Article Text

Abstract
Objectives Among nurse leaders, gender should receive particular attention, because life and work experiences and burnout during COVID-19 pandemic may vary between women and men, potentially requiring different strategies to achieve well-being. Thus, information about gender differences in burnout might be critical to burnout prevention in nurse leaders. Additionally, there has been a substantial call for attention to gender during the COVID-19 pandemic, reflecting a concern that responses to the pandemic that fail to consider gender differences and norms will be ineffective. Therefore, the objective of the current study is to examine personal burnout, client burnout and work-related burnout of nurse leaders while considering the impact of COVID-19 pandemic and work-life balance through a gender lens.
Design A cross-sectional study design was implemented in 2023 using a convenience sampling approach.
Setting Data on personal burnout, work-related burnout, client burnout, work-life balance and COVID-19 impact were collected electronically and assessed through a gender lens.
Participants A sample of 210 nurse leaders filled out the online surveys that were posted on the American Organization for Nursing Leadership and on Facebook.
Conclusion Females had significantly higher personal burnout than males (mean 56.2 vs 49.3, F=5.853, p=0.019). Males had significantly higher client-related burnout than females (mean 45.3 vs 34.8, F=7.014, p=0.008). Findings demonstrate the importance of addressing gender when examining how nurse leaders react to different factors leading to burnout. In employing a gender lens framework, future researchers might study how the pressures that working men and women nurse leaders face were intensified during the COVID-19 pandemic. To support nurse leaders in executing their roles, there is a need to widen the scope of conversations about including family-friendly policies and attention to the needs of men and women as nurse leaders. These policies might include but are not limited to paid childcare, flexible time off, access to paid time off and mandatory overtime laws.
- COVID-19
- Burnout, Professional
- Burnout
- Cross-Sectional Studies
- Administration
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The use of a validated instrument with a clear operational definition makes it possible to compare research results.
Posting the participation link on a professional organisation page and on Facebook page reduced the risk of selection bias.
The cross-sectional design does not allow causal relationships to be determined.
Unequal sample sizes might decrease the power to detect differences across the groups.
Background
Nurse leaders in healthcare settings play an integral role in supporting the work of nurses while ensuring safety and quality care is provided to patients.1 Nurse leaders represent a workforce of 169 795 registered nurses throughout the USA.2 For this research, a nurse leader was defined as a person who held a role as an assistant manager, manager, director or vice president with oversight over patient care and served in a supervisory role. Nurse leaders report increasing levels of burnout due to increasing occupational stressors.3 The effect of the stressful role of nursing leadership on nurse leaders is now compounded by the impact of COVID-19 yielding more incidents of burnout among nurse leaders.4 Nurse leaders need to pay close attention to their well-being by understanding what leads to burnout. By controlling the impact of burnout on nurse leaders, healthcare organisations may be able to retain more nurse leaders and stabilise the care environments for patients. Burnout is defined as the attribution of fatigue and exhaustion.5 Approximately, 30% of nurse leaders leave their positions due to burnout.6
In order to expand the research on job burnout among, the current study examined both individual and situational predictors of job burnout among a sample of nurse leaders. Burnout can be studied on two different levels: the individual level (who is more likely to experience burnout) and the situational level (where burnout occurs).7 Gender as a demographic variable can have an impact on burnout and stress.7 Situational characteristics such as work-life balance and COVID-19 impact have also been identified to contribute to job burnout among nurse managers.6 8 The existing literature has identified multiple sources of burnout among nurse leaders, but studies have rarely combined contextual and personal factors. Cano-García et al 9 confirmed that the combination of personal and contextual variables could significantly predict job burnout. Therefore, this study analysed burnout of nurse leaders based on the transactional model of job-stress and burnout,10 which extensively studies job stress and burnout. The model indicates that interaction between the personal and contextual variables determines whether the situation puts pressure on the individual. Therefore, burnout can be interpreted as a result of the interaction between triggering contextual and personal variables. Individual factors refer to individual differences or personal characteristics that are relatively stable over situations and time.11
