Article Text

Abstract
Objectives To examine the 36-year trends in tobacco use in northern Sweden.
Design and outcome measure Cross-sectional analysis of the eight population-based surveys that constitute the northern Sweden MONICA study (1986, 1990, 1994, 1999, 2004, 2009, 2014 and 2022). Cigarette smoking and snus use were self-reported via questionnaires, and age-adjusted percentages of cigarette smoking (including occasional use) and snus use were calculated via logit models.
Setting General population of Norrbotten and Västerbotten (the two northernmost counties of Sweden).
Participants 6678 women and 6320 men, aged 25 to 74 years, were included for analysis. A total of 191 participants were excluded due to missing data on either cigarette smoking or snus use.
Results Cigarette smoking decreased on a survey-to-survey basis, reaching a minimum in 2022 of 4.9% among men and 9.7% among women, corresponding to a percentage point change of 26.3 and 20.8, respectively, compared with 1986 (pwithin-group<0.01). With respect to snus, the use increased steeply up until 1999 among men, after which it persisted around 25% to 30% (26.2% in 2022), with percentage point changes between 6.6 and 13.4 compared with 1986 (pwithin-group<0.01). The percentage of female snus users was extremely low in the first surveys but increased continuously over time, reaching a maximum of 13.0% in 2022 and a percentage point change of 12.5 since 1986 (pwithin-group<0.01). Cigarette smoking—but not snus use—was more common in Norrbotten than in Västerbotten in 2022 (pbetween-group<0.01).
Conclusions A substantial decline in cigarette smoking has occurred over time in northern Sweden, particularly among men and more notably in Västerbotten. In contrast, snus use has become increasingly common in both sexes and in both counties.
- Tobacco Use
- EPIDEMIOLOGY
- PUBLIC HEALTH
Data availability statement
Data are available upon reasonable request. Access to individual-level data can be provided for research purposes but is restricted by laws regarding the privacy of research participants and are, therefore, not made publicly available. Requests for data can be sent to the Section of Biobank and Registry Support at Umeå University (contact: info.brs@umu.se).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The primary strength of this study was the large number of participants, recruited at eight different occasions over a 36-year time period.
Another strength was that the main questions on cigarette smoking and snus use were identical in all surveys.
The main limitation of this study was the decline in participation rate over time, from 81% in 1986 to 47% in 2022.
Another limitation was that the use of tobacco products was self-reported.
Introduction
Cigarette smoking is a major contributor to ill health and a known risk factor for, among others, cardiovascular disease, lung disease, diabetes and cancer.1–5 While the health effects of snus (a type of moist tobacco, placed under the lip in either loose or portion-packed form) are not as well-established as those of cigarettes,6 several studies have observed an association between snus use and increased risk of diabetes, overall mortality and cardiovascular mortality.7–12 Snus has been, and still is, mainly used in Nordic countries, especially in Sweden, where its use has been more or less widespread since the 19th century (as reviewed by Nordgren and Ramström).13
The popularity of cigarettes and snus has followed opposite trends in Sweden over the past decades (decrease in cigarette smoking, increase in snus use). As an example, based on national data between 2008 and 2022, the percentage of cigarette smokers decreased from 15.3% to 8.5% among women and from 12.9% to 8.8% among men, while the percentage of snus users increased from 3.2% to 7.1% among women and from 20.1% to 22.9% among men.14 In the 2019 Eurostat survey, the prevalence of cigarette smoking was 1.5 to 5.3 percentage points lower in Sweden than in other Nordic countries.15 The temporal changes in Sweden are even more evident in the Northern Sweden Monitoring of Trends and Determinants in Cardiovascular Disease (NS-MONICA) study, which has data dating back to the 1980s. Cigarette smoking decreased by 15 percentage points among women and by 12 percentage points among men between 1986 and 2009, and snus use increased by 9 percentage points among women and by 15 percentage points among men during the same time period.16
The aim of this study was to give an up-to-date description of the tobacco use and its associated characteristics in northern Sweden, using data spanning over 36 years from the NS-MONICA cohort.
