Article Text

Abstract
Objectives The majority of female immigrants who are married in Taiwan often face a variety of stresses, which may lead to physical or mental illness. Yet few studies have validated the impact of length of residency on physical and mental health using large-scale data. This study combined five nationwide databases and explored the impact of length of residency in Taiwan on the physical and mental health of female marriage immigrants.
Design This is a retrospective cohort study.
Setting Taiwan.
Participants A total of 168 202 female immigrants, who were registered in the national health insurance database from 2001 to 2017, were enrolled for analysis.
Measure The length of residency was taken as the period from their first appearance in the national health insurance database to the end of 2017. Hypertension and diabetes were chosen as indices of physical health and depression as an index of mental health. Diagnosis standards were based on the International Classification of Disease, ninth or 10th Revision.
Results The physical and mental health of the immigrants deteriorated with increasing time of residence in Taiwan. Immigrants who had resided in Taiwan for 5–10 years or ≥10 years, respectively, had a 5.8-fold (95% CI: 3.46 to 9.74) or 6.29-fold (95% CI: 4.61 to 8.59) higher adjusted risk of developing hypertension; a 3.97-fold (95% CI: 2.54 to 6.21) or 9.18-fold (95% CI: 5.48 to 15.38) higher adjusted risk of developing diabetes; and a 5.01-fold (95% CI: 3.14 to 8.01) or 12.19-fold (95% CI: 8.65 to 17.18) higher adjusted risk of developing depression than their counterparts who had lived in Taiwan for ≤5 years.
Conclusion These findings suggest the time elapsed since migration can be a factor in the deterioration of both physical and mental health among female marriage immigrants in Taiwan.
- Hypertension
- General diabetes
- Depression & mood disorders
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from Ministry of Health and Welfare, Taiwan, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study included the entire population of Taiwan in the analyses to prevent sampling and selection bias.
Through the retrospective cohort design, the causal relationships among the variables in this study become clearer.
Since length of residency correlates with age, the impact of residency duration on physical and mental illnesses observed in this 17 year longitudinal study could be influenced by the confounding factor of ageing.
A part of immigrant women may be lost to follow-up due to maladjustment or health issues, which results in underestimating of the HRs.
Background
The population of new immigrants in Taiwan comprises mostly women (90%) who come to the country through marriage and as individuals.1 This differs from the predominant pattern of family immigration that is seen in many other countries around the world.2 Knowledge concerning the physical and psychological development of marriage immigrants overcoming multiple acculturation challenges is still limited.
In general, immigrants are a strongly selected population: their average physical condition tends to be better than that of the citizens of the host country. The ‘healthy immigrant effect’ theory pertains not only to physical aspects,3 but can also be extended to the psychological aspects of the female immigrants of Taiwan.4 However, adaptation is a process that changes over time. For example, Berry5 proposed four distinct patterns of acculturation in terms of separation, integration, assimilation and marginalisation or individualism, which can change over time from one pattern to another. Ward and Geeraert6 further emphasised that cultural adaptation is not only a dynamic process but also highlighted that both acculturative stress and acculturative change occur within an ecological context. Therefore, the trajectories and outcomes of the adaptation process need to be understood through different levels of factors. Additionally, immigrants often encounter multiple and long-term stressors in their new environment. Taking a stress perspective, Cervantes and Castro7 explained how Mexican American immigrants evaluate potential sources of stress and regulate the impact of these stressors on their physical and mental health through a ‘multivariate stress-mediation-outcome model.’ Subsequently, Castro and Murray,8 based on resilience theory and research, proposed a ‘resilience-based stress-appraisal-coping model’ that conceptualises coping and cultural adjustment as processes within a long-term, time-oriented and developmental framework. The process of cultural adaptation is further defined as a resilience trajectory, which represents the path of development over time for immigrants in the host society. These perspectives suggest that a long-term observation from a process-oriented perspective is necessary when exploring immigrant health issues.
A study conducted in Central Taiwan showed that in female immigrants, with increasing time of residence in the host country, symptoms of depression increased significantly.9 A study conducted in the USA indicated that with increasing time of residence in the host country, immigrants’ depression and mental disturbance became worse than those of local Americans.10 With respect to cardiovascular health, the advantage conferred by the healthy immigrant effect appears to be short-lived.11 All these results indicate that the longer immigrants stay in the host country, the worse their physical and mental well-being becomes.12 13 However, the sample sizes were small and the studies were conducted in specific regions. This calls the representativeness of the data into question. Additionally, the paucity of studies on health issues related to immigration hinders our understanding of the full impact of acculturation.
