Article Text

Abstract
Objective To estimate the resource use of patients with obstructive hypertrophic cardiomyopathy (HCM), stratified by New York Heart Association (NYHA) class, in the English and Northern Irish healthcare systems via expert elicitation.
Design Modified Delphi framework methodology.
Setting UK HCM secondary care centres (n=24).
Participants Cardiologists who actively treated patients with HCM were eligible, of whom 10 from English and Northern Irish centres participated. Recruitment of participants to the study was limited to one expert per site.
Methods Responses were collected by electronic quantitative survey. Following the discussion of survey results in a virtual panel, aggregated responses from a final survey were analysed and stratified by NYHA class. Data were analysed without (base case) and with (scenario) interventional cardiologists who conduct septal reduction therapies (SRTs).
Results Based on expert opinion, as NYHA class increased, so did the mean±95% CI number of primary care consultations (classes I–IV: 0.64±0.35; 1.07±0.33; 3.29±1.02; 6.00±2.46, respectively) per patient per annum. This was also observed across all types of secondary care consultations, such as mean±95% CI number of cardiovascular-related outpatient visits (classes I–IV: 0.69±0.26; 0.88±0.24; 2.13±0.78; 3.25±1.42, respectively) and inpatient admissions (classes I–IV: 0.01±0.01; 0.04±0.07; 0.94±0.39; 1.90±0.65, respectively) per annum. Patients in NYHA class III were most likely to undergo SRT in their lifetime (mean±95% CI proportion of patients:17.25%±7.19% or 26.30%±13.61% including interventionalists). Across NYHA, experts estimated that septal myectomy was more costly than alcohol septal ablation (mean±95% CI: £15 675±£10 556 vs £6750±£5900, respectively). Prescription of beta-blockers was higher than calcium channel blockers, irrespective of NYHA class.
Conclusions Treatment of obstructive HCM is associated with a substantial clinical and economic burden in England and Northern Ireland; the burden of the disease increasing with NYHA class is driven by the need for intensive disease management, hospitalisations and the potential burden of undertaking SRTs.
- Cardiomyopathy
- Heart failure
- HEALTH ECONOMICS
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Bristol Myers Squibb’s policy on data sharing is available online and is located at https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The expert elicitation exercise involved 10 experts who represented (a) all cardiology subspecialties that treat patients with hypertrophic cardiomyopathy, (b) differing centre specialties and expertise and (c) diverse geographical areas within England and Northern Ireland, thus, maximising the generalisability of results.
The exercise used a modified Delphi framework methodology to capture experts’ responses in a quantitative manner, enabling data collection in a systematic, validated manner and ensuring that any potential for bias is reduced.
The final sample size was restricted due to implementation of a rule allowing for only one expert per site to limit the potential bias of large/specialist centres on the generalisability of the results.
The questionnaire underwent limited internal piloting and no external piloting; therefore, some questions may have been unclear or were differently interpreted by participants which led to variability in some responses.
The study design did now allow for investigation into the reasons for low response rates to some of the survey questions.
Introduction
Hypertrophic cardiomyopathy (HCM) is a chronic myocardial disease defined by left ventricular hypertrophy that cannot be explained by another condition.1 2 Phenotypically, HCM can be non-obstructive or obstructive; a study published in 2022 estimated that 49%–68% of patients with HCM have the obstructive subtype.3 Obstructive HCM can result in debilitating symptoms, lower quality of life and sudden cardiac death.2 4 5 Owing to the complex management of HCM, the European Society of Cardiology guidelines recommend that care is provided by specialist, multidisciplinary centres.6 Current pharmacological therapies for patients with HCM provide variable symptom relief and do not target the underlying pathophysiology of the disease.2 7 Invasive septal reduction therapies (SRTs) are also available, but there are risks associated with these interventions and access to these therapies can be limited owing to contraindications, patient preference or severity of disease.2 Additionally, SRTs in patients with obstructive HCM are associated with high costs and long hospital stays for those with postprocedural complications.8 9 Retrospective studies analysing healthcare resource use in the USA revealed that patients with diagnosed obstructive HCM were more likely to be hospitalised, have outpatient consultations and receive prescriptions than patients who had not yet received an obstructive HCM diagnosis or control patients without HCM.10 11 This ultimately resulted in patients with obstructive HCM incurring significantly higher associated medical costs on average than patients without the disease.10
The most common measure of disease severity in HCM is the four-category New York Heart Association (NYHA) Functional Classification, with class I representing no symptoms and class IV representing severe symptoms during rest.2 12 NYHA classification is routinely used by physicians to assess the symptomatic and functional capacity burden of patients with obstructive HCM and is used to guide decision-making on disease management. However, the determination of whether differences in economic burden exist between NYHA classes in patients with obstructive HCM in the UK has not previously been examined.
