Article Text

Abstract
Objectives To understand community antibiotic practices and their drivers, comprehensively and in contextually sensitive ways, we explored the individual, community and health system-level factors influencing community antibiotic practices in rural West Bengal in India.
Design Qualitative study using focus group discussions and in-depth interviews.
Setting Two contrasting village clusters in South 24 Parganas district, West Bengal, India. Fieldwork was conducted between November 2019 and January 2020.
Participants 98 adult community members (42 men and 56 women) were selected purposively for 8 focus group discussions. In-depth interviews were conducted with 16 community key informants (7 teachers, 4 elected village representatives, 2 doctors and 3 social workers) and 14 community health workers.
Results Significant themes at the individual level included sociodemographics (age, gender, education), cognitive factors (knowledge and perceptions of modern antibiotics within non-biomedical belief systems), affective influences (emotive interpretations of appropriate medicine consumption) and economic constraints (affordability of antibiotic courses and overall costs of care). Antibiotics were viewed as essential fever remedies, akin to antipyretics, with decisions to halt mid-course influenced by non-biomedical beliefs associating prolonged use with toxicity. Themes at the community and health system levels included the health stewardship roles of village leaders and knowledge brokering by informal providers, pharmacists and public sector accredited social health activists. However, these community resources lacked sufficient knowledge to address people’s doubts and concerns. Qualified doctors were physically and socially inaccessible, creating a barrier to seeking their expertise.
Conclusions The interplay of sociodemographic, cognitive and affective factors, and economic constraints at the individual level, underscores the complexity of antibiotic usage. Additionally, community leaders and health workers emerge as crucial players, yet their knowledge gaps and lack of empowerment pose challenges in addressing public concerns. This comprehensive analysis highlights the need for targeted interventions that address both individual beliefs and community health dynamics to promote judicious antibiotic use.
- Infection control
- Public health
- QUALITATIVE RESEARCH
- Behavior
- Infectious diseases & infestations
- Health Literacy
Data availability statement
Data are available upon reasonable request. Anonymised transcripts that do not pose any risk to participants’ confidentiality can be made available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Infection control
- Public health
- QUALITATIVE RESEARCH
- Behavior
- Infectious diseases & infestations
- Health Literacy
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study employed a comprehensive multilevel framework, shedding light on the intricate interplay between community and health system factors alongside individual-level influences that shape individuals’ antibiotic practices.
The utilisation of qualitative research methods enabled a more nuanced exploration of people’s perceptions of infectious diseases, uncovering latent non-biomedical belief models, and providing insights into how antibiotics are understood and used within this cultural context.
Another study strength is the special focus on the information needs of specific vulnerable groups, namely pregnant women, mothers with young children, and the elderly, elucidated through focus group discussions.
A key limitation is the study’s exclusive concentration on two village clusters (Gram Panchayats) within a single district in West Bengal, which, while offering depth, introduces limitations concerning the broader representativeness and generalisability of the findings to diverse contexts.
Introduction
Misuse of antibiotics in human health is a major contributor to the development of antimicrobial resistance (AMR),1 a phenomenon that occurs when diseases-causing pathogens no longer respond to antimicrobials. More than 5 million deaths were linked to drug-resistant infections in 2019, a substantial proportion of which were in sub-Saharan Africa and South Asia.2 India, a South Asian country where this study is located, is the highest consumer of antibiotics in the world by total volume (6.3 million defined daily doses)3 and has among the highest levels of drug resistance.4 National data show that the resistance of priority pathogens to broad-spectrum antibiotics has been increasing at 5%–10% annually5; in 2021, only 43% of pneumonia cases could be treated with first-line antibiotics.6
In most low/middle-income country (LMICs), antibiotics are easily available without a prescription.7 8 For example, between 50% and 100% of antibiotics are sold without a prescription in Asian countries like Vietnam, Bangladesh and India, and African countries like Ghana and Mozambique.9–13 People may self-medicate with antibiotics they buy over the counter, or they may be treated by providers with limited or no formal medical training. Self-medication is common across South Asia, including India, with a mean prevalence of 42.6%.14 In a study in rural Uttar Pradesh in India, antibiotics were the third most purchased drugs for self-medication.12 There is also strong evidence that a very substantial proportion of healthcare and antibiotics in several LMICs are sought from informal sources, such as village doctors in India and Bangladesh, drug shops in Africa and unlicensed pharmacies in South east Asia.9 15–18 There have been few systematic attempts to integrate these significant providers of antibiotics into formal health systems19 or to establish practical alternatives for people to seek treatment for infections.
Inappropriate antibiotic use includes taking a partial course or using them for viral infections and other conditions where antibiotics are not needed. In rural Ghana, for example, a study found that tetracycline and metronidazole were poured into ‘akpeteshie’ (local gin) to treat hernia and perceived stomach ulcers.10 We found in our earlier work in West Bengal that people purchased very short courses of antibiotics from informal providers (IPs), stopped taking them when they felt better and shared leftover antibiotics with friends and family.15 Similar practices have been found in other parts of India, including rural Haryana and Uttar Pradesh.12 13 The factors influencing these practices are not well understood, although there is some evidence that lack of knowledge about antibiotics,11 13 especially among rural communities,20 may be important.
Studies in Africa and Asia suggest that people have limited knowledge, from a western biomedical perspective, about antibiotics and antibiotic resistance. While some may recognise a few antibiotics by their colour or name, there is a lack understanding of how they work.10 11 21 Antibiotic users may perceive resistance as a kind of treatment failure resulting from non-compliance, ineffective medication, or a physical inability of the human body to respond to treatment.11 Concerns about affordability also influence people to seek quick relief in the shortest time, at minimum cost.13 15 22 23
The way that individuals interact with their antibiotics, and the pressures that influence these behaviours, need to be better understood and addressed in contextually sensitive ways in order to achieve the goal of optimising antibiotic use. Available studies of antibiotic use have largely focused on individual-level factors, providing much less information on the role of community and society-level factors influencing behaviour.24 25 There is also a paucity of comprehensive studies in the Indian community setting. We designed this study to explore the individual, community and wider health system level factors influencing rural communities’ antibiotic practices in West Bengal, India.