Methods
Study population
The NS-MONICA study was originally part of a WHO initiative to monitor cardiovascular risk factors.17–19 Starting in 1986, eight population-based surveys have been conducted in the two northernmost counties of Sweden, Norrbotten and Västerbotten, and include more than 13 000 participants. Each survey was an independent sample of randomly selected persons from the population registers, stratified for sex and age (25–64 years in 1986–1990; 25–74 years in 1994–2022). The participants answered a questionnaire, underwent a clinical examination and had blood samples drawn. The participation rate decreased over time, from 81% in 1986 to 47% in 2022 (online supplemental figure S1). Details on non-participation data with respect to tobacco use are presented in online supplemental text S1.
Supplemental material
The NS-MONICA study is covered by multiple ethical approvals from the Regional Ethical Committee at Umeå University and from the Swedish Ethical Review Authority. Reporting was done in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.20
Assessment of cigarette smoking and snus use
The questionnaires contained a number of questions on the current and previous use of cigarettes and snus. The main questions on current cigarette smoking and snus use were identical in the eight surveys, as exemplified in online supplemental figure S2. Cigarette questions were in general more detailed than snus questions; for example, the questionnaires differentiated between regular and occasional smoking (≥1 and <1 cigarette per day) and collected information on time since smoking cessation. Questions on the type of snus were only included in 2014 and 2022 (loose or portion-packed) and questions on the use of electronic cigarettes were only included in 2022.
The main questions on tobacco use in the NS-MONICA study have previously been validated with good results by comparing self-reported data with plasma concentrations of cotinine (the predominant nicotine metabolite).21
Assessment of other variables
Information on educational level, civil status, and diagnosis of diabetes and high blood pressure was collected via the questionnaires. Blood pressure, height and weight were measured during the clinical examination. Body Mass Index (BMI) was calculated as weight (kg) divided by height squared (m2) and hypertension was defined by systolic blood pressure of 140 mm Hg or more, diastolic blood pressure of 90 mm Hg or more, and/or diagnosis of high blood pressure.
Statistical analysis
The analytical cohort included 12 998 participants, after exclusion of 191 participants with missing data on either cigarette smoking or snus use (to have a common denominator in the time-trend analysis; online supplemental figure S1). All analyses were conducted using Stata V.14 (StataCorp LP, College Station, TX, USA).
Sex-specific percentages of cigarette smoking (including occasional use) and snus use were calculated in each survey via logit models. Between-survey differences in the age structure were accounted for by (i) adjustment (as a continuous covariate, with percentages estimated at 46.5 years (the median age of tobacco users) in main analyses and at 30, 40, 50 and 60 years in secondary analyses) and (ii) stratification (25–34, 35–44, 45–54, 55–64, 65–74 years). In the latter analysis, to avoid overemphasising findings due to small sample variability, the eight surveys were collapsed into four categories (1986–1990, 1994–1999, 2004–2009, 2014–2022). In addition, to examine the impact of the so-called Västerbotten Intervention Programme (a cardiovascular prevention programme, fully implemented in Västerbotten in 1993),22 separate analyses were conducted by county of residence. Finally, we calculated how the observed percentages of regular cigarette smoking in the 2022 survey would have changed at different participation rates and at different smoking percentages among non-participants (online supplemental text S2), with the purpose to examine the effect of potential selection bias.
Demographic and health characteristics were calculated by tobacco use in the 2022 survey, adjusted for sex and age where appropriate, via quantile and logit models (for continuous and categorical covariates, respectively). The same characteristics were also calculated among tobacco users for the left-tail (1986–1990) and right-tail (2014–2022) of the survey year distribution. Missing data were handled using complete case analysis (online supplemental table S1).
Patient and public involvement
Participants and the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Results
Study population
A total of 6678 women (median age, 49.0 years) and 6320 men (median age, 50.3 years) were included for analysis (online supplemental figure S1), of whom 20.2% smoked cigarettes (median age, 47.3 years; 54.8% women; 21.2% occasional use) and 14.9% used snus (median age, 44.2 years; 20.7% women). 3.0% used both cigarettes and snus (median age, 41.5 years; 17.8% women).
