Article Text

Abstract
Objective To assess the effect of the COVID-19 pandemic on people experiencing incarceration (PEI), focusing particularly on clinical outcomes compared with the general population.
Design Systematic review with narrative synthesis in accordance with the Centre for Reviews and Dissemination’s good practice guidelines.
Data sources Medline, Social Policy and Practice, Criminology Connection, ASSIA, EMBASE, SCOPUS, Web Of Science, CINAHL, Cochrane Library, Cochrane COVID-19 reviews, COVID-19 Evidence Reviews and L*OVE COVID-19 Evidence databases were searched up to 21 October 2022.
Eligibility criteria for selecting studies We included studies presenting data specific to adults ≥18 years experiencing incarceration, with exposure to SARS-CoV-2 infection. All studies with a comparison group, regardless of study design and country were included. Studies with no comparison group data or not measuring clinical outcomes/health inequalities were excluded. Studies focussing on detained migrants, forensic hospitals, prison staff and those not in English were also excluded.
Data extraction and synthesis Two reviewers extracted data and assessed risk of bias. Data underwent narrative synthesis using a framework analysis based on the objectives, for infection rates, testing, hospitalisation, mortality, vaccine uptake rates and mental health outcomes. There was no scope for meta-analysis, due to the heterogeneity of evidence available.
Results 4516 references were exported from the databases and grey literature searched, of which 55 met the inclusion criteria. Most were from the USA and were retrospective analyses. Compared with the general population, PEI were usually found to have higher rates of SARS-CoV-2 infection and poorer clinical outcomes. Conflicting data were found regarding vaccine uptake and testing rates compared with the general population. The mental health of PEI declined during the pandemic. Certain subgroups were more adversely affected by the COVID-19 pandemic, such as ethnic minorities and older PEI.
Conclusion PEI have poorer COVID-19 clinical outcomes than the general public, as shown by largely low-quality heterogenous evidence. Further high-quality research of continuing clinical outcomes and appropriate mitigating interventions is required to assess downstream effects of the pandemic on PEI. However, performing such research in the context of incarceration facilities is highly complex and potentially challenging. Prioritisation of resources for this vulnerable group should be a focus of national policy in the event of future pandemics.
PROSPERO registration number CRD42022296968.
- COVID-19
- PUBLIC HEALTH
- MEDICAL ETHICS
- Epidemiology
- INFECTIOUS DISEASES
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Systematic review presenting evidence published during the first 30 months of the COVID-19 pandemic for outcomes in people experiencing incarceration (PEI) worldwide.
The study used comprehensive search terms applied to 12 databases to collate evidence from both high-income and low/middle-income countries and focussed on objective data relating to clinical outcomes making comparisons, both within incarceration facilities and with the general population.
High-quality evidence was lacking about the COVID-19 outcomes of PEI—many studies were of low quality, relying on third-party observational data and prone to bias.
Published data were heterogeneous with varying statistical measures, meaning meta-analysis was not feasible.
Studies were excluded if not published in English, potentially leading to some selection bias.
Introduction
People experiencing incarceration (PEI) were particularly likely to be impacted by the COVID-19 pandemic but the extent and range of impacts and effects on pre-existing inequalities in health compared with the general population are not fully understood.1 2 Health inequalities are unequal and disadvantageous differences in the health of different populations, such as life expectancy or access to healthcare, which are socially determined.3 PEI have a high prevalence of physical and psychiatric morbidity, with many coming from marginalised backgrounds, experiencing homelessness or with limited educational backgrounds.1 4–6 There are complex social problems, including being deprived of liberties, a lack of social and familial support and violence, each contributing to ill health.2 5
When the COVID-19 pandemic began, high transmission rates were seen in incarceration facilities.7 PEI are susceptible to infectious diseases due to many factors, including living in confined crowded spaces.1 2 Incarceration facilities raise difficulties with social distancing and lesser access to hygiene products and personal protective equipment.8 Prolonged isolation in cells contributed to declines in mental health of PEI during the pandemic.9–11 Family visits were also suspended, court hearings delayed and educational programmes cancelled.9 12
The pre-existing health inequalities and increased risk of transmission suggest a greater risk for PEI from COVID-19. High prison COVID-19 death rates were seen in the UK—3.3 times greater than for the same age and sex in the public.13 Internationally, data from the USA show that PEI are more likely to require vasopressors when hospitalised with COVID-19 and have a higher in-hospital mortality rate than the general population.14 It is possible that rates of long COVID, a condition characterised by a range of manifestations across organ systems, including fatigue, shortness of breath and cognitive impairment persisting 12 weeks after onset of COVID-19 symptoms, may be more prevalent in PEI.15 16 However, comprehensive research on this population is lacking.