Methods
Conceptual framework
We adapted the socioecological model of social and behaviour change communication,25 which is also emphasised in water, sanitation and hygiene behaviour change24 and reflected in studies of healthcare seeking.26 This model views social and behaviour change as a product of multiple, overlapping levels of influence between the individual (a person’s knowledge, motivation and gender), the interpersonal (partners, family and peers), community (services, products, leaders and providers) and the environment (policies and health system). This model encompasses several theories of behaviour change ranging from individual-level theories (eg, health belief model and reasoned action) to social learning and diffusion theories, community organisation, social norms and gender theories and social movement and network theories. The model is based on the following principles of human behaviour: that people interpret information based on their own context; that culture, norms and networks influence individual behaviours; that people cannot always control the issues which create their behaviour and people’s decisions about health and well-being compete with other priorities. Adapting this to our study, we analysed antibiotic behaviours as the result of an interplay of influences at the individual, community and health system levels.
Study design
This was a qualitative study comprising focus group discussions (FGDs) and in-depth interviews (IDIs) to explore rural community members’ antibiotic practices. FGDs were followed by IDIs with key informants including community leaders and local healthcare providers. Fieldwork was conducted between November 2019 and January 2020. This study was part of a larger formative study27 that aimed to inform an antibiotic stewardship intervention in a rural community setting in India.
Study setting
West Bengal, India’s fourth most populous state with 91 million inhabitants,28 is a medium development state with a per capita net state domestic product of US$1333, slightly lower than the average for India.29 A District Level Household and Facility Survey30 conducted prior to this present study in 2018–2019 revealed a high burden of infectious diseases in the state: 16% of the population reported acute illnesses including fever (31%), acute respiratory infections (20%), diarrhoea/dysentery (12%) and malaria (7%). Previous studies including our own15 19 31 have revealed inappropriate antibiotic dispensing (unnecessary and subtherapeutic) by local healthcare providers, including those who are informally trained. As community expectations and perceptions have been found to be one of the key drivers of provider practices in the state,15 32 we considered it appropriate to conduct a more focused community-based study in our original research sites in West Bengal.
This study was conducted in South 24 Parganas district of West Bengal, which was one of our previous study sites. This is West Bengal’s largest district by area, and the second largest by population.33 Seventy-four per cent of the district’s nine million population is rural, more than the average for West Bengal (68%).33 We purposively selected two contrasting village clusters in the district (known as gram-panchayats in local administrative parlance). The first cluster (or site 1) (population 7527, Census 2011) was closer to the state capital, Kolkata (60 km; <2 hours by road) and had three periurban areas within 10–20 km with several pharmacies and private doctors’ clinics. There was one block level government Primary Health Centre (PHC) 10 km away where a medical doctor was available, and a smaller less well-equipped PHC closer to the site. The second cluster (site 2) (population 3620 as per census 2011) was more remote, 95 km (>4 hours by road and ferry) from Kolkata. There was only one government PHC here and one charitable health facility with two doctors. A few private doctors were reported to visit on weekly market days. Both sites, however, had several IPs practising in the villages: 19 in site 1 and 21 in site 2 (based on our earlier provider mapping done here15). Each site also had three government subhealth centres (base tier in the hierarchy of government health facilities, staffed with auxiliary nurse midwives (ANMs)). We selected our participants from the catchment areas of these three subcentres.
Study participants
Four FGDs were conducted in each site (eight in total), which included one each with adult males and adult females, one with a mixed gender group and one with pregnant women and nursing mothers. For the first three groups, we selected participants of varying age groups, from early 20s to late 50s, to elicit variations in behaviours and drivers. The subgroup of pregnant women and nursing mothers was included as we wanted to understand antibiotic practices during maternity and with young children. These women were recruited through an antenatal care clinic at one subcentre in each site. We kept three groups homogenous (adult male/female and pregnant women/nursing mothers) in terms of gender so that respondents were comfortable and forthcoming in discussing their views within such groups. One FGD group in each site was mixed, to stimulate a greater variety of responses.
IDIs were conducted with key village informants including schoolteachers, local doctors and nurses, elected representatives, and civil society, and also with local community health workers (CHWs) from the government healthcare system. These included accredited social health activists (ASHAs) and ANMs. ASHAs and ANMs provide preventive and promotive maternal and child health services. These IDIs were supplemented with previously collected data from IPs and private doctors obtained during a previous study in the same site.15
Our study prioritised conceptual depth and diversity over exhaustive coverage.34 This meant that the numbers of FGDs and IDIs were determined by obtaining sufficiently developed concepts and rich data rather than data saturation. Additionally, given the small size of our study sites, we aimed to prevent study fatigue among the local population while capturing diverse perspectives. This was achieved by strategically distributing data collection across three catchment areas in each cluster and maintaining a feasible number of FGDs and IDIs possible within our study resources.
Study instruments and data collection
We used semistructured topic guides for the FGDs and IDIs. The FGD guide included questions on perceptions of illnesses and explanatory models, treatment choices, antibiotic knowledge and practices, sources of information and influence of families, peers and others in the community. The IDI guides in turn investigated the roles, knowledge and perceptions of key informants, local health seeking patterns, peoples’ access to and use of existing forums for health-related awareness and behaviour change communication. We translated (into Bengali) and pretested the FGD and IDI guides in a non-study area with a comparable demographic and socioeconomic profile and made minor amendments to the guides. The FGD and IDI guides are attached as online supplemental files S1–S3.
Supplemental material
Supplemental material
Supplemental material
The data collection team comprised two researchers trained in qualitative research, guided by two senior qualitative researchers. The FGDs lasted between 45 and 70 min and were conducted in private spaces like a domestic courtyard, with the host’s permission. We took care to ensure that no health service providers or holders of public office were present so that people could speak freely. The IDIs lasted from 45 to 60 min and were conducted in private spaces in participants’ workplaces. Both FGDs and IDIs were audio recorded with the participants’ consent and supplemented with field notes. The recordings were anonymised and transcribed verbatim by the interviewing researchers who were bilingual. One senior researcher proficient in Bengali, the local language, checked the transcripts against the audio recordings for accuracy and completeness.
Patient and public involvement
The team was initially introduced to the rural communities by our collaborating non-governmental organisation with local presence and acceptance. Communities in our study sites were involved from early on, first through informal conversations to build our contextual understanding and develop our study tools, and then to participate in the piloting and implementation of the FGDs. Some of the key informants (IDI respondents) were selected with the help of local communities, while a few, like the village leaders helped introduce us to the village communities.
