancer patients with the latest scientific findings.24 The CCC-N is one of 14 oncological centres of excellence funded by the German Cancer Aid in Germany. The network of the CCC-N with its partner clinics is an excellent setting for the implementation of phase 1 of the Quincie study.
Data collection
The study preparations will be carried out in the first two project months (February–March 2023). In phase 1 (April 2023–September 2024), a retrospective analysis of routinely collected quantitative patient data from eight palliative care units in the commuting area of the CCC-N will be conducted. In WP 1a, an individual data extraction strategy will be developed for each participating palliative care unit, depending on which documentation systems are used and how the documentation is done (digital in one or more electronic systems/paper-based on different clinical documentation sheets/combination of both). In WP 1b, data extraction will be carried out for each participating palliative care unit. Data from adult patients with incurable cancer who were in inpatient care at one of the palliative care units for at least three nights will be assessed. Primarily, the following ten of the currently eleven available quality indicators in the routine data of the palliative care units will be considered3:
Quality indicator 1: reduction of breathlessness.
Quality indicator 2: reduction of pain.
Quality indicator 3: opioids and laxatives.
Quality indicator 4: symptom assessment in the dying phase.
Quality indicator 5: assessment of agitation in the dying phase.
Quality indicator 6: stopping cancer-specific measures in the dying phase.
Quality indicator 7: oral care.
Quality indicator 8: assessment of malignant wounds.
Quality indicator 9: documentation of goals of care.
Quality indicator 10: screening by means of Minimal Documentation System (MIDOS) or Integrated Palliative care Outcome Scale (IPOS).
The eleventh quality indicator refers to the number of patients with specialist palliative care. In the Quincie project, palliative care wards are observed and all patients admitted to palliative care units received specialist palliative care, which is why the eleventh quality indicator is not applicable. By definition, the eleventh indicator applies to all patients included and does therefore not need to be collected and evaluated.
As an example, the quality indicator 2 ‘reduction of pain’ measures how many patients with moderate/severe pain achieve a reduction in pain within 48 hours of hospital admission. Further information on the recording of the individual quality indicators can be found in table 1.
Quality indicators in the S3 guideline on palliative care3 (adapted)
Additionally, structural data from the participating palliative care units will be assessed, including information on general characteristics of the palliative care unit and the clinic, the number of beds, the number of patients with non-curable cancer per year and staffing ratios. Due to the focus on quality indicators from the national guideline on palliative care in our study, there will be additional questions about existing certifications, quality management, general awareness of the guideline, and the existence of SOPs with and without reference to guideline content. The structural questionnaire will be developed within the Quincie study.
In WP 1c, the extracted data will be analysed regarding the practical implementation of the quality indicators.
In phase 2 (October 2024–May 2025), recommendations for the practical implementation of the quality indicators will be developed on the basis of the phase 1 results, both in the consortium and through an expert workshop. The recommendations will be subsequently agreed on via a multi-round Delphi survey. In WP 2a, the results of WP 1a–c will be synthesised and interpreted by the project team. In WP 2b, the summarised results of WP 1a–c will be presented and discussed in an expert implementation workshop. The discussion will aim at developing recommendations for the further development of quality management within palliative care units. In WP 2c, the developed recommendations from WP 2b will be agreed on through an online Delphi survey. Finally, the project results will be combined in a data synthesis and disseminated in various ways including a final symposium (June–July 2025).
Sample selection
Phase 1: for WP 1a, the project team invited all ten hospitals with palliative care units in the commuting area of the CCC-N to participate prior to the grant application (two university hospitals included in the CCC-N and eight non-university hospitals with palliative care units). Via online research and through existing contacts the person responsible for each palliative care unit was contacted by email, including a brief information about the planned study. Possible queries were clarified by telephone, resulting in a written declaration of intent to participate from eight palliative care units. WP 1b and WP 1c will aim at extracting and analysing, respectively, a total of 845 data sets from adult patients with cancer who were treated at the participating palliative care units during 12 months prior data collection.
