Article Text

Abstract
Objective To demonstrate that acupuncture is beneficial for decreasing the risk of ischaemic stroke in patients with rheumatoid arthritis (RA).
Design A propensity score-matched cohort study.
Setting A nationwide population-based study.
Participants Patients with RA diagnosed between 1 January 1997 and 31 December 2010, through the National Health Insurance Research Database in Taiwan.
Interventions Patients who were administered acupuncture therapy from the initial date of RA diagnosis to 31 December 2010 were included in the acupuncture cohort. Patients who did not receive acupuncture treatment during the same time interval constituted the no-acupuncture cohort.
Primary outcome measures A Cox regression model was used to adjust for age, sex, comorbidities, and types of drugs used. We compared the subhazard ratios (SHRs) of ischaemic stroke between these two cohorts through competing-risks regression models.
Results After 1:1 propensity score matching, a total of 23 226 patients with newly diagnosed RA were equally subgrouped into acupuncture cohort or no-acupuncture cohort according to their use of acupuncture. The basic characteristics of these patients were similar. A lower cumulative incidence of ischaemic stroke was found in the acupuncture cohort (log-rank test, p<0.001; immortal time (period from initial diagnosis of RA to index date) 1065 days; mean number of acupuncture visits 9.83. In the end, 341 patients in the acupuncture cohort (5.95 per 1000 person-years) and 605 patients in the no-acupuncture cohort (12.4 per 1000 person-years) experienced ischaemic stroke (adjusted SHR 0.57, 95% CI 0.50 to 0.65). The advantage of lowering ischaemic stroke incidence through acupuncture therapy in RA patients was independent of sex, age, types of drugs used, and comorbidities.
Conclusions This study showed the beneficial effect of acupuncture in reducing the incidence of ischaemic stroke in patients with RA.
- Acupuncture
- Cardiovascular diseases
- National Health Insurance Research Database
- Rheumatoid arthritis
- Stroke
Data availability statement
Data are available upon reasonable request.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Acupuncture
- Cardiovascular diseases
- National Health Insurance Research Database
- Rheumatoid arthritis
- Stroke
STRENGTHS AND LIMITATIONS OF THIS STUDY
Our research discloses the possible long-term effect of acupuncture on stroke prevention that could not be investigated in clinical trials.
Lower incidence of ischaemic stroke developed in patients with rheumatoid arthritis after acupuncture therapy.
The causality could not be proven directly through our study design.
Introduction
Rheumatoid arthritis (RA) is a common rheumatoid disease that manifests as polyarthritis in the joints, mainly synovial inflammation and morning stiffness.1 Bone erosion, joint deformity, and loss of functional abilities are long-term complications of RA. In regard to chronic processes, the inflammation status can be noted in the whole body: pericarditis, myocarditis, pleuritis, interstitial lung fibrosis, osteoporosis, and cardiovascular disease.2–5 Comorbidities from cardiovascular disease, such as stroke, are the major cause of death in RA patients.6–11 Compared with the general population, stroke is more common in RA patients.12 The prevalence of RA globally and in Asia is 460 per 100 000 people and 15.8 per 100 000 people, respectively.13–15 However, the risk of developing ischaemic stroke in Asian RA patients (hazard ratio (HR) 1.32) is similar to that in Caucasian populations (HR 1.29).16 17
Determining the agents to prevent stroke is an essential issue for clinical doctors and patients.18 The common prescriptions to treat RA are non-steroidal anti-inflammatory drugs (NSAIDs), steroids, conventional disease-modifying antirheumatic drugs (DMARDs), and biological agents such as etanercept, infliximab (TNF-α inhibitor), and anakinra (IL-1 inhibitor).3 5 19 Steroids and DMARDs, such as methotrexate and infliximab, have advantages in the prevention of ischaemic stroke in RA patients.18 However, some of them could result in complications in the bone marrow that cause thrombocytopenia.20 Finding alternative interventions to control RA while lowering complications from treatment itself has become a well-discussed topic.