To overcome this problem, using representative nationwide data, we explored the impact of acculturation (using time spent living in Taiwan as an index) on female immigrants’ health development. A useful health index should include both mental-health conditions, such as depression and common physical illnesses, such as hypertension and diabetes. Using the 17 year retrospective follow-up study, we sought to examine whether immigrant women who were in good health when they first arrived in Taiwan see their physical and mental health deteriorate during the years of residence.
Methods
Research design and data selection
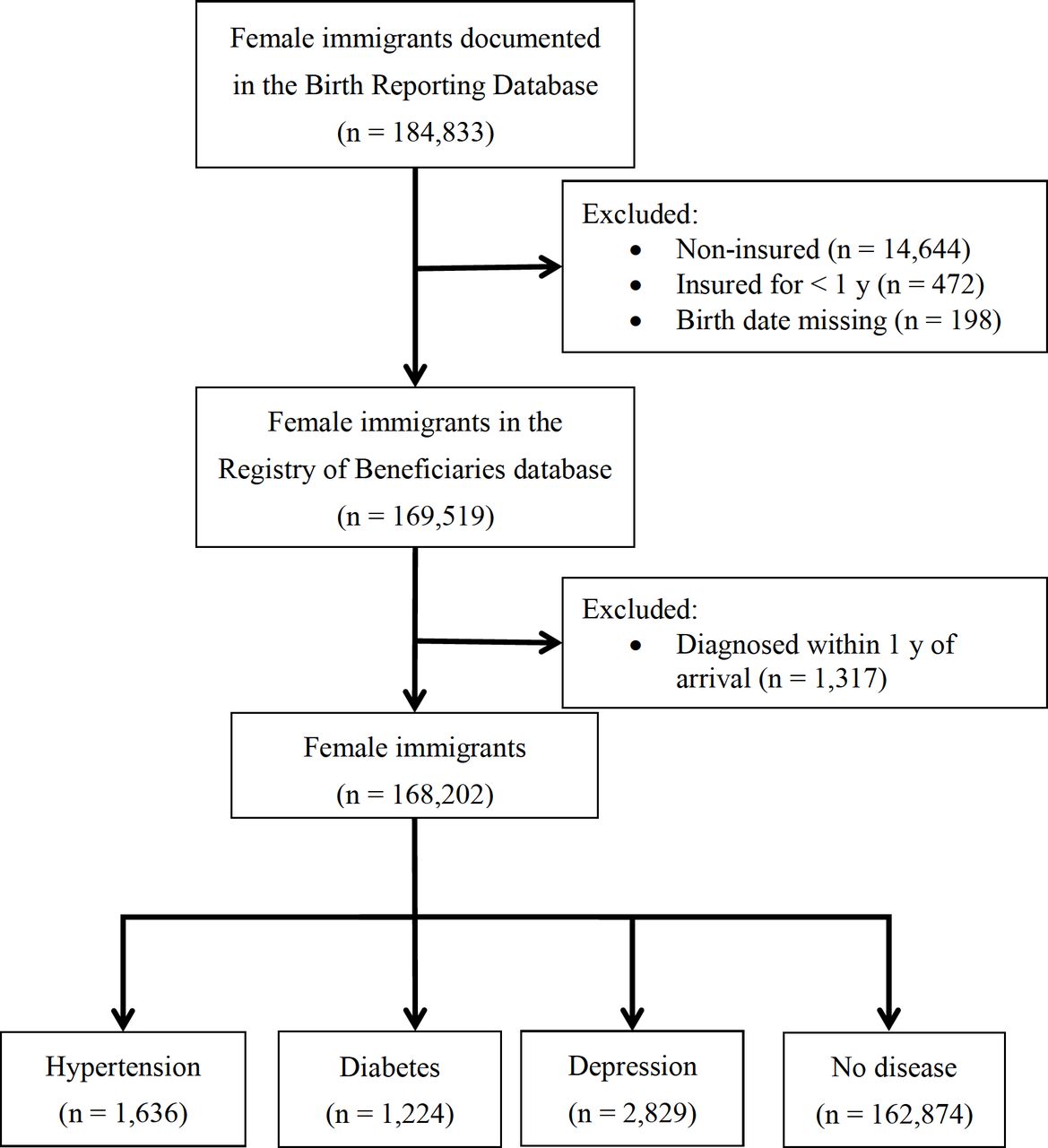
We adopted a retrospective cohort study design. Using five databases, we extracted eligible participants and their corresponding variables. First, we selected non-Taiwanese mothers documented in the ‘Birth Reporting Database’, which was maintained by the Ministry of Interior in Taiwan, from 2001 to 2016 and eliminated duplicate data for mothers who had given birth more than once. This resulted in 184 833 female immigrants. Next, we matched the mothers’ ID with the 2001–2017 data in the ‘Registry of Beneficiaries’, which was maintained by the Ministry of Health and Welfare in Taiwan, and used the first date on which each woman had appeared in the database as the starting point of her residency in Taiwan. The end of the study was the end of 2017. Immigrants without health insurance or who had held their insurance for less than 1 year, or who did not have a birth date in the database, were excluded. This process yielded 169 519 female immigrants with health insurance. Disease data for the observation period were obtained from the ‘Ambulatory Care Expenditure by Visits’ and the ‘Inpatient Expenditure by Admissions’ databases, which was maintained by the Ministry of Health and Welfare in Taiwan. We selected hypertension, diabetes and depression as the outcomes of this study. All diseases were diagnosed according to the diagnosis standard in the International Classification of Diseases, ninth or 10th Revision, and were only regarded as a confirmed diagnosis when there were at least three outpatient visits or one inpatient admission. Further, to prevent reverse causality (ie, when the woman may have already had the disease in her country of origin), we excluded all women who were diagnosed within 1 year of arriving in Taiwan. The final number of participants was 168 202 (figure 1).

The sampling process of this study.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this study.
Research variables
Dependent variable
The dependent variables of this study were the diagnoses of hypertension, diabetes and depression. We aimed to explore the impact of the process of acculturation on disease. To avoid any possible interference from hereditary or genetic disorders, we excluded diseases that are mainly caused by hereditary or genetic factors. We therefore included the following hypertension-related diseases (ICD-9 codes 402–405 and ICD-10 codes I11–I15): hypertensive heart disease, hypertensive chronic kidney disease, hypertensive heart and chronic kidney disease and secondary hypertension. We included the following diabetes diagnoses (ICD-9 code 250 and ICD-10 codes E11–E14): non-insulin-dependent diabetes mellitus, malnutrition-related diabetes mellitus, other specified diabetes mellitus and unspecified diabetes mellitus. Finally, we included the following depression diagnoses (ICD-9 codes 296.2 296.3 300.4 and ICD-10 codes F32–F34): depressive episode, recurrent depressive disorder and persistent depressive disorder.