Phase 2: in WP 2a, the results from phase 1 will be synthesised by five members of the project team. In WP 2b, approximately 20 inpatient palliative care providers and stakeholders in Germany will participate as experts in an implementation workshop. In WP 2c , similar to WP 2b, approximately 20 inpatient palliative care providers and stakeholders in Germany will participate as experts in a Delphi survey.
Inclusion, exclusion and termination criteria
In phase 1, specific inclusion and exclusion criteria for patient data sets will be applied for the data export. The inclusion criteria will be as follows:
Inpatient stay at a palliative care unit during the 12 months prior data collection.
Aged 18 years or older at the time of admission.
A main diagnosis that includes at least one cancer diagnosis (ICD-10 C00-C97 ‘malignant neoplasms’).
Inpatient stay with a duration of at least three nights.
The exclusion criteria will be as follows:
Death, transfer or discharge prior the end of the third night.
Lack of consent for the scientific use of the data.
Discontinuation of the study in phase 1 is possible in the case of a palliative care unit’s withdrawal of consent.
Given the abovementioned inclusion and exclusion criteria, and proceeding from the total of 65 beds within the eight participating palliative care units, a sample size calculation prior to the grant application estimated a total of 845 patient data sets for analysis. Approximate values from the palliative care unit of the Hannover Medical School were used for the sample size calculation, for example, in relation to ward occupancy, length of hospital stay, patient characteristics and agreement to use data for scientific purposes.
In phase 2, WP 2b, 20 inpatient palliative care providers and stakeholders in Germany will participate as experts in an implementation workshop. Given an anticipated drop-out rate of 10%, at least 22 experts will be invited to participate. Experts from all fields and professions relevant to inpatient palliative care will be invited, to recruit a group as heterogeneous as possible. These may include clinical specialists (eg, medical and nursing managers in palliative care units) and stakeholders at the meso and macro levels of the healthcare system (eg, staff from associations, professional societies and CCCs). Also, two cooperating experts and supporters involved in the grant application will be included. In WP 2c, similar to WP 2b, approximately 20 inpatient palliative care providers and stakeholders in Germany will participate as experts in a Delphi survey. In phase 2, a withdrawal of experts’ consent during data collection will terminate their participation.
Sample size calculation
A written declaration of intent to participate was obtained from eight palliative care units with a total of 65 palliative care beds. These units formed the basis for the sample size calculation. Literature indicates that approximately 90% of all patients in palliative care units in Germany have cancer and that the average length of stay is 10.6 days.25 For the further inclusion criteria in the Quincie study, data of the palliative unit at the Medical School Hannover from the year 2021 were used in order to calculate the sample size.
Average length of stay of 11 days per bed per year: 365/11 days=33 (one bed can be occupied 33 times per year).25
80% occupancy of the palliative unit: 80×33/100=26.
70% of these patients have a stay duration of at least 2 weeks. Three nights: 70×26/100=18.
90% of these patients have cancer: 90×18/100=13.25
A total of 65 beds on 8 participating palliative units: 13×65=845.
With the expected participation of eight palliative units, a total of 845 patient data sets is expected to be included in the analyses in phase 1 of the Quincie study.
Data analysis
In phase 1, quantitative analysis of routinely collected data that provide information on the achievement of quality indicators will be carried out descriptively by frequency analysis using IBM SPSS Statistics, Version 29. The descriptive analyses take gender and age-specific aspects of in the patient data as well as structural characteristics of each cooperation palliative care unit into account. Since we assume that no or a few quality indicators are systematically recorded in the routine documentation at all, no standardised analysis plan exists prior to data collection. Individual steps will be required to make the existing documentation usable for data analysis. The first step is therefore to record for each participating palliative care unit how and with which systems the patient data is documented and which symptom assessments are used. This information will be recorded in protocols of appointments and other conversations with the cooperating palliative care units. Afterwards, the individual documentation is reviewed by members of the study team with each participating palliative care unit and target variables from routine documentation or from symptom assessments are defined to help answer the research questions. To find out whether the quality indicators have been implemented, the corresponding numerator and denominator (see table 1) for each indicator are determined from the documentation/targeted variables and compared with each other. Depending on the format of the data, the evaluation procedure may be adapted. As a basis for data collection, a documentation file including information on inclusion and exclusion criteria, documentation and documentation systems, systematic survey of quality indicators, as well as data on each quality indicator, its documentation, numerator, denominator and screening instruments will be used, which might be adapted for each palliative care unit.