Tobacco use
The sex-specific percentages of tobacco use are shown in figure 1 (main analysis; tabulated in online supplemental table S2,S3) and online supplemental figure S3 (secondary analysis). Cigarette smoking decreased on a survey-to-survey basis (curvilinear among men, linear among women), reaching a minimum in 2022 of 4.9% among men and 9.7% among women, corresponding to a percentage point change of 26.3 and 20.8, respectively, compared with 1986 (pwithin-group<0.01). Four men and seven women also reported use of electronic cigarettes in 2022. With respect to snus, the use increased steeply up until 1999 among men, after which it persisted around 25% to 30% (26.2% in 2022), with percentage point changes between 6.6 and 13.4 compared with 1986 (pwithin-group<0.01). The percentage of female snus users was extremely low in the first surveys but increased continuously over time, reaching a maximum of 13.0% in 2022 and a percentage point change of 12.5 since 1986 (pwithin-group<0.01).

Percentage of tobacco use by sex (1986–2022). All estimates were obtained from logit models, adjusted for age (continuous, years) and predicted at the median age of tobacco users in the eight surveys (46.5 years). In the upper panels, dots and spiked caps represent percentages and 95% CIs in women (dark grey) and men (light grey). In the lower panels, dots represent percentage point change in each sex compared with the survey in 1986 (CIs are omitted for visual clarity). Solid lines represent the predicted change in percentage points per year, including a squared term for calendar year (to relax the linearity assumption).
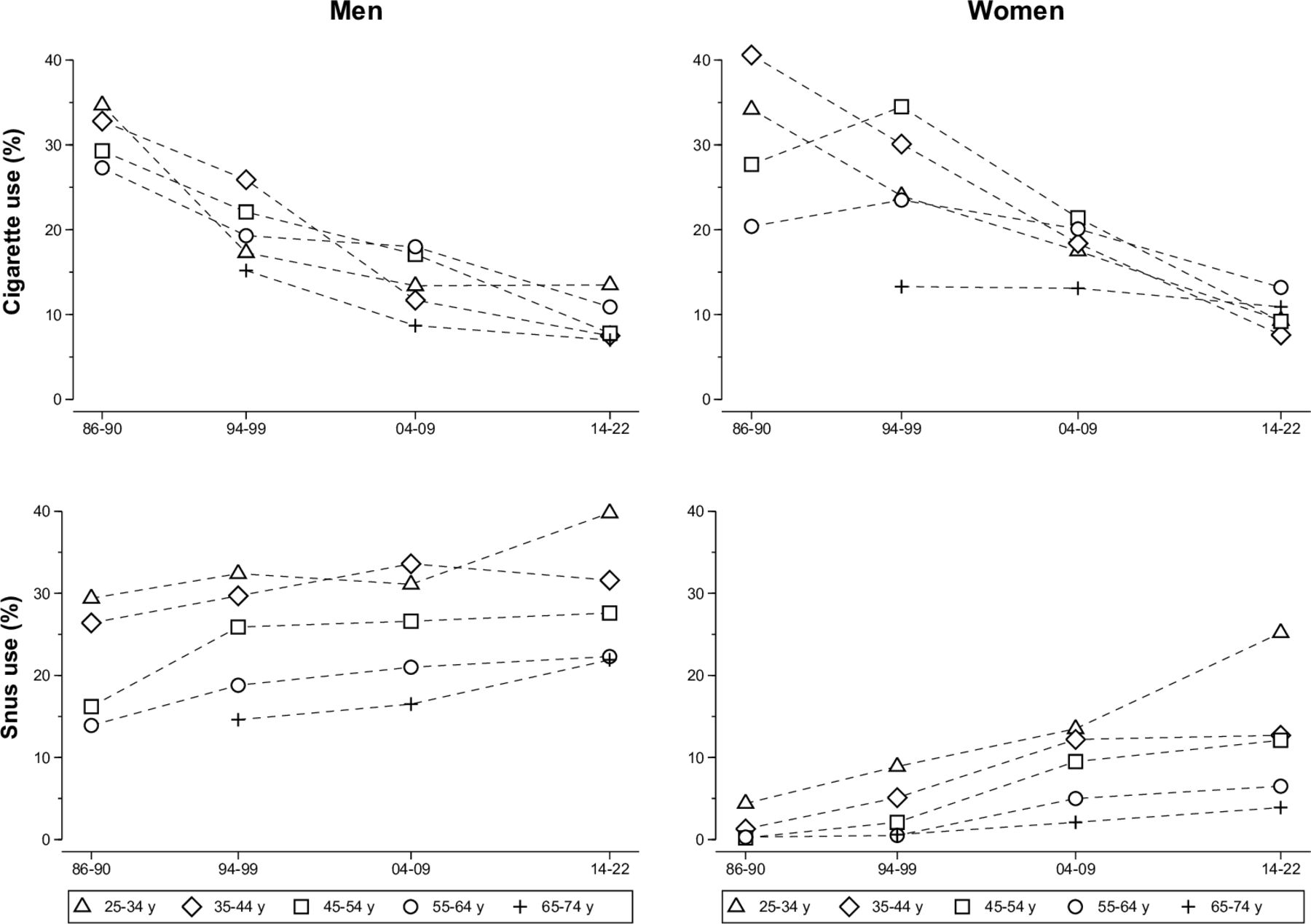
Similar trends were seen in the age-specific analyses (figure 2, tabulated in online supplemental table S4); however, there was a marked age gradient in women. As an example, women aged 25 to 34 years had decreased their cigarette use by 24.8 percentage points and increased their snus use by 20.8 percentage points between 1986 to 1990 and 2014 to 2022 (pwithin-group<0.01); the corresponding estimates in women aged 55 to 64 years were −7.2 and 6.2 percentage points (pwithin-group≤0.01). In contrast, the male trends were similar in the two age groups with decreases in cigarette smoking between 21.2 and 16.4 percentage points (pwithin-group<0.01) and increases in snus use between 10.4 and 8.3 percentage points (pwithin-group<0.01).