Independent variable
As the independent variable, we used length of residency (in years) in Taiwan as an index of acculturation. This was defined as 2017 (the endpoint of the study period) minus the year that the woman was first documented in the Registry of Beneficiaries, rounded off to the nearest integer. To prevent prevalent cases, women who were diagnosed with the disease within their first year of arriving were excluded. When estimating the risk of disease, the length of residency was divided to three categories: ≤5 years, 5–10 years and ≥10 years.
Sociodemographic variables
To prevent confounding, we adjusted for sociodemographic variables using regression analysis. These variables included (1) nationality of origin; (2) age on arrival (defined as the first year of registration in the insurance database minus the year of birth, rounded off to the nearest integer; for convenience, based on analysis, this was categorised into 18–25 years, 26–30 years, 31–35 years and ≥35 years); (3) region of residence (northern, central, southern, eastern and outlying islands) and (4) socioeconomic status (obtained from the ‘Low-income and Middle-income Households’, which was maintained by the Ministry of Health and Welfare in Taiwan, database and categorised into high (upper-middle-income households) and low (lower-middle-household and low-income households)).
Statistical analysis
Data were analysed using the SAS V.9.4 software (SAS Institute, Cary, NC, USA). The observed variables were summarised using frequency, percentage, mean, SD and their distributions. We used time-dependent Cox regression analysis to estimate the risk of developing hypertension, diabetes and depression during the follow-up period. Because we used the incident cases, the first year became immortal time. We followed up our participants from the second year of arriving to the outcomes of interest or the end of study (31 December 2017). On controlling for confounding variables, we used HRs to describe the risk of developing each disease and 95% CIs to assess whether the HRs were statistically significant.
Results
Characteristics and distribution of sociodemographic variables
For the 17 year observation period, we obtained data for 168 202 female immigrants who were eligible and included in the study. In terms of nationality of origin, the majority were from either Southeast Asia (50.84%) or Mainland China, Hong Kong and Macau (46.68%) in similar proportions (table 1). Approximately two-thirds (62.66%) of the women had lived in Taiwan for more than 10 years, and the largest proportion (46.83%) arrived when they were in the youngest age category (18–25 years). More than half of them lived in Northern Taiwan (51.52%). Only 1.85% of the women lived in low-income households.