In many countries, such as Taiwan, Germany, and China, acupuncture therapy is widely used to control pain when patients have musculoskeletal and immune problems, including RA.21–25 A previous cohort study found that approximately 27.3% of RA patients in Taiwan ever consulted traditional Chinese medicine (TCM) services, and 23.6% of these patients had received acupuncture.26 Furthermore, secondary stroke prevention is also noted to result from acupuncture therapy in the Taiwanese population.27 The hypothesised mechanism by which acupuncture lowers the stroke rate is similar to that of anti-RA agents—anti-inflammation. Thus, we wanted to investigate the relationship between acupuncture intervention and the incidence of ischaemic stroke in RA patients.
In Taiwan, the records of medical services are saved in the database of the National Health Insurance (NHI) program—the National Health Insurance Research Database (NHIRD). This service of the NHI has been operating from 1995 until now, and the coverage rate in the Taiwanese population is more than 99%.28 In other words, the medical data in the NHIRD cover a long enough time and are large enough to be used for nationwide population research. Sampling bias could be prevented when the study is conducted through such a large-scale database.29 We used the NHIRD to investigate the long-term effect of ischaemic stroke prevention in patients with RA who accepted acupuncture treatment.
Methods
Data sources
A nationwide, population-based 1:1 propensity score-matched cohort study via data analysis derived from the NHIRD was performed. The database used in this study was the Registry for Catastrophic Illness Patients Database (RCIPD), which is part of the NHIRD. Personal information was removed from the NHIRD. It was not possible to involve patients or the public in the design, conduct, reporting, or dissemination plans of our research. The RCIPD enrolled all patients with a catastrophic illness, which was proven by pathological, laboratory, and clinical diagnoses by both specialists and a regular review. This real-world database consists of datasets including demographic characteristics, outpatient and inpatient visits, diagnostic codes, assessments, remedies, procedures, and medical expenses for reimbursement. The diagnoses were coded by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Patients with a diagnosis of RA are issued catastrophic illness certificates and receive free medical services for health complications. Thus, the RCIPD is an ideal comprehensive database for the investigation of all RA patients in Taiwan. The Research Ethics Committee of China Medical University and Hospital in Taiwan approved this study (CMUH109-REC2-031 (CR-3)).
Study subjects and variables
We used both ambulatory and inpatient medical records to identify RA treatments that were linked with the RCIPD from 1997 to 2010 to identify a study population (n=47 809) for follow-up until the end of 2011 (figure 1). Newly diagnosed RA patients (n=36 277) with a diagnosis of ICD-9-CM code 714.0 were included. We excluded patients (n=1793) as follows: (1) patients who were younger than 18 years; (2) patients who had incomplete data on age or sex; (3) patients who had an interruption in health insurance services during the follow-up period; and (4) patients who had a diagnosis of ischaemic stroke (ICD-9-CM: 433–438) before the index date. Finally, 23 226 newly diagnosed RA patients were included. Patients who received acupuncture therapy from the initial RA diagnosis to 31 December 2010 were included in the acupuncture cohort (n=12 266). We used a propensity score approach to minimise confounders in the analysis of acupuncture therapy. A one-to-one propensity score match was conducted by age (per 5 years), sex, comorbidities, types of drugs used (oral steroids, NSAIDs, statins, all DMARDs), RA diagnosis year and index year by multiple logistic regression analysis. The definition of drugs used was patients with ≥28 cumulative use days. The numbers of participants in both the acupuncture and no-acupuncture cohorts were the same (n=11 613). The index date was defined as the first time that patients received acupuncture therapy, which was given randomly to patients in the no-acupuncture cohort according to the approach in the acupuncture cohort. The immortal time was defined as the period from the initial diagnosis of RA to the index date.

Study population flowchart. A total of 47 809 patients with RA were newly diagnosed from 1997 to 2010. Sex, age, comorbidities, types of drugs used, RA diagnosis year and index year were processed via 1:1 matching; subsequently, 11 613 patients were included in the acupuncture and no-acupuncture cohorts, respectively. RA, rheumatoid arthritis.