An earlier systematic and scoping review were undertaken assessing the effect of COVID-19 in PEI.17 18 These reviews appraise the evidence base regarding COVID-19 outcomes worldwide, published up to mid-October 2021 and in the USA only, up to February 2022, respectively. An up-to-date review of the cumulative literature base in this field is needed, to understand the impact and identify lessons for further pandemics or cycles of COVID-19.
This systematic review aimed to assess the effect of the COVID-19 pandemic on PEI. The objectives were to assess the following clinical outcomes of the COVID-19 pandemic, comparing them to the general population: infection rates of SARS‑CoV‑2/COVID-19, testing rates, hospitalisation, mortality, COVID-19 vaccine uptake and mental health outcomes. We also sought to evaluate whether inequalities between PEI and the general population widened during the pandemic and, if identified, to investigate potential reasons for this in relation to mediators of COVID-19 and risk factors faced in prisons.
Methods
This systematic review was conducted in accordance with the Centre for Reviews and Dissemination’s good practice guidelines.19 Guidance from stakeholders assisted with developing the eligibility criteria. We excluded studies focussing on detained migrants, forensic hospitals and staff; also studies published pre-pandemic, not in English or lacking comparison groups. The inclusion and exclusion criteria for selecting eligible studies are shown in table 1.
Criteria for including and excluding studies in this review
12 databases were searched, including health, criminology, sociology and COVID-19 specific databases (Medline via OVID, Social Policy and Practice via OVID, Criminology Connection via ProQuest, ASSIA via ProQuest, EMBASE via OVID, SCOPUS, Web Of Science, CINAHL, Cochrane Library, Cochrane COVID-19 reviews, COVID-19 Evidence Reviews, L*OVE COVID-19 Evidence). Preprints were searched via the online EMBASE database to minimise publication bias.
A ‘COVID-19’ search string, developed for use by the Wales COVID-19 Evidence Centre, and a ‘people experiencing incarceration’ search string, developed by the authors, were combined. The full search strategy is provided in online supplemental appendix 1. Grey literature suggested by stakeholders was screened to reduce publication bias and gain early insight from unpublished work. Databases were searched up to 21 October 2022.
Supplemental material
Search outputs were exported onto a reference management software, Endnote,20 and screened for eligibility by DBW and BS (table 1). Approximately 10% of the screening was duplicated by other reviewers (FB and AE), with differences in outcomes discussed, to ensure consistency. Disagreements occurred in approximately 2% of the screening process and were resolved through consensus discussion.
Full texts of references selected based on title and abstract were retrieved for analysis by DBW and BS. Assessment by a second reviewer (AE) was completed for 5% of full texts with disagreements occurring in approximately 1% and resolved through consensus discussion.
Data were extracted into Microsoft Excel. Headings included: Study Title and Authors, Country of Study, Study Type, Aim of Study, Participants and Setting, Data Collection, Exposure, Study Outcomes and Methodological Appraisal (online supplemental appendix 2).
Supplemental material
Critical appraisals of included studies were conducted using a Joanna Briggs Institute checklist based on study design.21–23 From an initial literature scoping exercise it was hypothesised that most studies would be low-quality. All studies meeting the inclusion criteria were included, rather than excluding low-quality evidence.