Sociodemographic characteristics of the female immigrants included in this study (n=168 202)
Incidence rate and age of onset of physical and mental illnesses
In the 17 year study period, the most common of the three diseases we were considering was depression: 2829 of the immigrants developed depression (table 2). The cumulative incidence rate was 1.68%, the average annual incidence rate was 0.11% and the mean age of onset was 33.40±5.43 years. This was followed by hypertension (1636 cases), which had a cumulative incidence rate of 0.97%, an average annual incidence rate of 0.06% and a mean age of onset of 36.07±5.85 years. Finally, 1224 of the women were diagnosed with diabetes, which had a cumulative incidence rate of 0.73%, an average annual incidence rate of 0.05% and a mean age of onset of 33.90±5.78 years.
Incidence rate and age of onset of physical and mental illnesses in female immigrants
Cumulative numbers of cases versus length of residency
Figure 2 shows that the cumulative cases of hypertension, diabetes and depression increased rapidly in the women’s first 5 years of living in Taiwan. The rate of increase in these cases gradually declined when the women had been in the country for 5–10 years. When the length of residency exceeded 10 years, the cumulative cases of all three diseases gradually plateaued. These patterns appear to reflect the predictions of the theory of acculturation.

{kind=link}
{kind=link}
Cumulative cases of hypertension, diabetes and depression among female immigrants by the length of residency.
Physical and mental disease risk in female immigrants
Controlling for nationality, age on arrival, region of residence and socioeconomic status, time-dependent Cox regression models revealed a pattern of increasing risk of physical and mental diseases with increasing length of residency in this group of female immigrants (table 3). Compared with women who had lived in Taiwan for ≤5 years, the risk of developing hypertension in those who had lived there for 5–10 years was 5.8-fold higher (95% CI: 3.46 to 9.74), and in those with ≥10 years’ residency, it was 6.29-fold higher (95% CI: 4.61 to 8.59). Similarly, the risk of developing diabetes was 3.97-fold higher in residents of 5–10 years (95% CI: 2.54 to 6.21) and 9.18-fold higher in residents of ≥10 years (95% CI: 5.48 to 15.38) than in those of ≤5 years’ residency. Finally, the risk of developing depression that was 5.01-fold higher in residents of 5–10 years (95% CI: 3.14 to 8.01) and 12.19-fold higher in residents of ≥10 years (95% CI: 8.65 to 17.18) than in those of ≤5 years’ residency. These reflect that both the physical and mental health deteriorated with the time elapsed since migration in female immigrants in Taiwan.
Changes in HRs for physical and mental illnesses with increasing duration of residency
Discussion
We used data from representative nationwide databases to explore the impact of length of residency on female immigrants’ physical and mental health to validate the negative acculturation theory, which is applicable to marriage immigrants who came to their new country as individuals. Main findings of the present study were as follows: (1) The longer the women resided in Taiwan, the higher was their risk of developing physical illness (hypertension and diabetes), and their risk of developing mental illness (depression) was even higher. This suggests that the initial healthy immigrant effect was reduced or completely abolished with increasing time of residency in Taiwan, and that the risk of developing physical and mental health problems increased with time. (2) Acculturation is not a linear process that goes from the time of arrival to that of integration or assimilation. In addition, it is a process of adaptation which can change over time that must be understood as a set of strategies deployed by immigrants to adapt to a new environment.
Although length of residency in the immigration country is often used as an index of acculturation, our findings suggest that with increasing residency time, new immigrants’ health status declines. Similar findings have been reported in previous studies.10 14–16 For example, a recent study in Central Italy16 showed that the risk of developing hypertension and type 2 diabetes in first-generation Chinese immigrants, especially women, who had lived in Italy for ≥20 years was double that of their ≤10 years counterparts (the ORs were 1.90 and 1.93, respectively). In contrast to previous studies, which only recruited participants regionally and had small sample sizes,9 we included the entire population of Taiwan in our analysis to prevent sampling and selection bias and allow for more compelling data inference. We also included both physical and mental health indices as outcomes and used the International Classification of Disease as our standard for disease diagnosis, which provides a more multimodal and objective assessment than the diagnosis standards applied in these previous studies.