Covariate assessment
The patients were assigned to three groups by age (18–39 years, 40–59 years, and ≥60 years). ICD-9-CM codes of comorbidities that appeared more than once in the outpatient or inpatient records before the primary diagnosis of RA were taken into consideration; such comorbidities included diabetes mellitus (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401–405), hyperlipidaemia (ICD-9-CM code 272), congestive heart failure (ICD-9-CM codes 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, and 428.0), anxiety (ICD-9-CM codes 300.0, 300.2, 300.3, 308.3, and 308.91), depression (ICD-9-CM 296.2–296.3, 300.4, 311), alcoholism (ICD-9-CM codes 291, 303, 305.00–305.03, 790.3, and V11.3), tobacco use (ICD-9-CM code 305.1), obesity (ICD-9-CM codes 278 and A183), and atrial fibrillation (ICD-9-CM 427.3). The events of ischaemic stroke (ICD-9-CM: 433–438) were compared between the acupuncture and no-acupuncture cohorts of RA patients.
Types of acupuncture and disease categories in the acupuncture cohort
We identified the different acupuncture types by the treatment codes, including manual acupuncture (B41, B42, B45, B46, B80, B81, B82, B83, B84, B90, B91, B92, B93, B94, P27041, P31103, and P32103) and electroacupuncture (B43, B44, B86, B87, B88, and B89), as previously described.30
Statistical analyses
The standardised mean difference (SMD) was used to compare the baseline characteristics of the acupuncture and no-acupuncture cohorts as previously described.30 A negligible difference in mean values or proportions between the two cohorts was defined as <0.1 SD. Competing-risk regression models were performed to estimate the crude and adjusted subhazard ratios (SHRs) of acupuncture therapy, age, sex, comorbidities, and types of drugs used. The Kaplan-Meier method and the log-rank test were conducted to find the difference between the two cohorts in the development of ischaemic stroke. We used SAS 9.4 (SAS Institute, Cary, NC, USA) and R software (R Foundation for Statistical Computing, Vienna, Austria) to perform statistical analyses and create the figures. Statistical significance was defined as p<0.05 in two-tailed tests.
Patient and public involvement
None
Results
We used 1:1 propensity score matching by sex, age, all comorbidities, drugs (oral steroids, NSAIDs, statins, all DMARDs), RA diagnosis year and index year to enrol an equal number (n=11 613) of RA patients in the acupuncture cohort and no-acupuncture cohort, respectively (figure 1). The baseline characteristics of both cohorts are presented in table 1, with similar distributions of sex, age, comorbidities, and prescriptions. In both cohorts, most participants were female, and most patients were middle-aged (40–59 years). The most common comorbidity was hypertension; more than 38% of patients had this problem. In patients with RA, 18% had diabetes mellitus, 28% had hyperlipidaemia, 6% had congestive heart failure, 24% had anxiety, and 10% had depression. There were no differences in the proportions of alcoholism, tobacco dependence, or obesity between the two cohorts. NSAIDs were the most common prescriptions in both cohorts, and 76% of the included patients were on these medications. In the participants of the two cohorts, 55% used oral steroids and 5% used statin agents. Most patients (87%) were treated by manual acupuncture, with electroacupuncture having been used in 3% of the participants; the remaining 10% had combined manual acupuncture and electroacupuncture treatments. The mean duration between RA diagnosis and the first acupuncture treatment was approximately 1065 days. The mean number of acupuncture visits was 9.83.