External validity assessment was undertaken by commenting on study limitations. An overall quality of evidence assessment was done for each study, through analysis of critical appraisals, the methodology and key limitations. The assessment graded the studies as low-quality, medium-quality or high-quality evidence. Where preprint articles were found, efforts were made to access subsequent peer-reviewed published versions, used the latter’s data in preference to preprint data.
A narrative synthesis of the results was conducted. There was no scope for meta-analysis, due to low-quality heterogeneous evidence available. Data were synthesised using a framework analysis,24 based on the objectives, for infection rates, testing, hospitalisation, mortality, vaccine uptake rates and mental health outcomes. We analysed potential mediators of COVID-19 outcomes, such as age or ethnicity, if the data were available.
Patient and public involvement
None.
Results
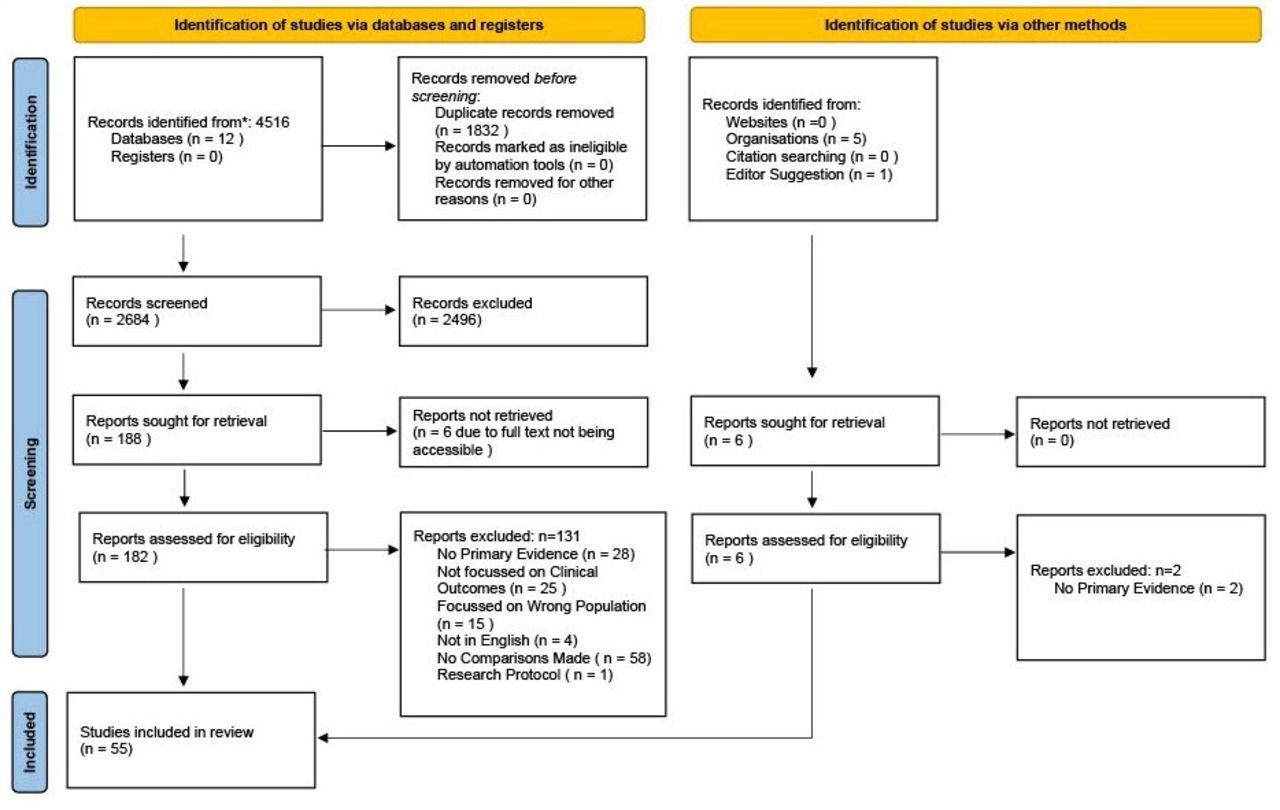
A total of 4516 references were exported from the databases searched. After de-duplication, 2684 references remained. Following screening of titles and abstracts, 182 articles were retrieved for full-text analysis, from which 51 studies were included. Six resources from grey literature were identified of which four were included. Reasons for exclusion were documented (see figure 1).25 Therefore, 55 studies were included (see online supplemental appendix 2).