At the initiation of this study, no other studies had analysed the relationship between obstructive HCM disease severity and healthcare resource management in the UK. Therefore, the primary aim of this study was to estimate the healthcare resource use of patients with obstructive HCM, stratified by NYHA class, in the UK healthcare system. Additional aims were to estimate the use and economic impact of SRT and pharmacological monotherapies (beta-blockers and non-dihydropyridine calcium channel blockers) among patients with obstructive HCM in the UK by NYHA class. Given that NYHA class is not frequently documented in the UK, and owing to the time needed to access healthcare databases and develop real-world evidence studies, this study was conducted using expert elicitation of highly experienced and geographically representative participants.
Methods
Participants
Cardiologists who actively treated patients with HCM from all 24 specialist secondary care centres that are known to treat patients with obstructive HCM in the UK were eligible to participate in the study. The identity of the 24 eligible centres was established with a mapping exercise undertaken by the study sponsor. Invitations to participate in the elicitation exercise were sent to the lead practising cardiologists in each of these centres. Recipients of the invitations were allowed to refer another cardiologist in the centre to participate in the study, providing that the alternative cardiologist was actively treating patients with HCM. Diversity in the type of cardiology subspecialty was sought to ensure that the entire continuum of care for patients with HCM was represented. Experts who were involved in a different observational study related to the economic burden of obstructive HCM funded by the study sponsor were excluded from consideration; however, other experts within the same site were eligible for participation. Recruitment was also limited to one expert per site to reduce potential bias related to the size of the centre or the number of clinicians employed by a centre, and to improve the generalisability of results. Honorarium was provided to all participants for the time spent participating in the study at fair market value.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, conduct, reporting or dissemination plans of this research.
Study design
The expert elicitation exercise used a modified Delphi framework methodology. The purpose of using this well-validated methodology was to allow for the collection of data from experts regarding their experience of their local practice and the associated treatment outcomes of patients with obstructive HCM. Although the Delphi methodology is typically associated with statements which are consensus generating, this study did not explicitly require consensus. Instead, quantitative data (by overall HCM population or by health status (NYHA class)) were collected using an iterative survey-panel approach, thus enabling experts to understand the variation in treatment practice and patient resource utilisation in different centres. Thus, the study design allowed for a nationally representative assessment of resource use while also identifying variability that exists in the different participating centres. Furthermore, the methodology allowed for determination of continuous estimates for healthcare resource use and other related outcomes. As such, participants were asked to provide numerical responses to some questions on a continuous scale. This modified methodology conforms to the good practice guidelines for structured expert elicitation in healthcare decision-making.13
An economic systematic literature review of obstructive HCM was performed by the study sponsor prior to the initiation of this study and has been reported previously.14 Key findings from the review included that there was a lack of published healthcare resource use data for obstructive HCM from non-US healthcare systems and that several studies failed to report disaggregated costs and were opaque in their reporting.14 The current knowledge and evidence gaps identified as part of the review were described to participants as contextual background.