As a result of phase 1, an individual evaluation for each cooperating palliative care unit will be created, visualising (1) how often quality indicators from the S3 guideline on palliative care have been implemented and (2) whether the quality objectives were achieved.
Beyond the descriptive analysis, multilevel logistic regression analyses will be performed to evaluate the influence of different structural characteristics as well as the influence of patient characteristics on the implementation of quality indicators and the achievement of quality objectives. Data includes the collected structural characteristics (eg, staffing ratio, guideline awareness) and patient characteristics (eg, age, gender, diagnoses). Target variables are the results regarding the quality indicators based on routinely collected data in phase 1 from patients treated at the cooperating palliative care units.
Qualitative data from the implementation workshop in phase 2 WP 2b will be transcribed verbatim from the audio record and analysed qualitatively using MAXQDA (VERBI Software Consult Sozialforschung GmbH, 1989–2020), based on the methodological principles of qualitative content analysis.26 The key subjects regarding the practical implementation of the quality indicators identified in phase 1 will comprise an a priori category system, which will be successively expanded with workshop data.
Quantitative data from phase 2, WP 2c, will be processed using IBM SPSS Statistics, Version 29. Recommendations from the first Delphi round that receive support from at least 80% of participants (on the basis of the scale responses ‘I rather agree’ and ‘I fully agree’) will be considered consented.27 The results will be calculated by means of a frequency analysis. Recommendations that fail to achieve consent in the first Delphi round will be revised according to participants’ free text comments and included in a second Delphi round. Following this, the revised recommendations will be sent to all participants who completed the first Delphi round for a second online evaluation. A third round will be applied, if necessary, following the same procedure.
Expected results
The Quincie project will generate relevant new and urgently needed scientific knowledge to support the practical implementation of the S3 guideline on palliative care within German palliative care units. The identification of limiting and facilitating factors for the implementation of the guideline will stimulate the development of targeted recommendations to improve implementation. These recommendations can support the direct transfer of the results into clinical practice, thereby promoting the best possible care for patients with incurable cancer. In addition, the participating palliative care units and cooperating clinics will be able to review their individual results in order to reflect on their quality of treatment and potential for further improvement. The results may also be used for the certification of palliative care units. It can be assumed that the limiting and facilitating factors identified for the implementation of the guideline will be transferable to other university and non-university palliative care units, enabling a national transfer of the recommendations to improve implementation. Due to the foundation on widely accepted quality indicators which are based on international literature, the results might partially be transferable to other palliative care units from other hospitals and in other federal states. However, crucial differences exist between healthcare systems and need to be taken into account.
Quincie is the first study that investigates the implementation of quality indicators of the S3 guideline for palliative care in palliative care units. This investigation includes the manner of documentation and the evaluation of the success rate of these quality indicators. Whether the evaluation of quality indicators really allows to draw conclusions on the implementation of the guideline as a whole needs to be discussed. Since it is assumed that the quality indicators are not systematically and explicitly assessed in clinical practice, the mixed-methods approach makes it possible to examine the state of the art (quantitative/retrospective) and, at the same time, to develop new insights and recommendations for improving the documentation and usability of the quality indicators (qualitative).
For each palliative care unit, an individual procedure of data collection will be developed depending on the individual respective documentation systems, which may limit uniformity and comparability but allows for an individual feedback for the participating wards. In the Quincie project, a retrospective analysis of routinely collected clinical data that were not explicitly documented for the purpose of evaluating quality indicators from the S3 guideline on palliative care will be conducted. Consequently, the project data might have been documented unsystematically, and must be interpreted with caution. Given the limited scientific evidence on the proposed inclusion and exclusion criteria for patient data from the palliative care units (eg, length of stay more than three nights), approximate values were used to calculate the sample size. Thus, deviations of about 10% may occur from the estimated number of 845 cases.