Data analysis
We started the analysis with data familiarisation, a process that involved reading the transcripts and noting down ideas. The coding was subsequently done using QRS International NVivo (V.12). The research team developed a coding tree based on the themes emerging from the data (the NVivo coding tree is attached as online supplemental file S4). Two transcripts in each category were coded by a pair of researchers to enhance inter-rater reliability and to identify any new additional codes that emerged. Discrepancies were resolved by discussion until a consensus was reached. Key themes (common and divergent ones), concepts and emergent categories were analysed using the thematic framework approach. Quotes used in this paper are anonymised and only the participants’ categories are mentioned.
Supplemental material
Study trustworthiness
We strengthened the trustworthiness35 of this study in the following ways: first by incorporating multiple data sources (FGDs and IDIs) and diverse participant perspectives, triangulating these and periodically discussing our ongoing findings with the wider project team and a few local stakeholders to increase the credibility of the findings; second, by documenting all study methods for data collection and analysis (including log sheets, topic guides, transcripts and coding trees) to enhance study dependability and transferability; and third by prolonged engagement with the data, systematic data analysis, and reflecting on (and mediating) our own biomedical lenses while exploring local perceptions and knowledge, to enhance study confirmability. Being aware of our possible biases, we made a conscious effort to remain open minded and receptive to the diversity of knowledge among our participants. Even though we were outsiders to the communities, our field research team including one of the lead investigators was fluent in Bangla, the local language. This helped us establish rapport with the study communities through informal as well as formal discussions. Researchers of the same sex as the participants conducted the FGDs and IDIs to ensure participants’ comfort and ease of responding. Finally, regular discussions within our research team provided a platform for ongoing reflection and enquiry, ensuring trustworthiness in the research process.
Results
Overview of antibiotic practices in the study communities
We interviewed 16 community leaders (7 teachers, 4 elected village representatives, 2 doctors and 3 social workers), 14 CHWs (6 ASHAs, 6 ANMs, 2 nurses) and conducted eight FGDs with 98 community members (42 men and 56 women). Most of the FGD participants were illiterate or educated only to the primary level. Most were from small farm owing households or agricultural labourers.
A majority of FGD participants in both study sites said they bought antibiotics from IPs and medicine shops much more than from CHWs, government facilities and private doctors. The bigger PHCs were a long walk away and it was often necessary to wait a considerable time to see a doctor, with adverse implications for daily wage labourers. There was also the risk of the doctor not being available at the facility. Among the nearby CHWs, ASHAs provided paracetamol and iron tablets for pregnant women, but were not permitted to dispense antibiotics. ANMs provided some antibiotics, including amoxicillin and cotrimoxazole, but these were not always in stock. It was IPs, medical shops and pharmacies on the other hand, who provided a wider range of antibiotics at all times, with less time wasted in travel and waiting. This made them the preferred option for healthcare.
People want to recover quickly; they cannot afford to lose even one days’ wage. If we go to a “Local Doctor”, (IPs) we are treated in a short time but in the hospital (PHC), I will waste a full day. (Adult men group_ GB_08).
Courses of treatment varied between 2–3 and 10 days, depending on patients’ ability to pay and providers’ judgement. Even then, course compliance was poor:
For cough and cold, doctors (includes formal and informal) prescribe antibiotics for 3 to 5 days—to be taken every 12 hours. But most people, especially women, stop after two days if they recover. (ANM_GB_03).
People also reported extensive self-medication with leftover medicines:
Once people knew that a medicine works for a certain illness, they also stock and use that for subsequent recurring illnesses. (Panchayat Member_NP_02).
The FGDs and IDIs revealed an interplay between a range of individual, community and health system level factors influencing knowledge and perceptions of antibiotics, and different aspects of their usage in this rural community setting (see figure 1).

Multilevel factors influencing antibiotic practices in a rural community setting.
Individual-level factors
Several individual-level factors including sociodemographic, cognitive, affective and economic, influenced patterns of antibiotic use which we have described thematically as follows:
Theme 1: sociodemographic factors
Age
Women’s responses in the FGDs suggested that mothers were conscious about the medicines they gave their children and there was greater compliance to a course of treatment for children than for adults. This was also corroborated by many CHWs.
In the case of babies, all of us follow the instructions but when it comes to us, we sometimes miss the follow-up. In the case of babies, if we are asked to give the child the full dose, then we do (Young mothers’group_NP_01).
This caution extended to self-medication. Some young mothers said that though they might give children their own choice of medicine for a minor cough, they would consult a doctor (formal or informal) before giving an antibiotic for fever or a perceived infection. For adults, they could buy antibiotics from a medical shop without consulting any health providers.
The age factor also affected the very elderly who faced mobility challenges and needed someone to bring their medicines from shops or providers.
Gender
Many community leaders and CHWs felt that women were an important influence on decision-making related to care-seeking and medicines. This was due to their role as caregivers and their availability while men were away at work.
Male group members suggested that any awareness campaign about health and medicines, especially for children, should begin with women. However, women were less mobile and therefore less able to access information, and medicines. Most men said that they could easily travel to medicine shops, even those at a distance, but women with young children and the elderly could only access nearby providers like ASHAs (who made home visits) or IPs. ASHAs were a major source of information for young mothers but this was mostly about maternal and child health and personal hygiene. Elderly women also complained that there was no one for them to speak to about their problems such as pain in the limbs and teeth.
Education
While some saw education as important in making better informed decisions about antibiotics, our discussions found that it could also exert a negative influence in that some better educated patients could influence IPs to dispense medicines of their choice. One schoolteacher, for example, said that he did not always complete antibiotic courses.
Theme 2: cognitive systems
Knowledge and perceptions of illnesses, remedies and antibiotics
The FGDs revealed the influence of cognitive systems on individuals’ interactions with biomedical antibiotics within a cultural context of non-biomedical belief systems. People had mixed knowledge and perceptions about the causes of illness. Many FGD participants attributed illnesses to consuming ‘hot’ and ‘cold’ foods, changes in the weather, exposure to cold temperature, hard physical labour (in the fields) and so on, and not necessarily to infections. While the awareness of the role of pathogens was limited, there was an understanding of other factors which might influence exposure to pathogens.