The study comprised three sequential phases: an initial electronic quantitative survey (phase I), a virtual panel discussion (phase II) and a second electronic quantitative survey (phase III) (figure 1). In phase I, undertaken in January 2022, experts were invited to complete a questionnaire that was developed in Microsoft Excel and delivered via email. The questionnaire was developed by the research partner in collaboration with the study sponsor; the study protocol was approved by the study sponsor observational protocol review committee. The questionnaire was informally piloted by a clinician employed by the study sponsor to ensure appropriateness and understanding. Minor revisions to the questionnaire were implemented following the internal piloting. All data pertaining to the pilot study were excluded from reporting of the main study. The survey included four sections: primary care consultations, secondary care consultations, tests and procedures, and other. Unless stated otherwise, responses to the questions were provided by NYHA class to determine the effect of disease severity. Experts were encouraged to provide a rationale for their answers to aid context of assessments.

Expert elicitation exercise study design. Experts were asked to complete the questionnaire remotely. The first two sections of the questionnaire focused on primary and secondary care and asked experts to estimate the number of all-cause consultations a typical patient with obstructive HCM has per annum. The tests and procedures section asked respondents to estimate the following: the number of tests that a patient with obstructive HCM undergoes per annum that are specific to HCM disease care; the proportion of patients who will receive an implantable device, SRT or cardiac rehabilitation procedure within the obstructive HCM patient population; and what proportion of patients would end up in each NYHA class after a successful SRT. The final section explored the experts’ opinions on the prevalence of obstructive HCM, use of common therapies and estimated cost of care for patients with obstructive HCM in the UK. HCM, hypertrophic cardiomyopathy; NYHA, New York Heart Association; SRT, septal reduction therapy.
Quantitative data from phase I were aggregated and summarised (and were thus anonymised) before being presented to experts to allow for a facilitated discussion of the results in phase II. The virtual panel discussion, held in early February 2022, was moderated by a senior expert in qualitative research with the third-party research partner. To minimise potential bias, research team members of the study sponsor were present at the meeting but were not allowed to actively participate. The discussion focused on questions that received highly variable responses in phase I which arose owing to various factors, including the participant’s experience, work setting or understanding of the question. Group consensus was not sought as the results were intended to reflect the variation in actual healthcare resource utilisation and costs across the participating centres, but the discussion was designed to ensure that questions were interpreted correctly. Participants could outline what their answers to specific questions were to the other experts as part of the discussion, but this was optional and was not prompted by the study team. In phase III, experts were sent a second survey and had the option to revise their responses from phase I following the panel discussion in phase II (over a 1-week period), if they wished to do so. The questionnaires circulated to participants in phase I and phase III were identical. Per Delphi methodology, only responses from phase III have been reported. To ensure anonymity, no individual data from participants are reported, and no questions regarding the characteristics of the participant’s treatment centre were collected. In addition to the quantitative responses received, key qualitative responses to questions have also been reported, where relevant.
Statistical analysis
Aggregated data from phase III were analysed in Microsoft Excel to calculate the mean, median, minimum and maximum values, and 95% CIs of the responses to each question, stratified by NYHA class. Individual responses from participants were anonymised. Descriptive statistics are reported; further statistical analyses were not conducted owing to the small sample size. Phase III data were analysed without (base case; n=8) and with (scenario; n=10) inclusion of responses from cardiologists who primarily focus on surgical interventions (ie, interventionalists). This approach was taken in order to understand the impact of interventionalists’ responses on the representativeness of the entire population of patients with HCM since surgical interventions are typically reserved for patients with advanced disease.
Results
Overall, 10 experts responded to the invitation and participated in all phases of the study (online supplemental table 1). The experts encompassed a range of cardiology subspecialties and geographical sites, and the ratio of men to women was 7:3. Participation was limited to participants at English and Northern Irish sites only, and as such, outcomes are specific to the healthcare system in England and Northern Ireland.