Characteristics of rheumatoid arthritis patients according to whether they received acupuncture treatment
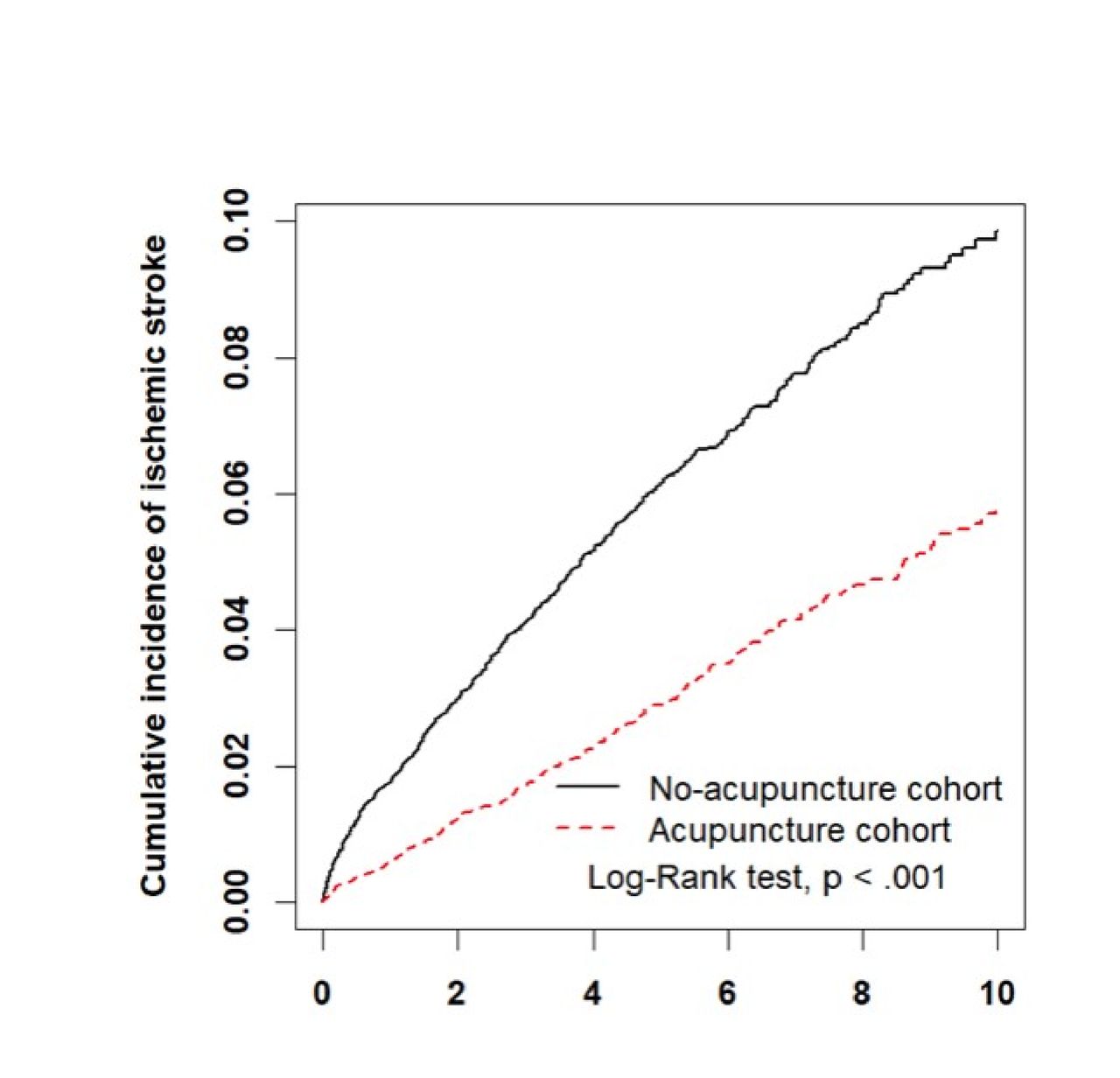
During the follow-up period, 946 patients developed ischaemic stroke (online supplemental table 1). The incidence of ischaemic stroke in RA patients increased with age, with older patients having a higher risk. The adjusted SHRs in the 40- to 59-year-old group and the over 60-year-old group were 5.99 and 14.7, respectively. The patients with comorbidities of diabetes mellitus, hypertension and congestive heart failure had a higher risk of ischaemic stroke. The adjusted SHRs of the patients with diabetes mellitus, hypertension and congestive heart failure were 1.58, 2.10 and 1.31, respectively. The cumulative incidence of ischaemic stroke was significantly lower in the acupuncture cohort (log-rank test, p<0.001) (figure 2).