If my son plays in the water, he will catch a cold. If he has a wet chest and I overlook it in the morning, he will definitely catch cold by afternoon. (Adult women group_GB_01)
These belief systems were likely rooted in non-biomedical systems of medicine practiced in India, like Ayurveda, that connects human physiological functions with five elements of nature (earth, water, air, fire and space). However, some people were also aware that environmental contamination with pesticides and other poisons like arsenic affected health, as did bathing in stagnant pond water. In some FGDs, people spoke about vector-borne and water-borne diseases like dengue, malaria and stomach infections. People related these diseases to mosquitoes and flies without having a clear idea about invisible ‘germs’.
We tell our children, when you visit the bathroom, you must wash your hands with soap. You have to keep your hands clean while eating. If you have nails then keep them clean. otherwise, they will get germs which can go into your stomach. We tell them that if the germ gets into your stomach, then snake will bite in the stomach… (Adult men group_GB_03)
These narratives suggested a coexistence of biomedical concepts regarding disease causality and transmission, alongside traditional and non-biomedical belief systems. This integrated cognition extended to the understanding of and interactions with antibiotics as well.
Some FGD participants had heard of antibiotics and were able to recall a few by name like norflox, amoxicillin 500, DS cotrimoxazole and opox (a combination of cefpodoxime and clavulanic acid) and occasionally by just their strength—500 or 625. However, among those that had heard of antibiotics, many thought they were like other antipyretic medicines like ‘Calpol’ (paracetamol) for fever and acted on all infectious diseases. They viewed antibiotics as a necessary treatment for syndromes like cold and cough accompanied by fever, and wounds and small injuries, without knowing how antibiotics worked on these conditions.
Just as you need curry to eat rice, you need antibiotics along with [other general] medicines for fever and cough. (Adult women group_ GB_03)
People’s relationship with antibiotics was one of faith mixed with fear, with many believing that consuming too much of an allopathic medicine, including antibiotics, could be harmful for health. This perception seems to underlie the prevalence of incomplete courses.
I worry about something worse happening. What if I consume the rest of the medicine and some bad things happens. (Adult men group_NP_05)
Medicines are given for 5 days and if I am feeling better after 2 days, why would I take all the medicines? (Adult Women group_NP_02)
However, a group of young mothers was aware of the risks of not completing a full course of antibiotics, possibly relayed by the ASHAs or ANMs.
If we stop an antibiotic mid-course, the illness will return. (Young mothers’ group_GB_02)
Theme 3: affective influences on decision-making
Emotive and instinctive interpretations of what is ‘right’
Both FGDs and IDIs revealed that invariably, emotive factors interplayed with knowledge and cognition to influence behaviour. People stopped taking antibiotics (and other medicines too) when they started to ‘feel’ better. In the absence of any formal and clear sources of information about antibiotics, people did what they ‘felt’ was right and also what they saw and heard from trusted local health providers and friends and relatives with whom they had close personal relationships. People valued kinship ties and their sense of belonging in their communities. Self-esteem and personal motivation were linked to being an accepted member of their community and this, too, shaped choices about health. Village leaders in both study sites shared examples of how they used a carrot and stick approach—like shaming people for outdoor defaecation, and warning them with loss of entitlement for refusing vaccination, along with some motivation—to encourage behaviour change for complex behaviours like toilet use and vaccinations:
Earlier people were hesitant to take the polio vaccine, despite our consistent promotion of its advantages. So, we began warning them that if they do not take polio vaccine then government will have to restrict their entitlement on housing etc. Now everyone takes the vaccine. (Panchayat members_NP_ 04)
Theme 4: economic constraints
Individual and household economics strongly influenced healthcare seeking, as well as medicine dosage and compliance. In both study sites, the cost of healthcare was an important consideration in deciding which provider to consult. The total cost of an IP (inclusive of medicines) was much less than just the consultation fee, of a qualified private doctor:
Suppose somebody has headache, body-ache, fever or children suffering from cough and cold, people go to quack doctors (IP,) which costs approximately Rs.100-200, but in case of treatment with reputed MBBS doctor, it will be Rs 200-250 just for the consultation fee. So, the people are depending on quack doctors. (Panchayat members_NP_ 04)
The cost of transportation to a proper healthcare facility, and the opportunity cost of travelling (the loss of a day’s wages) was another major barrier to accessing proper care.
Affordability also influenced the doses that people purchased. IDIs and FGDs revealed that many people, especially daily wage earners, did not have enough money for full treatment, whether for a long-term chronic condition or for a course of antibiotics. People generally bought medicines for an acute illness for 2–3 days or even less depending on cash availability on hand. They stopped the medicines if they felt better, or went back to the provider to continue for another couple of days, or changed the medicines if they felt no improvement as there was a fear of wasting money on unused medicines.
Suppose a medicine is prescribed for 3 months and after 10 days if I feel fit then I stop it. If the cost of the full course is Rs 1500 and I stop after a month Rs 800 will go waste. (Adult men group_ NP _04)
Community-level factors
Key themes at this level included the influence of peers, the dominant role of health providers and the important role of community leadership.
Theme 1: influence of peers
Neighbours, friends and relatives influenced decisions about care-seeking and medicine use in multiple ways. Several FGDs revealed that people gave and sought advice about where to seek care for which illness:
Yes, we talk to each other. At the tea shop one person talked about his daughter’s illness, and, another one said why did you not go to PG [a tertiary hospital and medical college] yesterday. This is the way in which people choose where to go for care, after talking to 2-3 people… doctors’ reputations and people’s earlier experience and discussion—that’s how they decide. (Mixed Adult group_NP_05).
A few FGDs revealed that besides sharing their views and opinions about health providers, people also shared medicines with neighbours and relatives.
Suppose I had a problem and doctor gave me a medicine. In the middle of the course I felt fit and stopped the medicine. After 2 months if someone of my family or neighbour’s family has similar symptoms, I give him the leftover medicine and he takes it. This thing happens and it is very bad because who can confirm that his fever and my fever have the same reason. It may cause some side-effects. (Adult men_NP _04)
It was also common for neighbours and family members to buy medicines for each other, for example, for a husband to buy a medicine for his wife based on his understanding of her illness:
When my mother has a problem, father buys Saridon and gives it to her and if my mother has thyroid, an antibiotic may be problematic. My father doesn’t know that. He goes to the doctor’s [ IP’s] chamber and brings some antibiotic for her. (Adult men group_NP _04)
These actions were motivated by feelings of kinship and caring, and even when people were vaguely aware that sharing some medicines was inappropriate, they were driven by a desire to help each other reduce financial burdens.