Supplemental material
Primary care consultations
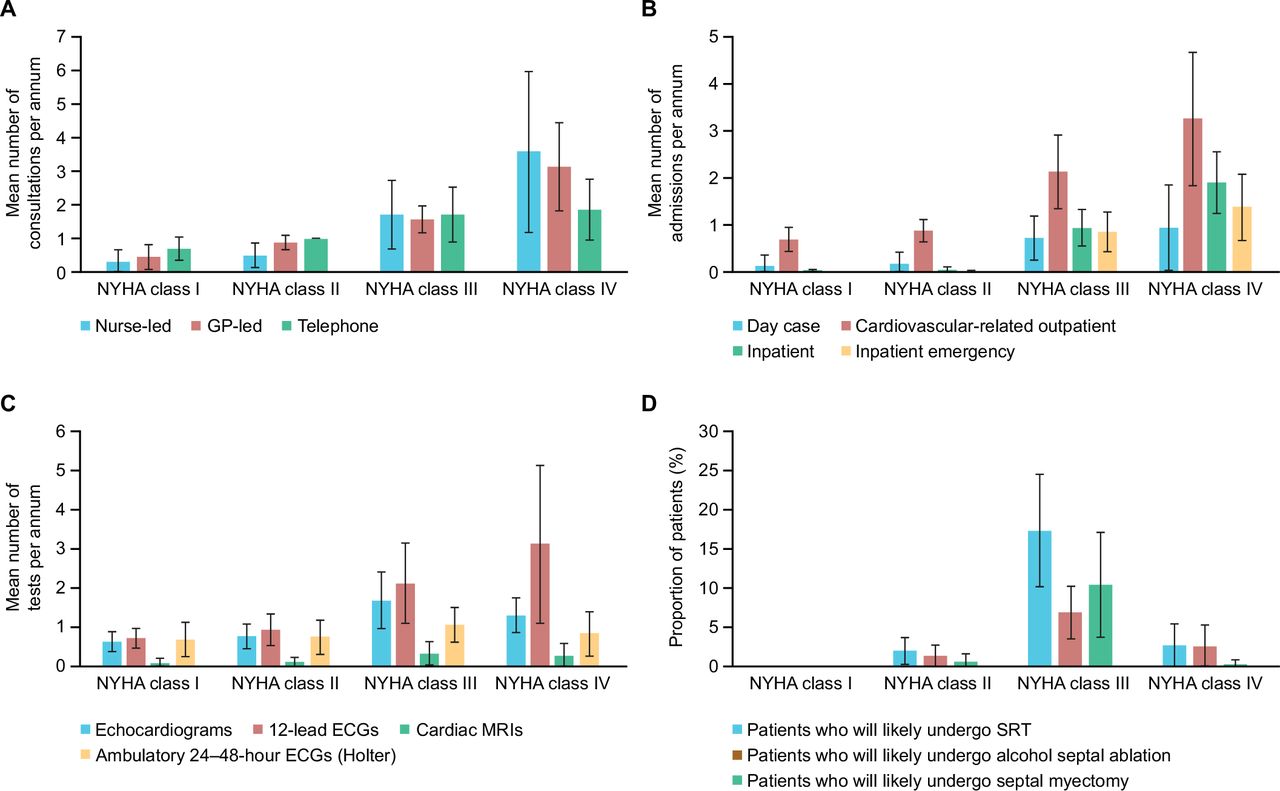
Taking into account that the experts selected were from a secondary care setting, their visibility within a non-hospital care setting was limited; therefore, some experts opted to skip questions in this section. Of the assessments received, a trend was observed between a higher NYHA class and an increasing mean±95% CI number of all primary care consultations per annum per patient with obstructive HCM (class I: 0.64±0.35; class II: 1.07±0.33; class III: 3.29±1.02; class IV: 6.00±2.46) (figure 2A and online supplemental table 2). This trend was also observed when estimating the mean±95% CI number of general practitioner-led (class I: 0.46±0.38; class II: 0.89±0.21; class III: 1.57±0.40; class IV: 3.14±1.31) and nurse-led (class I: 0.32±0.35; class II: 0.50±0.37; class III: 1.71±1.02; class IV: 3.57±2.38) consultations per annum. Some experts noted that it was difficult to estimate the number of telephone consultations per annum that a patient would have because the use of this type of service varies widely within regions of the UK; as such, there is uncertainty over the estimates provided. Results were similar irrespective of whether interventionalists’ responses were included (online supplemental table 3).