Percentage of tobacco use by sex and according to categories of survey year and age (1986–2022). All percentages were obtained from logit models. CIs are omitted for visual clarity.
Cigarette habits according to county of residence are shown in figure 3 (tabulated in online supplemental table S5). In general, cigarette smoking was less common in Västerbotten than in Norrbotten throughout the entire follow-up period; both prior to (1986–1994) and during (1994–2022) a cardiovascular prevention programme in Västerbotten. Among women, 35.0% smoked in Norrbotten and 22.8% smoked in Västerbotten in 1994 (pbetween-group<0.01) but the subsequent within-county decline was larger in Norrbotten, especially up until 2014, leading to percentages of 15.4% in Norrbotten and 4.5% in Västerbotten by 2022 (pwithin-group<0.01; pbetween-group<0.01). Among men, the percentage of cigarette smokers in 1994 was 25.4% in Norrbotten and 22.2% in Västerbotten (pbetween-group=0.30) but the subsequent within-county decline was larger in Västerbotten, especially from 2014 and onwards, leading to percentages of 8.6% in Norrbotten and 1.6% in Västerbotten by 2022 (pwithin-group<0.01; pbetween-group<0.01). Snus use did not differ between the counties in 2022, neither among men at 28.7 and 23.8% (pbetween-group=0.29) nor among women at 11.1 and 14.7% (pbetween-group=0.17).

{kind=link}
{kind=link}
{kind=link}
Percentage of cigarette smoking by sex in a county with (Västerbotten) and a county without (Norrbotten) a cardiovascular prevention programme (1986–2022). All estimates were obtained from logit models, adjusted for age (continuous, years) and predicted at the median age of tobacco users in the eight surveys (46.5 years). In the upper panels, dots and shaded areas represent percentages and 95% CIs in Västerbotten (dark grey) and Norrbotten (light grey). In the lower panels, dots represent percentage point change in each county compared with the survey in 1986 (prior to the prevention programme, 1986–1994) and compared with the survey in 1994 (during the prevention programme, 1994–2022) (CIs are omitted for visual clarity). Solid lines in the lower panels represent the predicted change in percentage points per year (during the prevention programme, 1994–2022), including a squared term for calendar year (to relax the linearity assumption).