Theme 2: role of local healthcare providers
While family and peers provided general advice and help, local healthcare providers were the most significant sources of knowledge and advice about health, medicines and antibiotics. Chief among these were the ASHAs and IPs. Our FGD narratives revealed the special bonds that people had with these providers and the trust and faith invested in them. This is because both were local and easily accessible.
ASHAs were residents of the villages where they worked. They went from house-to-house meeting pregnant women and young mothers and advised them on health and nutrition, immunisation, institutional deliveries, sanitation and hygiene. They dispensed iron supplements and paracetamol for fevers. In several FGDs, people recalled their advice and referrals and also tried to follow these:
They ask after people suffering from a cough for more than 2 weeks, and ask them to go to the PHC [Primary Health Centre] for a cough test. They also give us pamphlets on menstrual hygiene, pregnancy, lactation, dengue etc. (Young mothers’ group_GB_02).
They advise us to refrain from keeping stagnant water around the house, to use mosquito nets while sleeping and to keep the environment clean. (Adult men group_NP _03)
ASHAs however did not supply antibiotics nor provide much information about antibiotics, but they helped people understand medicine use. In several FGDs, women said they asked ASHAs to explain how to follow government doctors’ instructions for taking medicines, including antibiotics. They were perceived as extremely well-trusted knowledge sources, and people saw them as potentially good counsellors about antibiotics.
By far, the most important source of both access and information about antibiotics was IPs followed by pharmacists (where these were available). IPs in both sites stocked and dispensed a variety of medicines including antibiotics31 and some also owned medical shops. The boundary between IPs and pharmacies could be blurred, especially in the more rural areas. People called them ‘doctors’, blurring the boundaries between IPs and qualified doctors. Even when they were called ‘quack doctors’, it was always with a sense of familiarity and respect. Most FGD narratives indicated that people’s understanding of antibiotics was based on what they heard from IPs.
The doctor (IP) says I do not know what this disease is but it cannot be cured by ordinary medicine. It needs antibiotics (Adult women group_GB _01)
Although IPs were said to dispense short courses according to a patient’s ability to pay, they were also reported to counsel patients about the importance of completing antibiotic courses and the risk of antibiotic resistance.
It is important to finish the course of the medicine… if we don’t finish the course then the disease will return again…
Interviewer: Who told you that? That you have to finish the dose?
Doctors (referring to local IPs) tell us that it’s important to finish the course of medicine. (Adult women_GB _03)
Medical shops/pharmacies were also influential as they helped people understand dosages for different medicines:
The shopkeeper dispenses the medicine and also explains when and how to take it. He also writes it on the envelope. (Local teacher_NP_03).
Theme 3: role of community leaders
Village council representatives, village heads and schoolteachers were involved in keeping their communities disease free and healthy. Village leaders, in particular, appeared to have close links with local administration officials and with village CHWs. They were active in several health-related activities such as monitoring the weight of children and the number of institutional deliveries per month. Both the village council and schoolteachers had considerable influence on the community’s sanitation and hygiene behaviours, which could in turn reduce infections and the need for antibiotics.
The village council conducted campaigns for infection prevention which could reduce the need for antibiotics, such as against avoiding pond (stagnant) water for drinking, increasing vaccine acceptance and increasing the use of toilets. They did so through affective strategies such as naming and shaming those who did not comply:
…Whenever they [appointed toilet supervisors] see anybody going to the field or other open area for defecation they immediately whistle. Also tell him (the violator) ‘if you go outside for defecation, we will take your picture and disclose to all.’ This is the story of 1 year ago, now people are not going outside for defecation….we tried continuously so it became successful. (Panchayat members_ GB_03)
The knowledge of antibiotics of village leaders was, however, not much better than their communities. Since antibiotic misuse was not on the agenda of any government schemes, nothing had been done by village councils on raising awareness about antibiotics.
Health system-level factors
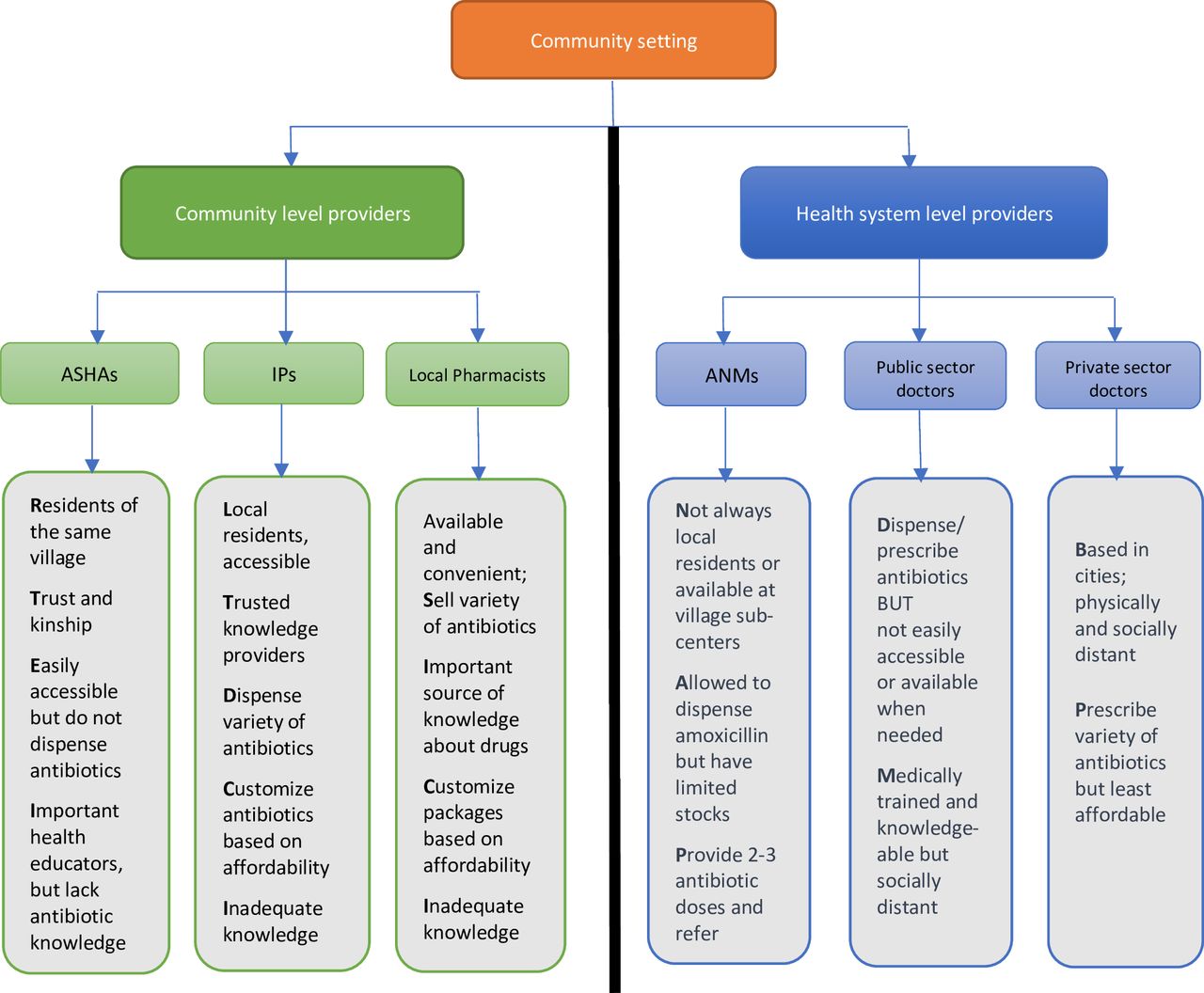
Key themes at this level included the location and availability of health providers, the critical role of access and trust building and ability to access quality medicines (figure 2).