Estimated number of primary care consultations (A), secondary care consultations (B) and tests performed (C) per patient per annum, and the estimated proportion of patients who will undergo SRT* (D), stratified by NYHA class (excluding interventionalists). Data are presented as mean±95% CI. *SRT includes both alcohol septal ablation and/or myectomy. GP, general practitioner; NYHA, New York Heart Association; SRT, septal reduction therapy.
Secondary care consultations
The experts indicated that increasing NYHA class was also associated with an increase in secondary care use (figure 2B, table 1, online supplemental table 4 and online supplemental table 5). Of note, a substantial increase in the mean±95% CI number of secondary care consultations per annum by NYHA class was reported for cardiovascular-related outpatient admissions (class I: 0.69±0.26; class II: 0.88±0.24; class III: 2.13±0.78; class IV: 3.25±1.42). Although inpatient admissions per annum were estimated to be close to zero for patients in NYHA class I and class II, it was considered that this frequency would increase for patients in NYHA class III (0.94±0.39) and class IV (1.90±0.65). The mean±95% CI length of stay per inpatient emergency admission was also estimated to increase as symptoms worsened (class I: 2.50±4.90; class II: 1.00±1.13; class III: 4.57±1.65; class IV: 8.43±2.67) (table 1). Although experts believed that the number of day case admissions would be highest in patients in NYHA classes III and IV, these consultations were estimated to be infrequent irrespective of NYHA class (<1 per annum). The mean±95% CI numbers of accident and emergency department admissions were also estimated to increase, with the biggest increases observed between patients in NYHA class II (0.41±0.34) and those in NYHA classes III (1.56±0.77) and IV (2.56±0.97). The experts considered that the observed trend between higher NYHA class and increased resource use was driven by a combination of older age, greater comorbidity burden and whether symptoms were optimally controlled with treatment.
Mean±95% CI secondary care consultations by NYHA class per annum (excluding interventionalists)
Tests and procedures
When experts were asked to estimate the average number of tests performed per patient per annum, it was considered that patients with higher symptomatic burden generally underwent a greater number of tests than those with lower symptomatic burden (figure 2C). Notably, patients in NYHA class III (vs class II) were considered to more frequently undergo echocardiogram (mean±95% CI number of tests: 1.69±0.72 vs 0.78±0.32), cardiac MRI (0.34±0.29 vs 0.13±0.12) and ambulatory 24–48 hour Holter electrocardiograph tests (1.07±0.44 vs 0.76±0.44). The estimated use of cardiac implantable devices and cardiac rehabilitation procedures were similar among symptomatic NYHA classes (table 2, online supplemental tables 6 and 7). Experts agreed that this was because patients with HCM will typically be implanted with a defibrillator once they present with NYHA class II symptoms to prevent sudden cardiac death, although implantation of a pacemaker device in this patient population is not a common procedure.