The effect of potential selection bias in the 2022 survey is illustrated in online supplemental table S6, specifically with respect to regular cigarette smoking. However, a substantial change in the observed results would only have occurred if participation rates were above 80% and if regular smoking were twice as common in non-participants as in participants.
Characteristics associated with tobacco use
Details of the tobacco users in the 2022 survey are shown in table 1. Compared with non-users of each tobacco product, cigarette smokers and snus users were less educated, less often married or co-habiting, and seemed more likely to have diabetes and a higher BMI.
Demographic and health characteristics by tobacco use in 2022
Over time, cigarette smokers and snus users became more well-educated, more likely to have a higher BMI, and less likely to be married or co-habiting and to have hypertension (within-group comparisons; Online supplemental table S7). However, the cigarette smokers in later surveys were disproportionately less well-educated and less often married or co-habiting compared with the snus users and the overall study population (between-group comparisons); and they also seemed to have had a less positive development with respect to hypertension.
As shown in table 2, the cigarette smokers in later surveys were more often occasional users, smoked fewer cigarettes per day, had more often started to smoke before 18 years of age (leading to a longer duration of use) and were more likely to be current or past users of snus. With respect to snus, the users in later surveys had a longer duration of use, were more likely to consume more than four boxes per week and were less likely to be current or past users of cigarettes.
Tobacco-specific characteristics among tobacco users over time (1986–1990 vs 2014–2022)
Discussion
Brief summary of main findings
In this cross-sectional study based on the NS-MONICA cohort, we have conducted a detailed, 36-year analysis of tobacco use and its associated characteristics in northern Sweden. Over the years, the prevalence of cigarette smoking has seen a dramatic decrease and the prevalence of snus use has seen a notable increase. Contemporary tobacco use, especially of cigarettes, was associated with multiple unhealthy characteristics, such as a lower educational level and higher BMI levels.
Findings on tobacco use and in relation to other studies
A substantial decline in cigarette smoking was observed during the study period (by more than 20 percentage points in both women and men since the 1980s), leading to one in 20.4 men and one in 10.3 women smoking cigarettes by 2022. In contrast, between 1986 and 2022, the use of snus increased by 7.3 percentage points among men (with only small changes from 1999 to 2022) and by 12.5 percentage points among women, up to the point that one in 3.8 men and one in 7.7 women used snus in 2022. The female trends, but not the male trends, had a marked age gradient, exemplified by a threefold higher percentage point change of each tobacco product in younger women than in older women. Cigarette smoking was less common in Västerbotten than in Norrbotten, while snus use did not differ between the two counties.
Our findings are similar to those in other surveys, such as the Statistics on Income and Living Conditions (SILC) survey.14 In the SILC surveys in 2009, 2014 and 2022, the percentage point difference in regular cigarette smoking ranged from 0.2 to 1.8 among men and from 0.2 to 3.1 among women compared with the same survey years in the NS-MONICA cohort. The corresponding estimates for snus use ranged from 0.2 to 6.8 among men and from 0.3 to 2.8 among women. (Nota bene: A detailed comparison of the NS-MONICA study and the SILC survey is shown in online supplemental table S8).
Sweden has had a long history of various control policies to reduce the prevalence of cigarette smoking, including sales restrictions, advertisement restrictions and smoke-free environments,23 which, together with other educational and preventive measures,24 has clearly paid off and should be advocated by other countries. It is also possible that the increased use of snus has influenced the smoking prevalence, either due to a transition from cigarettes to snus over time or a choice of snus over cigarettes from the beginning. Previous studies have reported that snus is used by around one-fourth of Swedish men to assist in smoking cessation,25 26 in line with the proportion of snus users in our data who had smoked in the past. However, the use of snus as a mean to quit smoking is controversial even in Sweden, not to mention that the European Union (EU) prohibits the sale of snus products in all EU countries except Sweden, limiting its role as a smoking cessation aid in Europe.