The reason for the decline in the physical health of immigrants over time is generally believed to be related to the environment of the immigration country, especially changes in lifestyle and diet. This suggests that immigrants’ health status should become more consistent with that of locals with increasing residency time.12 17 18 It has been shown in the USA that the prevalence rate of hypertension in the immigrant population increases with increasing length of residency.14 Compared with local Caucasians, Southeast Asian immigrants were more likely to develop hypertension problems.19 The reason for this may be insufficient intake of fresh vegetables, consuming excessive quantities of processed food, and increasing amounts of time spent sedentary.20
Life in Taiwan is fast-paced, and Taiwanese society attaches great importance to gourmet food which often contains high levels of sugar, fat and salt. The prevalence rate of hypertension and diabetes in the general population aged over 19 years is increasing annually. A large-scale survey indicated that the prevalence rate of diabetes in males increased from 3.2% in the 1990s to 12.0% in the 2000s. In females, it increased from 5.5% to 8.0%. This change is likely due to unhealthy changes in diet and lifestyle, including the increased availability and variety of sweets and sugary drinks, increased calorie intake and long hours spent sedentary.21 Our finding that diabetes and hypertension in new immigrants in Taiwan also increased with time of residency suggests that the immigrants are adapting to the diet and lifestyle in Taiwan, thereby increasing their risk of diabetes and hypertension.
Apart from lifestyle and diet, the process of immigration and subsequent adaptation contribute to increasing risk factors for hypertension and diabetes. Recent research22 has compiled study results of migrants in Europe and North America, revealing that acculturation, psychological stress and various environmental factors contribute to the development of cardiovascular and metabolic conditions. This indicates that the experience of being an immigrant, along with associated stresses, could be significant contributing factors to diabetes and hypertension.
It is noteworthy that the risk of depression also increased significantly with increasing length of residency. This implies that negative acculturation exerts a stronger impact on mental health. A nationwide survey23 showed that the prevalence rate of depression requiring treatment in hospitals and clinics in females in Taiwan rose from 2.02% in 2007 to 2.42% in 2016, which was a 20% increase in 10 years. Our findings are consistent with this study and indicate that female immigrants encounter similar levels of stress to local Taiwanese women. Further, female immigrants are subject to stigmatisation and discrimination1 because they have come to the country as part of the system of commodified marriage.24 More importantly, a lack of emotional support in such marriages and the patriarchal culture of traditional Chinese society makes acculturation more challenging.9 The continuous challenges of adapting can result in mental health problems.
Female immigrants in Taiwan through marriage are a highly selective group with considerable physical and mental resilience.4 The ‘healthy immigrant theory’ refers to their physical and mental state on first arriving and it does not presuppose that immigrants will remain so for the rest of their lives. It is conceivable that there is a process whereby, for some, this state of health deteriorates from the very first years to reach the national average, and that changes in lifestyle habits are significantly involved.
There are some limitations to the current study, which may reduce the generalisability of the findings. First, since length of residency correlates with age, the impact of residency duration on physical and mental illnesses observed in this 17 year longitudinal study could be influenced by the confounding factor of ageing. Although age on arrival is controlled for in the Cox proportional hazards model, it is still challenging to avoid the impact of ageing on physical and mental health during long-term follow-up of participants. Second, a part of immigrant women may be lost to follow-up due to maladjustment or health issues, which results in underestimating of the HRs. Nevertheless, since this study analysed national data, the number of people lost to follow-up was relatively small, so the extent of the impact should be minimal.
In conclusion, we found that among the female marriage immigrants who account for 90% of immigrants in Taiwan, the time elapsed since migration can be a factor in the deterioration of their physical and mental health. Findings of this study suggest that providing health-promoting information and programmes during the early stages of immigration, along with continuous screening in later periods, is of significant importance for the physical and mental health of immigrant populations.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from Ministry of Health and Welfare, Taiwan, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Research Ethics Committee of the China Medical University and Hospital (approval number: CMUH108-REC1-142), and informed consent is not required as this study used existing data of the NHIRD in Taiwan which are deidentified.
Footnotes
Contributors PCL generated the concept of this research paper, wrote the research proposal, analysed the data, was involved in the presentation and interpretation process of results and discussions. YLC was involved in data analysis, participated in the presentation and interpretation process of results and discussions and reviewed the draft manuscript. HJY participated in the concept generation and presentation and interpretation of results and discussions, and reviewed and finalised the manuscript and is the corresponding author who is responsible for the overall content as the guarantor. All the authors read and approved the final manuscript.
Funding This work was partly supported by grants from the Ministry of Science and Technology, Taiwan (MOST 109-2314-B-468-001-MY2).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.