Mean±95% CI tests and procedures by NYHA class (excluding interventionalists)
The mean±95% CI proportion of patients in NYHA class III estimated to likely undergo SRT (inclusive of septal myectomy and alcohol septal ablation procedures) in their lifetime was 17.25%±7.19% (figure 2D). Experts agreed that patients in this NYHA class were substantially more likely to undergo septal myectomy than those in NYHA classes I, II and IV because patients in these classes are generally not considered to be eligible for the procedure (mean±95% CI: 10.38%±6.64% vs 0%, 0.63%±0.98% and 0.29%±0.56%, respectively). However, it was noted that alcohol septal ablation, in some cases, is performed in patients in class II (1.38%±1.38%) or IV (2.57%±2.77%). As expected, the proportion of patients estimated to undergo any SRT increased after including the responses of the cardiology interventionalists in the analysis (online supplemental figure 1 and table 7). When asked to estimate what proportion of patients undergoing SRT are likely to have a complication as a result of the procedure, the experts felt that this risk was relatively low (mean±95% CI: 10.83%±8.82% for NYHA class III) and that occurrence of complications was more associated with patient comorbidities than NYHA class (table 2). Experts noted that across the overall obstructive HCM population, the likelihood of a patient undergoing an additional SRT was unlikely (mean±95% CI: 5.00%±2.15%). If an additional SRT was required, experts agreed that this was more commonly alcohol septal ablation rather than septal myectomy in patients whose disease had progressed, or their initial procedure had failed. Experts also estimated that septal myectomy was a more costly procedure than alcohol septal ablation in their centre (mean±95% CI: £15 675±£10 556 vs £6750±£5900, respectively). SRT was considered to be a mostly reliable procedure to improve NYHA class in patients. Indeed, 83.65% of patients who had NYHA class III symptoms at the time of the procedure were estimated to improve to NYHA class I or II following the procedure (figure 3A). However, it was also projected that 14.36%±6.26% of patients in NYHA class III and 44.12%±22.62% in NYHA class II would not improve class on SRT. Furthermore, 2.50%±3.35% of patients in NYHA class II and 2.00%±2.54% in NYHA class III were estimated to worsen NYHA class on SRT (2.50%±2.62% and 1.60%±2.07% when including interventionalist’s responses, respectively) (figure 3B). The expert rationale for this response was that patients who undergo SRT have a small risk of developing related conditions following the procedure, such as systolic dysfunction.

{kind=link}
{kind=link}
{kind=link}
Likely NYHA class outcome distribution of patients once they had undergone SRT in interventionalist excluded (A) and interventionalist included (B) cohorts. Values were reweighted on a single responder perspective up/down to 100%. Green cells indicate an improvement in NYHA class, orange cells indicate no improvement and red cells indicate a worsening. *CI was not relevant because the variance was 0. N/A, not available; NYHA, New York Heart Association; SRT, septal reduction therapy.
Other
Participants were asked to estimate the overall prevalence of obstructive HCM in the UK; however, almost all experts responded that they were unable to accurately estimate this rate. Regarding use of established therapies for obstructive HCM, there was general agreement among experts that beta-blocker monotherapy is more commonly used than calcium channel blocker monotherapy irrespective of NYHA class (online supplemental tables 8 and 9). However, some experts thought the mean±95% CI proportion of patients in NYHA class I who receive beta-blockers (37.50%±19.95%) was low considering its status as first-line therapy for obstructive HCM. Experts acknowledged that once a patient with obstructive HCM becomes symptomatic (NYHA class II or higher), they treat the patient as symptomatic even if the patient experiences periods of time without symptoms or functional limitations. Furthermore, some experts noted that the estimated mean proportion of patients in NYHA class IV who received beta-blockers (36.88%±27.34%) appeared to be high considering that the therapy is contraindicated in acute heart failure, and that most patients in NYHA class IV have concomitant heart failure. Regarding calcium channel blockers, it was acknowledged that their use as a monotherapy in patients in lower NYHA classes would be considered if symptoms persisted during beta-blocker monotherapy.
Discussion
Through expert elicitation of practising cardiologists, this exercise revealed that differences in healthcare resource use in England and Northern Ireland are most prominent between patients with obstructive HCM in the lower NYHA classes (I and II) and those in NYHA classes III and IV. The biggest increases were observed between class II and III, and between class III and IV, indicating a potential strategic focus on reducing the symptomatic burden in those with class III and class IV symptoms to reduce the resource utilisation of these patients.
In particular, the expert opinion was that an increase in NYHA class was associated with a greater number of both primary and secondary care consultations per annum, with the highest resource use consistently observed for patients with class IV symptoms. In addition to a higher number of consultations, compared with patients in lower NYHA classes, patients in higher NYHA classes were estimated to have a longer average length of stay per admission to inpatient care; those patients will have had a higher frequency of emergency care and coronary care visits, a higher dependency and an incrementally higher use of intensive care units. Patients in higher NYHA classes were also estimated to require a greater number of annual tests than patients in lower NYHA classes. Patients in NYHA class III were considered most likely to undergo SRT, irrespective of inclusion of interventionalists’ responses. Although considered to be an effective procedure to improve patient NYHA class, the expert opinion was that SRT (particularly septal myectomy) was costly to perform. The responses from experts regarding the treatment landscape of obstructive HCM revealed that patients predominantly receive beta-blocker therapy over calcium channel blocker monotherapy irrespective of NYHA class.