Cigarette smoking has been—and still is—more common in Norrbotten than in Västerbotten. This finding must, at least partly, be related to the Västerbotten Intervention Programme,22 a cardiovascular prevention programme that began in 1985 and was fully implemented in 1993. All persons who turn 40, 50 and 60 years of age in Västerbotten are invited to systematic risk factor screenings and individual health and lifestyle counselling sessions. Around 48% of the NS-MONICA participants recruited between 1994 and 2022 from Västerbotten had previously taken part in the prevention programme (Veronica Hellström, Biobank Research Unit, Umeå University, personal communication, 2024). However, in our data, there were no consistent findings across the sexes that favoured the prevention programme with respect to smoking trends on the county-level—women in Västerbotten smoked less by 2022 due to a lower prevalence at the beginning of the prevention programme; men in Västerbotten smoked less by 2022 due to a larger decline during the prevention programme.
Findings on the characteristics associated with tobacco use
Modern-day cigarette smokers and snus users exhibited more characteristics associated with ill-health, such as a lower educational level, higher BMI levels and a higher probability of having diabetes, than did their non-using peers. A shift in the within-group characteristics was also seen among cigarette smokers and snus users over time, as they had higher educational and BMI levels, were less often married or co-habiting, and had less often hypertension. However, the cigarette smokers were markedly less well-educated and less often married or co-habiting than the snus users and the population at-large; they also had a less positive development with respect to hypertension. As such, especially in relative terms, a cigarette smoker can be seen as unhealthier today than he or she was 30 years ago. On the other hand, modern-day cigarette smokers were more often occasional users and had lowered their smoking intensity but not their smoking duration. In contrast, both the duration and intensity of snus use had increased over time.
Practical implications
The observed decline in cigarette smoking is extremely beneficial for public health in northern Sweden, due to the established link between cigarettes and adverse health outcomes (eg, cardiovascular disease, lung disease, diabetes and cancer).1–5 It should, however, be noted that the overall disease risk for a cigarette smoker might be greater today than it was in the past, given the co-existence with other unhealthy characteristics and a greater clustering of risk factors. A recent study also concluded that the relative importance of cigarette smoking in the development of cardiovascular diseases has increased over time, especially with respect to coronary heart disease.27 These two reasons, together with the low prevalence of cigarette smoking in northern Sweden, indicate that the time is now for a cost-effective and logistically plausible smoking cessation intervention programme on the individual level. Beyond conventional cigarettes, electronic cigarettes have become increasingly common (used by 5%–8% of 16–29-year-olds and by 0%–2% of 30–84-year-olds, according to contemporary data from the Public Health Agency of Sweden).28 Studies examining the association between electronic cigarettes and chronic diseases are limited and show inconsistent results.29 30 However, given the short-term effects of electronic cigarettes in experimental studies, including airway inflammation and obstruction, endothelial dysfunction and arterial stiffness,31 32 such exposure-outcome associations are likely to manifest in due time. Therefore, a continued monitoring of the population’s use of both conventional and electronic cigarettes is highly important.
The health effects of snus are not as well-established as the health effects of cigarettes; however, several studies have noted an association between snus use and increased risk of diabetes, overall mortality and cardiovascular mortality.7–12 A continued monitoring of the population’s snus habits is, therefore, equally important to that of its smoking habits, especially considering that snus use is now becoming very common and that even minor hazardous effects could have significant public health implications. In that regard, it is encouraging that the percentage of male snus users in the NS-MONICA study seems to have hit a plateau. Beyond conventional snus, so-called tobacco-free (nicotine) snus has become popular during the last decade, particularly among young women (used by 18% of 16–29-year-olds in 202228), and its use and health effects also need to be monitored going forward.
Strengths and limitations
The primary strength of this study was the large number of participants who were recruited at eight different occasions over a 36-year time period. Another strength was that the main questions on cigarette smoking and snus use were identical in all surveys.