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses chart of included studies.
Studies were included from USA (36, 65.4%), UK (5, 9%), Canada (3, 5.4%), Italy (3, 5.4%), Denmark (2, 3.6%), Brazil (2, 3.6%), China (1, 1.8%), Ethiopia (1, 1.8%), France (1, 1.8%) and Switzerland (1, 1.8%). Study designs included were 29 retrospective analyses of data (52.7%), 8 retrospective cohort studies (14.5%), 7 longitudinal studies (12.7%), 6 cross-sectional studies (10.9%), 3 outbreak reports (5.5%), 1 matched case–control study (1.8%) and 1 policy analysis (1.8%).
Infection rates of COVID-19/SARS-CoV-2 in PEI
Incidence of COVID-19/SARS-CoV-2 varied significantly across countries and prison facilities. Crude incidence rates were mostly higher in prisons than in the general population.26–36 Relative risk of COVID-19 positivity versus the general population was increased by 4.32 times37 and 5.29 times.36 However, a UK study documented a crude incidence rate in prisons which was not statistically different to the general population38 and four studies, from the UK, USA, Italy and Denmark, respectively, showed a lower incidence rate in the incarcerated population.39–42 Testing strategies were not clearly documented in these studies, so results must be interpreted with care. Analysis often used population estimates, which are not accurate.
Conflicting evidence was found about the seropositivity levels of PEI compared with the general population. A study in Paris, France found 18.4% positivity rates compared with 20.6% in the general Parisian population.43 However, in Montreal, Canada 22% of participants were seropositive over the study period compared with 13.75% in a comparator general population sample of Montreal blood donors.44
Although the incidence of COVID-19 was greater among PEI than in the community, some subgroups of incarcerated residents were at greater risk of seropositivity and COVID-19 incidence. Risk factors for contracting COVID-19 in PEI included Hispanic ethnicity,36 45–47 being of non-Hispanic black ethnicity,36 38 44 46–48 Asian ethnicity,38 partaking in prison labour,44 49 being in high occupancy prisons,32 unstable housing prior to incarceration44 shared meal consumption44 and older age.47 50 Higher security prisons had lower per capita rates of infection.37 There was conflicting evidence about type of accommodation and risk factors for COVID-19. Some studies found dormitory housing was a risk factor,32 45 49 while another found no differences compared with single cells.44 Working or residing in a prison also increased the risk of secondary detection of COVID-19, 90 days after primary infection, by almost five times compared with the public.51
Correlations were seen between case rates in staff, incarcerated residents and in the wider community.34 37 52 A US study demonstrated that once community rates reached a threshold case rate of >50 per 100 000, there was an immediate increase in the COVID-19 case rate in prisons by 118.55 cases per 100 000 (95% CI −3.71 to 240.81).34 A rise in staff cases was associated with a rise in cases among PEI.52 Areas of rurality and with higher economic distress scores had higher rates of COVID-19 outbreaks in local prisons.48 One study noted time lagged an average of 1–2 weeks between peaks of infection rates in the general population and the prison population.40
The overall quality of evidence about infection rates of COVID-19 in the prison population was low. See table 2 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing infection rates of COVID-19/SARS-CoV-2 in PEI versus the general population
Testing for COVID-19 in PEI
Testing for COVID-19 in prisons varied, even within countries. In the USA and Canada prisons tested on average more than the general population, but this varied between states and provinces.29 31 53 Blair et al presented conflicting Canadian data relating to comparatively high testing rates in a few prisons with COVID-19 outbreaks.29 Some facilities had no access to testing early in the pandemic, but this improved as the pandemic continued.29 53 One study in Lombardy, Italy noted higher mean weekly testing rates per 1000 individuals in PEI compared with the general population through both first and second waves (61.09 vs 6.11 and 258.43 vs 19.73, respectively).35 Conflicting data was found in a whole population Danish study which noted lower testing rates in PEI compared with the general population (OR 0.47 95% CI 0.46 to 0.48, p<.0001).42
Older PEI (age ≥55 years) had higher testing rates than younger counterparts.50 Screening of people newly experiencing incarceration increased during the pandemic.46 Test positivity (percentage of tests that were positive) was also greater in prisons than public settings.31 46 Thus the more testing was undertaken, the more COVID-19 cases were identified, with higher incidence rates.30 53 Testing strategies (eg, asymptomatic testing at defined intervals vs symptomatic testing) were generally not documented so results should be interpreted with caution.