At the time of undertaking, this study was the first to quantify the burden of obstructive HCM on the English and Northern Irish healthcare systems. A key strength of this study is the participation of cardiology experts from 10 different centres across England and Northern Ireland that encompass a breadth of cardiovascular expertise, from centres that specialise in the treatment of obstructive HCM. Another strength of this study relates to the use of a modified Delphi methodology to produce a quantitative data set based on experts’ opinions. The modified methodology also ensured that any response bias that arose from the influence of prominent experts’ opinions was minimal because individual feedback was anonymised during the two rounds of questionnaires. However, the findings of the study should be interpreted in the context of various limitations. The design of the phase III questionnaire meant that it was not possible to ascertain the reason why some questions had low response rates, although questions pertaining to the lack of response to certain questions in phase I were explored in phase II. Potential reasons include some experts believing that it was not applicable to their practice, or not knowing the answer. For example, some experts expressed difficulty in providing accurate answers for the primary care consultations section and for questions that required estimating the proportion of patients who received implantable devices or underwent SRT because they were not aware of how many patients of each NYHA class there were in their clinic. Experts also noted that it was challenging to estimate the average number of tests performed per annum for patients with obstructive HCM specifically, because they often have no need to subgroup by type of HCM during the course of a clinical visit. The questionnaire was informally piloted by one clinician employed by the study sponsor and was not piloted externally. It is possible that this led to differing interpretations from the participants regarding what information was intended to be elicited from questions, which led to the variability observed in some responses. Although efforts were made to recruit experts from a wide range of cardiovascular subspecialties to participate in the study, those who did participate, which were less than half of those who were invited, may not accurately reflect the broader population of practising cardiologists who care for patients with obstructive HCM in the UK. The results of the study may also be transiently relevant given potential future changes in clinical practice when treating patients in specific NYHA classes. Therefore, although the elicitation exercise has been informative to elucidate expert opinion on this topic, further studies using real-world evidence are required to validate the findings.
Obstructive HCM is associated with a substantial clinical and economic burden; one study of US insurance claims data determined that patients with obstructive HCM had significantly more all-cause hospitalisations, days in hospital and outpatient visits than matched control patients who did not have the disease. Ultimately, healthcare costs for symptomatic patients with obstructive HCM were estimated to be approximately US$35 000/year higher than those of the matched controls.11 The association of high NYHA class with an increased risk of hospitalisation is well established in patients with heart failure,15–18 yet, until the findings of this study, evidence that supported a similar relationship in patients with obstructive HCM was limited. The results of this exercise suggest that patients with obstructive HCM in NYHA classes III or IV are admitted more frequently and spend longer in care than those who are asymptomatic or who have mild symptoms. However, the experts acknowledged that the number of secondary care consultations per patient can vary greatly depending on the patient’s comorbidities, age and type of treatment. The observation that patients in NYHA classes III and IV require a greater number of tests than those in NYHA classes I and II was consistent with the findings of the accompanying economic analysis of this study, which determined that higher NYHA classes were associated with greater mean healthcare costs per patient-year than lower NYHA classes, ranging from £771 for patients in NYHA class I to £14 483 for patients in NYHA class IV.19 However, owing to the severity of symptoms associated with NYHA class IV, experts in this study noted that patients in this class predominantly receive supportive care and, therefore, some diagnostic tests would be unnecessary (eg, ECGs) or potentially dangerous (eg, stress-induced echocardiograms, cardiopulmonary exercise testing).