{kind=link}
{kind=link}
Community versus the health system: a divide based on trust, accessibility and availability of providers. ASHAs: accredited social health activists are link workers between rural communities and the public health system; ANMs: auxiliary nurse midwife in the public sector; IPs: informally trained village medical practitioners. In-charge of rural subhealth centres.
Theme 1: location, accessibility and availability of providers
All the FGDs suggested that the physical proximity and convenient opening times of IPs made them the first choice for care and medicines, especially for illnesses perceived to be minor. Among formal providers, ASHAs, who were from the same village, were a primary source of advice and some non-prescription medicines like paracetamol. They were also easily accessible over the phone.
The nearest public facility with a qualified doctor was the PHC. Site 1 had a small PHC within 5 km and a larger one about 10 km away. Site 2 had only one PHC, which was quite far away and could not be accessed on foot. There was low attendance at PHCs: “Across the whole XX area (Site 1), I can guarantee that not even 30% patients visit the PHC in a whole month” (Adult men Group_ NP_04)”. This could be because PHCs were open for limited hours, were poorly equipped and the doctor might not be available.
Most often the doctor does not come, even a bandage is not available for first aid. A quack doctor has more resources for treatment than the doctor of the XX hospital (a small PHC). (Adult men group _NP_ 04)
Subcentres managed by ANMS were often closer to the villages than PHCs. But these only provided immunisation and weight monitoring for children and pregnant women, and some family planning advice. When people fell ill, they had to seek care elsewhere.
Government district hospitals, secondary-level facilities, were mostly used on referral by IPs, ASHAs or ANMs. These were even further than PHCs and had long waiting times. For site 2, the nearest district hospital was in Kolkata,100 km away. So, most residents relied on IPs for healthcare at first contact and in emergencies:
We survive because of the quack doctors (IPs). Without them, we’d be dead.(Local teacher_GB_05)
Theme 2: social access and trust
Several FGD participants said that government doctors did not explain enough about the medicines including information about dosage, duration and how to consume the medicines. They attributed this to the pressures on the system.
In the hospital, there is no time… there are so many patients. They do not listen to us properly… They just make a prescription and call the next patient… (Adult Men group_GB_05).
There was also a social distance between doctors and patients. In the FGDs, women said they were often afraid to ask questions or seek clarifications from the doctors due to their tough attitude and demeanour. Even if they mustered enough courage to ask about dosage and duration, it was not easy to discuss their other concerns about medicines:
We can ask the doctor about the dosage or course of a medicine. But can I ask about what will happen if I do not take the medicine or how it will work? He will shoo me off, and say ‘What is the use of you knowing so much? Many doctors are like this.
There is a doctor who looks very tough. If you go to him you will be afraid to say anything. (Young mother’s group _NP _01)
IPs were more socially accessible than qualified doctors (public or private) and willing to explain to people what medicines they were giving and why. IPs also followed other strategies to help their semiliterate patients comply with medicine dosages:
“They (the IPs) make us a series of envelopes. They write on it when to take it, for example after lunch—and also how many”. They make separate envelopes for each dose. Even an illiterate person can identify these…this one in the morning, this at night and so on (Adult men group _GB_05)
Theme 3: access and perceived quality of medicines
We heard repeatedly in the FGDs and IDIs that IPs provided easy access to a variety of antibiotics, customised to patients’ needs, affordability, convenience and demand for speedy cures, and this made them the preferred providers for common illnesses. Local pharmacies were also well stocked and all types of antibiotics were always available and sold easily without a prescription. Here too, dosages were tailored to the patient’s affordability:
The shopkeeper (pharmacist) first cut a strip of medicine and said the cost was 24 rupees. The customer replied that this was too high. He said he could only pay 20 rupees. The shopkeeper then reduced two tablets from the course. (Civil Society member_GB_08).
Some pharmacies and IPs even offered an added attraction: they accepted the return of unused medicines and provided refunds.
ANMs dispensed some antibiotics, such as amoxicillin, cotrimoxazole, metrogyl, along with paracetamol for fevers and ORS, zinc and calcium tablets, but they usually had very limited stocks and experienced frequent stockouts. Another limitation was that they provided adult patients only a few tablets to start the course and then referred them to the PHC or hospital for the rest.
In case of children, we give them full dose. We give them for 5 days…if they need 20 tablets we give, according to their age and requirement, provided we have enough supply. People of other age groups, we give them medicines for two or three days, and then we ask them to go to hospital. We tell them they will get same medicines at the hospital, we ask them to take the medicine packet to the doctor, to show what medicine is given to them and to tell the doctor that we were given only few tablets. (ANM_NP _02).
Some FGD and IDI respondents perceived that the medicines purchased from IPs or pharmacies were of superior quality compared with medicines dispensed free at government facilities. People tended to equate medicines that provided quick relief, with better quality of drugs, but it is possible that some medicines at government facilities were not of standard quality.