A number of limitations must be mentioned. First, similar to most epidemiological studies,33 the NS-MONICA cohort has had decreasing participation rates over time (81% in 1986, 47% in 2022), questioning the representativeness of the later NS-MONICA surveys. As detailed in the supplementary material, the non-participants in the NS-MONICA study up until 2009 were more likely to be regular cigarette smokers, with non-participant-to-participant percentage point ratios of 1.15 to 1.48 in men and 1.14 to 1.54 in women. In 2022, the corresponding ratios were 0.54 in men and 1.03 in women. These two ratios should be interpreted with caution, due to the small numbers on which they were based on (around one-tenth of all non-participants), and do not exclude the possibility that non-participants in 2022 were also more likely to be regular cigarette smokers, meaning that the actual percentages in Norrbotten and Västerbotten could be higher than what we observed. However, as exemplified in our sensitivity analyses, a substantial change in the observed results would only have occurred if participation rates had been above 80% and if regular smoking had been twice as common in non-participants as in participants. Second, irrespective of participation rates, we used self-reported tobacco data, leaving the possibility of misclassification due to social desirability bias. If present, that type of bias should have affected cigarette smoking and snus use differentially over time, given that the former habit was very common and socially accepted in the first surveys and the later habit was very common and socially accepted in the last surveys. With that said, the main tobacco questions in the NS-MONICA study have been validated with good results.21 Third, the question on electronic cigarettes was only included in 2022, hindering time-trend analysis. The sampling frame is also likely to have excluded the majority of electronic cigarette users, since the NS-MONICA participants were 25 years or older. Finally, the questionnaire did not differentiate between conventional and tobacco-free snus, leading to a mixture of both types among snus users in 2014 and 2022 (which, in turn, could be a partial explanation to the marked age gradient in women).
Conclusions
A substantial decline in cigarette smoking has occurred over time in northern Sweden, particularly among men and more notably in Västerbotten. In contrast, snus use has become increasingly common in both sexes and in both counties. A continued monitoring of the population’s tobacco use is important for the public health, with the purpose to promote sustained reductions in conventional cigarette smoking without simultaneous increases in snus use (conventional and tobacco-free) or electronic cigarette use.
Data availability statement
Data are available upon reasonable request. Access to individual-level data can be provided for research purposes but is restricted by laws regarding the privacy of research participants and are, therefore, not made publicly available. Requests for data can be sent to the Section of Biobank and Registry Support at Umeå University (contact: info.brs@umu.se).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The NS-MONICA study is covered by multiple ethical approvals from the Regional Ethical Committee at Umeå University and the Swedish Ethical Review Authority (reference number: 85-19, 99-025, 03-375, 08-106M, 2013/97-31, 2020-04544, and 2021-06369-02). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the staff at the Biobank Research Unit, Umeå University, especially Robert Johansson and Veronica Hellström, for data harmonisation and data support.
References
Footnotes
SS and VO contributed equally.
Contributors Concept and design of study: ES, JA, MN, MW, LHF, CL, SS and VO; acquisition of data: SS; analysis of data: ES and VO; drafting of manuscript: ES, SS and VO; revision of manuscript: ES, JA, MN, MW, LHF, CL, SS and VO; approval of final manuscript: ES, JA, MN, MW, LHF, CL, SS and VO. SS and VO accepted full responsibility for the finished work and conduct of the study, had access to the data and controlled the decision to publish. VO acted as guarantor.
Funding The NS-MONICA study in 2022 was supported by Umeå University, the County Councils of Norrbotten and Västerbotten, the Swedish Environmental Protection Agency, and the King Gustaf V and Queen Victoria's Foundation of Freemasons. VO was supported by grants from the Norrbotten County Council.
Disclaimer The funding bodies had no role in the study design, data collection, analysis or interpretation of data, nor in the preparation of the manuscript.
Competing interests SS reports speaker’s honoraria and scientific committee participation (the EXPOSURE study), both from Janssen Pharmaceuticals (outside of the submitted work). The other authors have no conflicts of interest to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.