Supplemental material

{kind=link}
{kind=link}
The cumulative incidence of ischaemic stroke in acupuncture (dashed line) cohort and the no-acupuncture cohort (solid line). Patients in the acupuncture group had a lower incidence of ischaemic stroke (log-rank test, p<0.001).
Online supplemental table 2 shows that the 341 patients in the acupuncture cohort (5.95 per 1000 person-years) and the 605 patients in the no-acupuncture cohort (12.4 per 1000 person-years) developed ischaemic stroke (adjusted SHR 0.57, 95% CI 0.50 to 0.65). Both males and females were observed to experience the benefit of ischaemic stroke prevention, with an adjusted SHR of 0.58 in the female group (95% CI 0.49 to 0.67) and an adjusted SHR of 0.54 in the male group (95% CI 0.41 to 0.70). Patients in the age subgroup ≥40 years old had a lower risk of ischaemic stroke after acupuncture therapy (adjusted SHR 0.54, 95% CI 0.44 to 0.66 in the 40- to 59-year-old group; adjusted SHR 0.58, 95% CI 0.48 to 0.69 in the over 60-year-old group). Acupuncture decreased the risk of ischaemic stroke in most patients with comorbidities. Coprescriptions with steroids, statins or DMARDs did not change the positive results of acupuncture therapy.
The results from the non-matching analysis were also provided to prevent possible sampling bias from our 1:1 propensity score matching in online supplemental tables 3 and 4. The final results analysed by competing-risk regression models are compatible with the results after 1:1 propensity score matching.
Discussion
To the best of our knowledge, this is the first study to show that acupuncture therapy is beneficial for ischaemic stroke prevention in RA patients. RA is one of the common disease categories among acupuncture visits in Taiwan.31 We previously found that 23.6% of RA patients had received acupuncture.26 In the present study, we showed that the benefit of acupuncture therapy in reducing the risk of ischaemic stroke was independent of sex, age, and comorbidities.
Although patients with RA have been known to have a high risk for the development of stroke, there is an unmet need to improve preventive measures for patients with RA.32 Inflammation is a consistent and independent predictor of cardiovascular disease in RA.33 TNF-α is a cytokine that mediates inflammatory reactions.34 A high level of TNF-α has been observed in RA patients, and it has been found that TNF-α can induce pannus formation and subsequent bone destruction.35 By interrupting TNF-α expression and production by inflammatory cells, TNF-α inhibitors can efficiently control the inflammatory process.36 Biological agents targeting cytokines may decrease cardiovascular disease risk in RA.37 Therefore, it would be of interest to know whether acupuncture fits the niche to reduce inflammation in RA patients.
There are some evidence and potential explanations about the effects and mechanisms of acupuncture. Acupuncture has been reported to be effective in treating neuropathy,38 relieving pain39 and attenuating cardiovascular disease40 in different clinical trials. Previous clinical studies revealed that acupuncture reduced the number of tender joints, relieved morning stiffness and joint pain, enhanced physical activity, and improved quality of life in patients with RA.41 42 In the analysis of blood and synovial fluid of RA patients, acupuncture was found to reduce TNF-α and vascular endothelial growth factor to improve the inflammation of RA.43 In animal studies, acupuncture reduced inflammation in a collagen-induced arthritis model.44–46 Furthermore, acupuncture not only has analgesic effects through β-endorphin,47 adenosine48 and orexin,49 but also reduces inflammation through dopamine.50 On the other hand, unstable blood pressure and lipid profiles are the two risk factors for ischaemic stroke, and acupuncture therapy has the advantage of controlling both hypertension and dyslipidaemia.51 52 If acupuncture relieves morning stiffness and joint pain, patients might also benefit from increasing daily activities, which might also reduce the risk of stroke.53