The PHC doctors typically give light doses. Your illness will take two weeks to go away. But the ones provided by the IP or the private doctor can provide immediate relief within half an hour. People are invested in this fix, not so much in the specifics of the medicine dispensed. (Panchayat member_NP_04).
Platforms and channels for communication about antibiotics
Both FGDs and IDIs indicated that there were no ongoing awareness campaigns by state or non-state actors about antibiotics or AMR. We asked respondents about their preferred platforms for receiving this information. The local health providers, especially ASHAs and IPs, emerged as the first choice as people believed that training these providers would ensure that they gave the right information to their patients in a sustainable way:
People don't know what is good or what is harmful. So at first level, you need to make the doctors (IPs) aware. First train the doctor and after that the common people…then let’s see what happens. (Panchayat member _GB_ 03)
You have to go first to the quack doctors…they are reliable and trusted and everyone will listen to them. (Adult men group_NP_ 04)
ASHAs had the added advantage of making home visits and this was seen as hugely advantageous for women busy with babies and children and household responsibilities, and also for the elderly with mobility issues.
Many FGD participants also emphasised the importance of peer-to-peer networks including their wide reach and increased likelihood of acceptance.
Consider this programme you are doing today; 20 of us are listening—each of us can now inform 10 others…this is the way to spread the news properly… (Adult women group_ GB _03)
If this information was delivered through respectable sources like schools, it would further increase the impact:
…Calling them (parents) in to the school will increase the gravity of the situation… they will give more importance to it… they will accept it better…they will understand the importance and go back to the house repeat it … (Adult men group_GB_ 05)
Some participants, the elderly in particular, liked the idea of receiving information through television, as they had time to watch TV, while younger participants recommended the use of smart phones to deliver quick, easy and even personalised messages.
For 70% people smart phone is available in each family. I have it. The whole world is in my fist. You can give awareness of antibiotic into it…! (Adult men group_NP_04)
With respect to the content of such information, several FGD participants said they would like to know more about the medicines they were receiving from doctors, whether antibiotics or something else, whether they should be consuming these at all, and what might happen if they did not. They also wanted to know about prevention and alternatives to antibiotics, including infection prevention and nutritious diets.
Discussion
Our study shows the complex and critical interplay of individual, community and health system-level influences on how people in rural settings use antibiotics and other ‘western’ medicines. The framework (figure 1) describing these influences emphasises that structural challenges at the health system level are as significant drivers of suboptimal antibiotic use as individual-level knowledge, perceptions and economic constraints. Community-level health providers—IPs and ASHAs—were the most reliable, trusted and accessible sources of information in this setting, but were paradoxically the least well equipped or empowered to address people’s doubts and concerns about antibiotics. IPs, in addition, operated on the fringes of the formal health system even while providing services central to antibiotic users.
Many of our study findings resonate with those reported from other parts of India as well as from other LMICs, where a substantial proportion of healthcare and antibiotics are sought from informal sources, like village doctors, drug shops and unlicensed pharmacies9 15–18 22 and used in ad-hoc ways through self-medication, non-standardised dosing and inadequate course compliance.11 13 15 18 22 Lack of accessibility and affordability of formal health services and cost of full courses of medicines are profound health system-level barriers for optimal use of antibiotics13 15 21 in community settings in many LMICs.
At the individual level, suboptimal antibiotic practices have frequently been attributed to prevailing perceptions regarding antibiotic usage,10 11 15 20 a phenomenon congruent with our findings. Our study revealed a common perception of antibiotics as fever remedies that can be initiated and terminated at will. Similar trends have been observed in studies conducted in Nepal20 and Mozambique11 reflecting a misconception about similarities between antibiotics and other fever medicines, with participants in Mozambique using the terms paracetamol and antibiotics interchangeably while describing self-medication practices. Additionally, in rural Ghana22 and in rural UP in India,12 antibiotics were indiscriminately equated with general medicines, such as painkillers, and employed for treating diverse conditions such as stomach aches, body sores, respiratory infections, diarrhoea and other ailments that do not inherently necessitate antibiotic intervention. Cumulatively, these findings strongly signify widespread misperceptions, wherein antibiotics are erroneously perceived as analogous to general symptom-alleviating drugs, leading to their inappropriate use for a broad spectrum of infections, irrespective of their aetiology.
Misperceptions about how antibiotics work and about drug resistance10 11 21 have also been identified as important reasons for non-compliance and self-medication. Our findings support this relationship, but we have also uncovered an additional layer of distrust of biomedicines, perhaps shaped by non-western belief systems of health and causality. Non-biomedical health models such as Ayurveda emphasise the role of nature’s elements in illnesses, rather than the singular presence of invisible disease-causing microorganisms that form the core of western biomedicine. Our FGD narratives pointed to an intrinsic fear that continuing an antibiotic beyond the recovery period might harm the body by generating toxicity, a perception linked to Ayurvedic principles of maintaining good health through balancing bodily elements.36 This suggests a natural predilection among these rural communities to be suspicious of an overuse of antibiotics, a perception that could potentially be drawn on to prevent antibiotic overuse.
However, an important implication of this finding is that even if the economic constraints on purchasing optimal antibiotic courses are removed, by providing free essential antibiotics, changing antibiotic practices will still be a challenge, given people’s conflicting relationship with the drugs. It must be noted however that existing recommendations on what constitutes a full antibiotic course are challenged by new evidence that short course antibiotics (for 3–7 days) are as effective as longer courses (>7 days) for most infections seen in outpatient care.37 For example, in hospitalised children with community-acquired pneumonia, a 3-day course has been found to be as effective as a 7-day course.38 This evidence urgently needs to be integrated into existing national guidelines and recommendations to enable greater course compliance in future.
Our research underscores the pivotal role of community healthcare providers as reliable and accessible reservoirs of antibiotic-related information, a theme echoed in other studies in Asia and Africa.22 23 In rural Ghana, for example, the adoption of antibiotic practices for conditions such as hernia and stomach ache was found to be influenced by diverse sources, including over-the-counter medicine sellers, drug peddlers, pharmacies, doctors, as well as information from family and friends.22 Our study extends these observations by elucidating the intricate interplay between both physical and social access to healthcare providers, shedding light on their impact on both healthcare-seeking behaviours and the patterns of antibiotic utilisation. This analysis, presented diagrammatically in figure 2, shows a stark health system divide based on trust, accessibility and availability of healthcare providers. Community-level providers, such as ASHAs, IPs and pharmacists, are characterised by physical and social accessibility but often lack comprehensive antibiotic knowledge. In contrast, formally trained healthcare providers, notably qualified doctors, possess greater knowledge but maintain a social distance and employ a paternalistic communication style. This cultural divide, prevalent in hierarchical societies of South and Southeast Asia,39 contributes to a patient–provider gap, wherein patients may lack agency to negotiate their relationship with providers, fostering reduced patient involvement. This cycle necessitates further investigation, as patient–provider communication significantly influences patient satisfaction and treatment compliance. Addressing this social disconnect demands enhanced communication training in medical colleges as well as strategies to empower patients, particularly those from economically disadvantaged backgrounds.