Evidence was graded low-quality or medium-quality, with most studies reporting retrospective publicly available data, with comment on testing strategies limited. See table 3 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing testing of COVID-19/SARS-CoV-2 in people experiencing incarceration (PEI) versus the general population
Hospitalisation from COVID-19 in PEI
PEI had worse hospitalisation outcomes than the general population. A whole population Danish study found that PEI were nearly two times as likely to be hospitalised with COVID-19 (adjusted incidence rate ratio (aIRR) of hospitalisation within 14 days diagnosis 1.99, 1.64–2.40) and over twice as likely to be admitted to intensive care (aIRR of intensive care admission within 14 days 2.41, 1.56–3.72).42 A large US study also found higher rates of hospitalisation, mechanical ventilation requirement, readmission for COVID-19 within 30 days of hospital discharge and longer stays following admission for COVID-19.54 Overall, PEI presented later with more severe disease than the general population.14
However, two US studies found conflicting results with no significant differences in admission to intensive care or intubation rates.14 55 This evidence was weaker, though, with a combined sample size of approximately 800 individuals from three hospital sites for both studies, compared with a total cohort of 4 412 382 individuals encompassing the entirety of the general population and prison population in the Danish study and a total cohort of 1 257 250 encompassing 3415 incarcerated people in the US study.42 54 There was conflicting evidence on whether COVID-19 positive PEI required greater use of vasopressors than the general population.14 55
Certain subgroups of PEI were more likely to be admitted to hospital. Risk factors for being hospitalised with COVID-19 in PEI included heart disease53 and older age.45 54 56 Risk factors for admission to intensive care included autoimmune diseases and older age.45
Access to healthcare for PEI potentially decreased during the pandemic, with fewer admissions to hospital than usual.57 The reduction in elective procedures was greater among PEI than in the public, widening health inequalities.57 Only urgent cases in PEI, such as cancer and dialysis, were prioritised, potentially leading to a backlog in other medical problems.57
Evidence was graded low-quality or medium-quality, with most studies reporting retrospective publicly available observational data prone to inaccuracy. See table 4 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing hospitalisation from COVID-19 in PEI versus the general population
Mortality from COVID-19 in PEI
Standardised morality rates (SMR) from COVID-19 were higher in PEI than in the public, though this varied between and within countries.13 26–28 58 In England and Wales, PEI had an SMR of 3.3, that is, a 3.3 times increase in COVID-19 deaths in prisoners compared with the public.13 Two US studies noted SMRs of 4.45 and 2.89 in PEI.59 60 Death within 60 days of COVID-19 diagnosis was over three times more likely in the Danish prison population population compared with the general population (aIRR 3.11, 95% CI 1.93 to 5.03).42 COVID-19 contributed to a reduced life expectancy among PEI,61 62 quantified at 4.2 years versus 1.5 years in the general population in one US study.59
PEI admitted to hospital had a higher in-hospital mortality rate compared with the general population.14 54 Crude mortality rates in prisons were often equal to, or less than the community,26 29 38 39 53 55 58 63 although these were not standardised (eg, for age). Deaths from COVID-19 disproportionately affected non-Hispanic black, Hispanic and older PEI.45 50 62 64 All-cause mortality in PEI increased compared to pre-pandemic.61 62
Evidence was graded as low-quality or medium-quality, due to many reporting crude mortality rates, rather than standardised rates. See table 5 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing mortality from COVID-19 in PEI versus the general population
Vaccine uptake among PEI