The present study protocol describes the purpose, significance and scope of the Quincie research project, as well as its research design. The systematically developed recommendations that will be generated in this project are expected to improve inpatient palliative care for patients with incurable cancer in Germany.
By publishing the present study protocol, the authors aim at promoting research transparency, beyond that which was achieved through registration in the German Clinical Trials Register. The study protocol will serve as a point of reference for the Quincie project team, as well as for the scientific community and other parties interested in the scientific and ethical aspects of the research. Finally, the publication of the study protocol may prevent unnecessary duplication.
Ethics and dissemination
Ethical approval and consent to participate
The clinics have agreed to participate and support the Quincie project by issuing a letter of intent prior to the start of the project. The authors submitted the study protocol to the ethics committee of Hannover Medical School. Ethical approval was obtained from the ethics committee of the Hannover Medical School (first vote, No. 10567_BO_K_2022), the Medical Association of Lower Saxony (No. Ar/050/2023), the University Medical Centre Göttingen (No. 33/4/23 Ü) and the Ethics Commission Westfalen Lippe (No. 2023-248-b-S).
Data security
Prior to the start of data collection at the cooperating palliative care units, contracts are concluded in close cooperation with the data protection officer of the Hannover Medical School in order to safeguard data protection in accordance with the General Data Protection Regulation.
The data protection officer of the Hannover Medical School confirmed that the study meets all data protection laws. All personal data will be treated in accordance with the German General Data Protection Regulation. All data collected in the course of the study will be subject to confidentiality, and all members of the project team will be bound to data secrecy. The data collected from all WP will be pseudonymised and stored in accordance with the applicable data protection guidelines. Furthermore, they will be exclusively analysed with regard to the objectives stated in the project proposal. All participating palliative care units, healthcare providers and stakeholders will be informed (verbally and in writing), in detail, about the aims and purpose of the Quincie research project in advance of data collection. Participation will only begin after participants express their consent (phase 1, WP 1a–c; phase 2, WP 2c) or provide additional written informed consent (phase 1, WP 1a–c; phase 2, WP 2b). Written information will be provided to all participants. Each participant will have the right to refuse or terminate participation at any time, before or during the data collection, without providing a reason.
Dissemination and implementation
If desired, individual feedback can be provided to each participating palliative care unit after data analysis to discuss the individual results in comparison to the other palliative care units. This enables direct transfer of the results into clinical practice for the participating palliative care units and, if necessary, allows adjustments to be made after the first project phase. Individual results can also be re-used for certification purposes by the palliative care units.
The intended implementation workshop and Delphi process in phase 2, as well as a final project symposium (which will be attended by national experts, among others), will promote the dissemination of the results and underline the relevance of the project to clinical palliative care practice. Thus, in addition to having a direct influence on palliative care units in the commuting area of the CCC-N, the project results may also guide the further development of palliative care throughout Germany. Both, the expert workshop and the symposium offer a great chance for all participants to network and strengthen collaboration.
To promote the accessibility and long-term safeguarding of the research data and results, the project team will report comprehensively and transparently on the project and, irrespective of the findings, publish in national and international publications (under an open access license, where possible). In addition, the project team is willing to make digital research data, as well as research data protected by data protection and copyright, available for secondary use, in response to verifiably justified requests.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge Valerie Appleby’s editorial review of the study protocol.
References
Footnotes
Contributors KvB and SS developed the original study plan, wrote the grant application and obtained funding for the research project. KvB and SS wrote the first draft of the study protocol on the basis of the original German grant application. AE and FS contributed to the writing. All authors enhanced the quality of the manuscript by revising it critically. All authors read and approved the final manuscript.
Funding This work is supported by the German Cancer Aid (Grant number 70115061). The funding body does not have any influence on the design of the study and collection, analysis and interpretation of data or on writing the manuscript. This publication was supported by the publication fund NiedersachsenOPEN, funded by zukunft.niedersachsen.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.