Our study has some limitations. For example, we could not identify the number and specific affected joints from the data of the RCIPD. Thus, we used prescriptions for RA treatment as variables that could represent the severity of RA. After performing 1:1 propensity score matching, the differences between the two cohorts were minimised. We had similar percentages of patients who used NSAIDs, steroid agents, statins, and DMARDs. The second limitation was that the RCIPD did not provide data on height, weight, laboratory data or exercise status. We tried to define a diagnosis of alcoholism, tobacco use, and obesity to represent these personal characteristics and lifestyles; then, through 1:1 propensity score matching, we attempted to eliminate or minimise confounders.54 The distribution of patients with different habits was similar, and these parameters did not change the significant effect of ischaemic stroke prevention in patients with RA. The algorithm for risk of developing cardiovascular events, such as the Framingham Risk Score, is hard to formulate because of the lack of the above information. Additionally, the RCIPD database could not offer information on acupoints for RA treatment. The selection of acupoints depends on the diagnosis and the experience of TCM doctors. The variable prescriptions of acupuncture could also stem from the different complaints, comorbidities and expectations of the patients. Because of the standard TCM programme training in medical schools, most TCM doctors in Taiwan know the concepts of basic acupoints, such as LI11, ST36, and SP9 (online supplemental figure 1).55 56 Further clinical trials with standardised acupoints should be conducted based on the findings of this study. The difference in treatment results among various types of interventions could not be discovered in our database and was not included as a result measure. The evidence of the treatment dose of acupuncture therapy is still being established; thus, we did not discuss the topic here.
Supplemental material
Conclusions
Our study demonstrates that the ischaemic stroke risk could be reduced by acupuncture treatment in patients with RA in Taiwan. The possible mechanism may involve reducing proinflammatory cytokines through acupuncture therapy, thereby attenuating cardiovascular disease, including ischaemic stroke. The study also offers important ideas for more comprehensive research in the future.
Data availability statement
Data are available upon reasonable request.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
This study was based in part on data from the National Health Insurance Research Database. We are grateful to Health Data Science Center, China Medical University Hospital for providing administrative, technical and funding support. The interpretation and conclusions contained herein do not represent those of the National Health Insurance Administration, Ministry of Health and Welfare, or China Medical University Hospital, Taiwan.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Press release
Press release
- Press release -
Press release
- Press release -
Footnotes
C-YH and M-CH are joint first authors.
X @YenHungRong1
C-YH and M-CH contributed equally.
M-YW and H-RY contributed equally.
Authors’ contributions CYH and MCH contributed equally as co-first authors. MCH contributed to the conception of the study, participated in the interpretation of clinical data and drafted the manuscript. CYH contributed to the conception of the study, participated in the interpretation of clinical data and drafted the manuscript. HHL participated in the interpretation of clinical data and drafted the manuscript. CLL performed the statistical analysis. GZ drafted the manuscript. MYW contributed to the design of the study, participated in the interpretation of clinical data and drafted the manuscript. YCL supervised the project, participated in the interpretation of clinical data and drafted the manuscript. HRY supervised the project, contributed to the conception and design of the study and finalised the manuscript. HRY is the gurantor. MYW and HRY contributed equally as co-corresponding authors.
Funding This work was financially supported by the 'Chinese Medicine Research Centre, China Medical University' from the Featured Areas Research Centre Programme within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan (CMRC-CHM-1). This study was also supported in part by China Medical University (CMU103-BC-4–2, CMU105-BC-1–1, CMU105-BC-1–2), China Medical University Hospital (DMR-107–011, DMR-110–002, and DMR-111–105), and the Ministry of Science and Technology (MOST108-2638-B-039–001-MY2, MOST107-2320-B-039–037, MOST108-2320-B-039–021, MOST110-2321-B- 039–003, and NSTC 112-2327-B-039-005). This study is also supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial Centre (MOHW111-TDU-B-212–1 34 004), Taiwan. None of the funders and institutions listed had a role in the design and conduct of the study, the collection, management, analysis, and interpretation of the data, the preparation, review, or approval of the manuscript, or the decision to submit the manuscript for publication.
Competing interests The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Ethics Approval Statement The Research Ethics Committee of China Medical University and Hospital in Taiwan approved this study (CMUH109-REC2-031(CR-3)).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.