Evidence regarding vaccination uptake was conflicting. A large US study of 126 413 PEI reported a slightly higher rate of full vaccination (33.4%) compared with the general population (29.5%).65 Incarcerated residents also had more time eligible for vaccination in the community (79 days, IQR: 41–183) than in jail (14 days IQR: 3–31) and were 12.5 times (95% CI 10.2 to 15.3) more likely to consent to and receive vaccination while incarcerated than before incarceration.66 Conversely, a Public Health Scotland report found that uptake of a full course of COVID-19 vaccine in PEI was lower than in the public.67 This finding was echoed by a Danish whole population study demonstrating that PEI during 2020 in Denmark were half as likely to complete a full course of COVID-19 vaccination as the general population (aIRR 0.5 95% CI 0.5 to 0.5).68
Two studies highlighted the importance of re-offering vaccines to PEI with significant numbers accepting the second time, after having previously declined a dose.69 70 PEI were more likely to accept vaccination if they were older, had comorbidities associated with severe COVID-19 illness, a higher level of education, identified as white or Hispanic ethnicity, were not born in the USA, had experienced prior SARS-CoV-2 infection, were involved in working activities in the prison or resided in shared rooms.50 65 69–71
Factors correlating with lower vaccine uptake included declining additional information about COVID-19 vaccine, non-Hispanic black or Asian ethnicity.65 71 Worrying about side-effects and wanting more information were reasons why vaccines were not accepted by some.72
Conflicting evidence was noted around the role of female sex in vaccine uptake: one study71 reporting increased uptake of vaccination but another US study noting lower uptake.65
Vaccination policy, which varied significantly between US states, appeared to affect uptake.72 Facilities with similar risk factors, such as long-term care facilities, were prioritised in ‘phase 1’ in all vaccine plans. State plans did not usually specify in which phase PEI should be vaccinated, and only 22% of plans included them in ‘phase 1’.72 One study showed that US states with policies that prioritised vaccination for PEI had higher vaccination rates compared with other states over time. In states with no prioritisation policy, vaccination rates were lower among PEI than for the general population.73
Evidence on vaccine uptake was low-quality, with limited comparisons to the general population and may not be generalisable to other prison populations. See table 6 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing COVID-19 vaccine uptake among PEI versus the general population
Mental health outcomes of PEI during the COVID-19 pandemic
Overall, deteriorating mental health of PEI during the pandemic was reported. Depression and anxiety scores worsened from pre-pandemic comparisons.10 74 75 There was a significant increase in suicide attempts and self-harm events in a Swiss prison comparing 2020 to 2016–2019.76 One study from China noted worsening levels of anxiety in those with no pre-pandemic mental health diagnoses but an improvement in anxiety scores in those with a pre-pandemic diagnosis.77 An Ethiopian study reported high rates of major depressive disorder (66.4% vs 41.9%−56.4%) and generalised anxiety disorder (66.9% vs 36.1%) among PEI compared with pre-pandemic studies.75
Evidence about the mental health was low-quality, due to small sample sizes with limited demographics noted. Instruments to measure mental health outcomes were often heterogeneous between studies and self-reported. Studies lacked general population comparison groups. See table 7 for a summary of key papers comparing outcomes of PEI versus the general population.
Key papers comparing mental health outcomes among people experiencing incarceration (PEI) during the COVID-19 pandemic
Discussion
Principal findings
PEI had higher infection rates and worse COVID-19 clinical outcomes, including hospitalisation, mortality and mental health outcomes, compared with the general population. People with black and Hispanic ethnicity had worse COVID-19 outcomes overall compared with their white counterparts. Older PEI showed poorer outcomes across several domains including higher COVID-19 incidence, testing rates, hospitalisation and mortality related to COVID-19. Testing rates varied greatly between institutions and countries.