Another point of concern is the role of ANMs in our study dispensing just a few doses of antibiotics to patients and referring them to a PHC to get the rest. This practice could lead to suboptimal antibiotic consumption as patients are unlikely to travel to a distant health facility after receiving the first few doses nearby. In line with the World Health Organisation's AWARE classification of antibiotics that distinguishes between ACCESS (first line antibiotics for a wide range of infections), WATCH (antibiotics to be used sparingly) and RESERVE (last resort antibiotics) antibiotics,40 a set of affordable ACCESS antibiotics can be made widely available through all available community providers with proper guidance and information, so that the riskier WATCH and RESERVE antibiotics can be protected.
It is also necessary to examine and mitigate the perceptions that people have, regarding the poor quality of drugs in government-run facilities, a finding consistent with other studies in India.41 These perceptions could be due to several reasons: IPs may be giving stronger antibiotics that are therefore seen to be more effective, or these perceptions may be linked with a general distrust of the public system and of generic medicines due to extensive pharmaceutical promotion of branded medicines, as reported elsewhere.41 There may also be genuine problems with the quality of government drugs in some facilities that needs to be ascertained and the public reassured. This is an important research agenda for the future.
Finally, our study highlighted important gender and age-related issues that need to be kept in mind while designing accessible and equitable health services and awareness campaigns. Other studies from rural India have also reported that families may be more careful about course compliance for children than for adults13 and that self-medication may be prevalent across adults of both genders, although more so among men.12 An important finding in our study was that women with young children and the elderly have mobility issues and are most reliant on their nearby providers who must be supported in delivering both essential services and health information. These issues need to be addressed in awareness campaigns and in improved configuration of health services to address the needs of women and the elderly.
Strengths and limitations
In contrast to predominant examinations focusing on individual factors in community antibiotic practices, our study employs a comprehensive multilevel framework, offering a more nuanced understanding of the intricate interplay between community and health system factors alongside individual-level influences shaping antibiotic practices. Using qualitative research methods facilitated an in-depth exploration of infectious disease perceptions and non-biomedical belief models, providing valuable insights into the cognitive foundations influencing community antibiotic practices. The inclusion of vulnerable groups, such as pregnant women and the elderly, allowed for a nuanced examination of their information needs regarding antibiotics. Despite limitations, such as the absence of interviews with IPs in this round of data collection, the study draws on earlier data15 31 to supplement and triangulate findings. While our study is specific to two village clusters in one district of West Bengal, it sheds light on broader issues, such as infrastructural and human resource inadequacies in the public sector and the widespread reliance on IPs, which are well documented in other rural Indian settings.13 17 42
Conclusions
This study reveals the intricate web of influences shaping antibiotic usage, encompassing individual sociodemographics, cognitive factors, affective influences and economic constraints. Recognising this complexity is crucial for designing effective interventions. Community leaders and health workers emerge as key players in shaping community antibiotic practices. However, their insufficient knowledge and capacity underscores the need for targeted training programmes to enhance their capacity as health educators and knowledge brokers.
Our findings have several implications for tailored educational initiatives, capacity building for CHWs, policy interventions to improve access to antibiotics and integrated health stewardship models. Many of these are relevant for rural community settings in LMICs in Asia and Africa. Educational initiatives should address sociodemographic factors, cognitive and emotive aspects, and economic considerations. They should enable identification of antibiotics versus other drugs for symptomatic relief in acute illnesses. AMR-related communication needs to be integrated into existing sanitation and hygiene campaigns, maternal and child health advocacy programmes, TB and HIV control programme and toilet promotion campaigns. Given the pivotal role of CHWs in enabling access to information as well as antibiotics, there is a necessity for comprehensive training programmes, promotion of antibiotic use guidelines and policy shifts to enable judicious antibiotic sales and dispensing at that level. Awareness programmes for antibiotic providers that promote understanding of antibiotics and antibiotic resistance through tailored interventions may be helpful in changing current antibiotic sales practices.
In India, given the importance of community leaders as health stewards lies the opportunity to develop integrated health stewardship models that leverage local leadership. Collaborative efforts involving community leaders, healthcare providers and public health authorities can foster a holistic approach to health promotion, including responsible antibiotic use. Finally, recognising the coexistence of traditional and biomedical belief systems, communication strategies about antibiotic use, should be culturally sensitive. Tailoring these strategies to align with local beliefs and practices can enhance their effectiveness in India and serve as a model for similar adaptations in other countries facing comparable challenges.
Data availability statement
Data are available upon reasonable request. Anonymised transcripts that do not pose any risk to participants’ confidentiality can be made available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval was obtained from—the LSHTM Ethics Committee (LSHTM Ethics Ref: 17484)—the Institutional Ethics Committee of the Indian Institute of Liver and Digestive Sciences, West Bengal, the initial study partner (No. IILDS/IECHR/01/2019). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We gratefully acknowledge the valuable participation of all our study participants including community members, village leaders and health workers, and the kind support of all those stakeholders who facilitated access for us to the study communities.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MG and SB are joint first authors.
Twitter @gautham_meen
Contributors MG and SB jointly conceptualised the study, developed study guides, supervised data collection, led the analysis and drafted the manuscript. MG was the overall PI and secured funding for the study. MBR and SM collected, transcribed and coded the data and conducted the preliminary literature search. PB, AE and GB contributed to the study conceptualisation, analysis discussions, drafting of parts of the manuscript and critically reviewed the manuscript. MG ans SB are study guarantors.
Funding Financial support for this study was through a Health Systems Research Initiative grant (Ref: MR/S013598/1) jointly funded by the Medical Research Council, the Economic and Social Research Council, the Foreign, Commonwealth and Development Office and Wellcome Trust, UK.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.