In agreement with guideline recommendations,1 2 experts estimated that patients with obstructive HCM are almost exclusively referred for SRT if they have NYHA class III symptoms (compared with other NYHA classes), although as a relatively low proportion of the total patients in the class. This finding corresponds with experts estimating that patients in NYHA class III would also have the highest average number of cardiac MRI and cardiopulmonary exercise tests per annum because these tests are routinely performed to guide structural intervention in patients with obstructive HCM.1 20–22 The generally low estimated use of SRT across NYHA classes was thought to be because of contraindications for the procedure or patients expressing a preference for not undergoing the procedure. Although experts noted SRT to be an efficacious procedure, they also estimated that it would not guarantee an improvement in NYHA class and, in some cases, would result in complication or a worsening of NYHA class, or would require the patient to have a repeat SRT.
Despite beta-blockers and calcium channel blockers being guideline-recommended therapies for obstructive HCM, evidence supporting the effectiveness of these agents in reducing the need for invasive procedures in severely symptomatic patients is limited. Consistent with previous studies, it was noted by the experts that patients are often switched between therapies owing to treatment intolerance,23–25 thus further increasing healthcare costs.
Conclusion
In summary, a modified Delphi structured expert elicitation of leading practising cardiologists in England and Northern Ireland revealed a trend towards an increased number of primary and secondary care consultations, a longer length of inpatient admissions and a greater proportion of invasive interventions for patients in higher NYHA classes compared with those who are asymptomatic or who have mild symptoms. Therefore, reducing the symptomatic burden on patients with obstructive HCM, specifically those in class III and IV, may have a substantial impact on healthcare system resource use in England and Northern Ireland.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. Bristol Myers Squibb’s policy on data sharing is available online and is located at https://www.bms.com/researchers-and-partners/clinical-trials-and-research/disclosure-commitment.html.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval of the study from a national committee was not required because no prospective collection of patient-level data was performed. The study protocol was reviewed by an independent protocol review committee of the study sponsor which granted ethical approval on 10 January 2022, with an amendment approved on 18 January 2022. The study protocol was not prospectively registered on a data platform.
Acknowledgments
The authors would like to thank the participants who made this study possible and the following contributors: Elliot Rosen of Accession Healthcare Consulting Ltd for moderating the virtual panel meeting, Elizabeth Molenkamp of Accession Healthcare Consulting Ltd for providing subject matter expertise, Susannah Jackson of Accession Healthcare Consulting Ltdf for providing administrative support and Peter Magnusson of Bristol Myers Squibb for providing clinical support in question development. Writing and editorial assistance was provided by Thomas Crighton, PhD, of Oxford PharmaGenesis, Oxford, UK, funded by Bristol Myers Squibb.
References
Footnotes
Contributors MH, CZ, TK, BS and DA collected and analysed the data. MH, CZ, TK, BS, TL, KN, DA and FO interpreted the data; contributed to manuscript development; critically revised the manuscript for important intellectual content and approved the final version. MH is responsible for the overall content as guarantor. TK and DA at the time the study was conducted.
Funding This study was supported by Bristol Myers Squibb.
Competing interests Since the study was conducted, Bristol Myers Squibb launched mavacamten, a cardiac myosin inhibitor indicated for the treatment of adult patients with symptomatic NYHA class II–III obstructive HCM, in the UK (Medicines and Healthcare Products Regulatory Agency approval date: July 2023). The study did not include any materials or discussions relating to mavacamten or cardiac myosin inhibitors and was intended to understand the resource use associated with obstructive HCM before the introduction of such treatments in the UK. The study chair (employed by Accession Healthcare Consulting Ltd) did not form part of the study team. The competing interests of the study chair were relayed to the participants during the phase II panel discussion. Competing interest information was collected as part of involvement in the study; however, they were not applicable owing to there being no discussion of patented therapies. MH, BS, TL and KN are employees of Bristol Myers Squibb and may own stock in Bristol Myers Squibb. CZ is a contractor for Bristol Myers Squibb. TK was an employee of Bristol Myers Squibb at the time the study was conducted and may own stock in Bristol Myers Squibb. DA was an employee of Accession Healthcare Consulting Ltd at the time that the study was conducted, which received payment from Bristol Myers Squibb for participation in this study. FO has no conflicts of interest to disclose.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.