Evidence regarding vaccine uptake was conflicting. Prioritisation of incarcerated populations for vaccination varied between countries and regions. Poorer access to healthcare and not always being prioritised for vaccination contributed to widening of health inequalities in an already under-served population.57 72
Significant health inequalities have been demonstrated. There is a suggestion that health inequalities may have widened—several studies demonstrated worsened mental health outcomes and all-cause mortality rates compared with pre-pandemic data in PEI.10 61 62 74–77 However, there are insufficient longitudinal studies comparing outcomes pre-/post-pandemic with the general population to confidently determine whether pre-existing inequalities between PEI and the general population widened during the pandemic.
Context of other literature
This review supports other literature showing that PEI have poor outcomes and high transmission rates from infectious disease, and specifically COVID-19. Incarceration facilities and pre-existing conditions suffered by many PEI facilitate spread of infectious diseases.2 The pre-pandemic infectious disease burden in prisons was high including tuberculosis, hepatitis and other communicable disease, now exacerbated by COVID-19.78 79
The reasons behind poorer outcomes from COVID-19 in PEI are likely to be complex and multi-factorial. Evidence suggests an interplay of overcrowding, limited healthcare access, pre-existing health conditions and higher respiratory illness risk factors, lack of continuity of care and reduced preventative measures such as lower vaccination rates and poorer health education.1 40 49 62 80–85
Prevalence of long COVID in PEI remains a notable absence from published literature. A lack of long-duration longitudinal/cohort studies is a contributory reason for this. A systematic review of long COVID prevalence in the general population noted a pooled estimate of prevalence between 13.6% and 43.9%, depending on definition and method of measurement.86 The review also noted increased prevalence in hospitalised patients.86 Given the increased hospitalisation rates and poorer COVID-19 outcomes evident in PEI, long COVID burden in PEI is likely to be substantial.
Two prior systematic reviews assessed the impact of COVID-19 in PEI, with evidence up to October 2021,17 and February 2022.18 Findings from the more recently published data included in our review are consistent with those of the previous reviews, suggesting that the disparities in outcomes (infection rates, hospitalisation rates and outcomes and mortality) have persisted and not been mitigated. A prior scoping review specifically assessed mental health outcomes of PEI during the COVID-19 pandemic, also showing worsening mental health outcomes.11 Data from a whole population Danish study, however, found comparable rates of self-harm among PEI who tested positive for SARS-CoV-2 compared with those who did not.87
The present review’s findings appear consistent with other systematic reviews in minoritised groups. Ogbonna et al reviewed COVID-19 outcomes in people experiencing homelessness, demonstrating higher rates of hospitalisation, increased mortality rates, lower vaccination rates and poorer mental health outcomes compared with the general population.88 Several authors have noted a higher COVID-19-related mortality rate in residents of long-term care facilities.89 90 Though these two groups are clinically and epidemiologically distinct from PEI, there are multiple common factors evident. A whole population Danish study also demonstrated higher rates of adverse outcomes such as hospitalisation, intensive care admission and mortality in subjects with a low educational level, and those with a history of substance misuse, psychiatric admission or severe mental health illness.42
Implications for policy and practice
PEI are a vulnerable population who could benefit from implementation of mitigating interventions and better access to healthcare. Given the poorer outcomes shown, this vulnerable group should be prioritised in national policy in the event of further waves of COVID-19 or for different potential future pandemics. Where vaccines exist, vaccination is essential to improving COVID-19 outcomes in PEI. Prioritisation for vaccination in this vulnerable group significantly increased vaccine uptake to levels above that of the general population and should be integral to future vaccine policy.73 Education about vaccine importance and re-offering vaccines to people who previously declined are also warranted.69 70
Certain minoritised groups including non-Hispanic black, black ethnic minority groups and older PEI had poorer outcomes following COVID-19 infection.47 48 50 64 The burden of COVID-19 in prisons in rural and socio-economically disadvantaged areas was also higher.48 Mitigation strategies are required for these vulnerable groups and areas.
Mental health outcomes deteriorated during the COVID-19 pandemic for PEI. Further support is necessary, considering the high baseline psychiatric morbidity in prisoners, and the decline seen during the pandemic.11
Further research
High-quality evidence was lacking about the COVID-19 outcomes of PEI. Many studies were of low quality, relying on third-party observational data, and prone to bias. No research on longer-term outcomes such as long COVID was identified but this is needed to assess the full effect of the pandemic on PEI. Longer-term data will also help to quantify whether health inequalities have grown further as a result of the pandemic. Again, in the event of further waves of COVID-19 or for different potential future pandemics, higher quality evidence documenting incidence and testing rates/strategies together and further analysis of different prison subgroups is necessary. More international data are required to assess transferability of results from this systematic review to other incarceration systems. Higher-quality studies from nations with comparative incarceration and healthcare systems may have more generalisable and transferable findings.
Data assessing mental health outcomes in more detail with control groups from the general population should also be prioritised. The effectiveness of any mitigating interventions should be evaluated by high-quality randomised controlled trials. We recognise that performing such studies in the context of incarceration facilities is highly complex and potentially challenging. Quality of studies could be improved with better pandemic readiness allowing prison teams to immediately liaise with researchers so that prospective verifiable data could be collected rather than relying on third party (eg, governments/prisons, unconnected with the research teams themselves) retrospective data.
Strengths and limitations
Our review is the most current assessment of COVID-19 outcomes in PEI worldwide. The study focuses on objective data relating to clinical outcomes and makes comparisons, both within incarceration facilities and with the general population, highlighting significant health inequalities. The protocol was registered on PROSPERO and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed.25 Comprehensive search terms generated evidence from both high-income and low/middle-income countries.
Incidence rates were often reported without testing rate documentation and outcomes without standardisation for age or comorbidity. Heterogenous testing strategies across countries, regions and institutions between the general population and PEI mean comparisons between data should be interpreted with caution. Crude mortality rates between the general and prison population were often reported and should also be interpreted with care. Other confounders, such as pre-existing conditions, which could impact mortality, were often not identified.
Study limitations include that only 10% of the eligibility assessment was duplicated. Studies were excluded if not published in English, potentially leading to some selection bias. Most studies (~65%) were based in the USA which may limit transferability of overall findings to other nations with different prison systems and COVID-19 burdens.
The included studies varied greatly in terms of their measured outcomes, testing strategies, data collection time, comorbidities of subjects (variably reported), vaccination coverage of subjects (often unreported) and epidemiology of COVID-19 conditions both within and between included countries. This heterogeneity was considered too great to allow for meaningful meta-analysis. The limitations of inappropriate use of random-effects model meta-analysis in systematic reviews of highly heterogeneous studies have been highlighted.91–93 Nevertheless, the lack of meta-analysis is a limitation of this study and a common issue faced by systematic reviews looking to assess impacts of the COVID-19 pandemic on small population groups in differing regions/countries, for example, long-term care facility residents and people experiencing homelessness.88 90
Conclusion
PEI had poor COVID-19 clinical outcomes such as higher incidence and rates of hospitalisation, poorer hospital outcomes, higher mortality and worsening mental health outcomes. However, the true and lasting impact of COVID-19 on PEI cannot be assessed due to research gaps, low-quality evidence and heterogeneous results. Outcomes, especially the long-term effects of COVID-19, and the effectiveness of mitigating COVID-19 interventions should be assessed, so that management of this pandemic (if there are further waves) or any potential future pandemics, is evidence-based.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank Elizabeth Gillen (Wales Centre for Evidence Based Care) for assistance in designing the searching, Dr Stephanie Perrett (Public Health Wales) and Dr Jake Hard (Medical Director for prisons healthcare) for stakeholder advice.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DBW and BS are joint first authors.
Contributors AE and BS conceived the article. DBW, BS and FB performed the literature search. BS and DBW collected data from individual studies and interpreted the data. BS and DBW wrote the first draft of the paper. DBW, DW, AE and RL revised the first and subsequent drafts. All authors contributed to interpretation of the findings and revised the manuscript for important intellectual content. All authors meet all four criteria of ICMJE recommendations for authorship. DBW is the author acting as guarantor for this paper.
Funding Authors DBW, BS and FB have not received a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. Authors DW, AE and RL are funded by the Wales COVID-19 Evidence Centre.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.