Gender as an individual factor is conceptualised as one of the core social determinants of population health within the social determinants of health (SDH) framework of the WHO.12 Together with other SDH, gender shapes health outcomes through the differential exposure to intermediary determinants of health, that is, psychosocial (stressors).13 There has been a particular emphasis on gender-based issues with regard to human resources in the global health workforce in recent years.12 Among nurse leaders, gender should receive particular attention, because life and work experiences and burnout during COVID-19 may vary between women and men potentially requiring different strategies to achieve well-being. Therefore, examining how nurse leaders experience burnout through a gender lens during COVID-19 may highlight differences between male and female nurse leaders, the needs of working men and women nurse leaders, and policy implications that may otherwise be overlooked. Research on burnout among nurse leaders during COVID-19 focused on other factors than gender.6 8 9 Additionally, despite there being research considering the issue of work-family interferences as a relevant factor to burnout among nurse leaders,6 there is still no clear consensus on whether perceived levels of work-life balance and its effects on nurse leader burnout may vary between male and female nurse leaders during COVID-19. Gender identity in this context is defined according to the CDC,14 which defines gender as an individual’s biological status as male, female or non-gender conforming. The connection between work and life and the topic of work-life balance is gaining significant interest among researchers.15 In the context of nursing leadership and management, there is evidence that women who become nurse leaders are more likely to be single and not responsible for the care of children.16 This implies that women with family responsibilities are disadvantaged when aspiring to leadership positions, which is supported by evidence that women consider family responsibilities a barrier to career progression.16 In a clinical vignette, Dr Smith as a healthcare worker and a mother of two children continued to feel disillusioned regarding her hopes of moving into leadership.17 Dr Smith struggles with managing her many roles of mom, wife and job duties which left her more prone to stress because of needing to ‘prove herself constantly’ to the men in her department.17 Thus, in studies of job burnout, it is important to consider how the burden of domestic responsibilities can intertwine and even disrupt paid work.18 A study found that being a mother with small children was associated with emotional exhaustion among nurses who are not leaders.19 On the other hand, other studies found that even though male nurses are more likely to be in senior roles than their female counterparts,20 male nurses were more likely to leave the profession than females.21 A better understanding of these issues by exploring the differences in burnout between male and female nurse leaders will benefit healthcare systems to alleviate workforce shortages.
Haar and Brougham22 identified work-life balance as one of the main factors that decrease stress among individuals. One of the factors that affect work-life balance is environmental factors, such as government policies and globalisation.23 The environmental factors had a drastic change after the COVID-19 pandemic started in December 2019, affecting millions worldwide.24 Subsequently, the governments-imposed measures to minimise the spread of the virus, such as lockdowns, the closing of organisations and social distancing regulations until vaccines were available.25 Increased uncertainty makes nurse leaders face the work-life issue while trying to fulfil their work requirements.26 Nurse leaders have responsibility for nursing quality and safety by which they often carry their work home causing poor work-life balance.27 Researchers have considered work-life balance among nurse leaders to be a significant issue, leading to stress28 and burnout.6 Considering the interest in effectively promoting work-family balance and well-being among nurse leaders, this study was to identify COVID-19 impact as a factor that may intervene in this association, overwhelming the negative effects of work-life balance on male and female nurse leaders’ psychological well-being. COVID-19 impact was considered as a covariate in our current study and was predicted to affect the study findings. Thus, information about gender differences in burnout while considering the impact of work-life balance between them might be critical to burnout prevention in nurse leaders. Work-life balance in this study is defined as an individual’s subjective appraisal of the accord between their work and non-work activities.29 Guided by the hypothesised model in figure 1, the purpose of this study is to determine whether the gender of nurse leaders has an impact on burnout while controlling for the effect of work-life balance and COVID-19 by testing the following hypothesis: There will be a difference in the burnout of female and male nurse leaders while controlling for work-life balance impact and COVID-19 impact.

Conceptual model.
Relevance to the American Organization of Nurse Leadership
American Organization for Nursing Leadership (AONL) is the voice of US nursing leadership. By establishing information and baseline characteristics for this occupational population, the study was aligned with AONL strategic priority 1:3 lead, influence and support the healthcare workforce and advance nursing leadership.30 This study looked at burnout in nurse leaders from a new perspective. Male and female nurse leaders can then be attuned to which degree they are susceptible to burnout, during times of crises such as the pandemic of COVID-19, while ensuring a good balance between work and life. Additionally, employing a gender lens framework may shed the light on meaningful conversations on the role of gender in the daily practices of nurse leaders and on how the pressures that working men and women nurse leaders face were intensified during the COVID-19 pandemic. These might widen the scope of conversations to include family-friendly policies and attention to the needs of women and men as nurse leaders.
Methods
Design and setting
A descriptive cross-sectional study design was used to determine if burnout among nurse leaders differs based on gender. The target population was nurse leaders in the USA. Convenience sampling method allowed for online recruitment of volunteers from across the USA. Selection was based on respondent availability. Recruitment and data collection occurred between November 2022 and February 2023. Based on computing statistical power analysis using G*Power, the target sample size was 128, which was based on detecting a large effect size (0.25)31 for gender and burnout variables, alpha=0.05 and power=0.80. After accounting for attrition, 143 respondents needed to be included in this study.
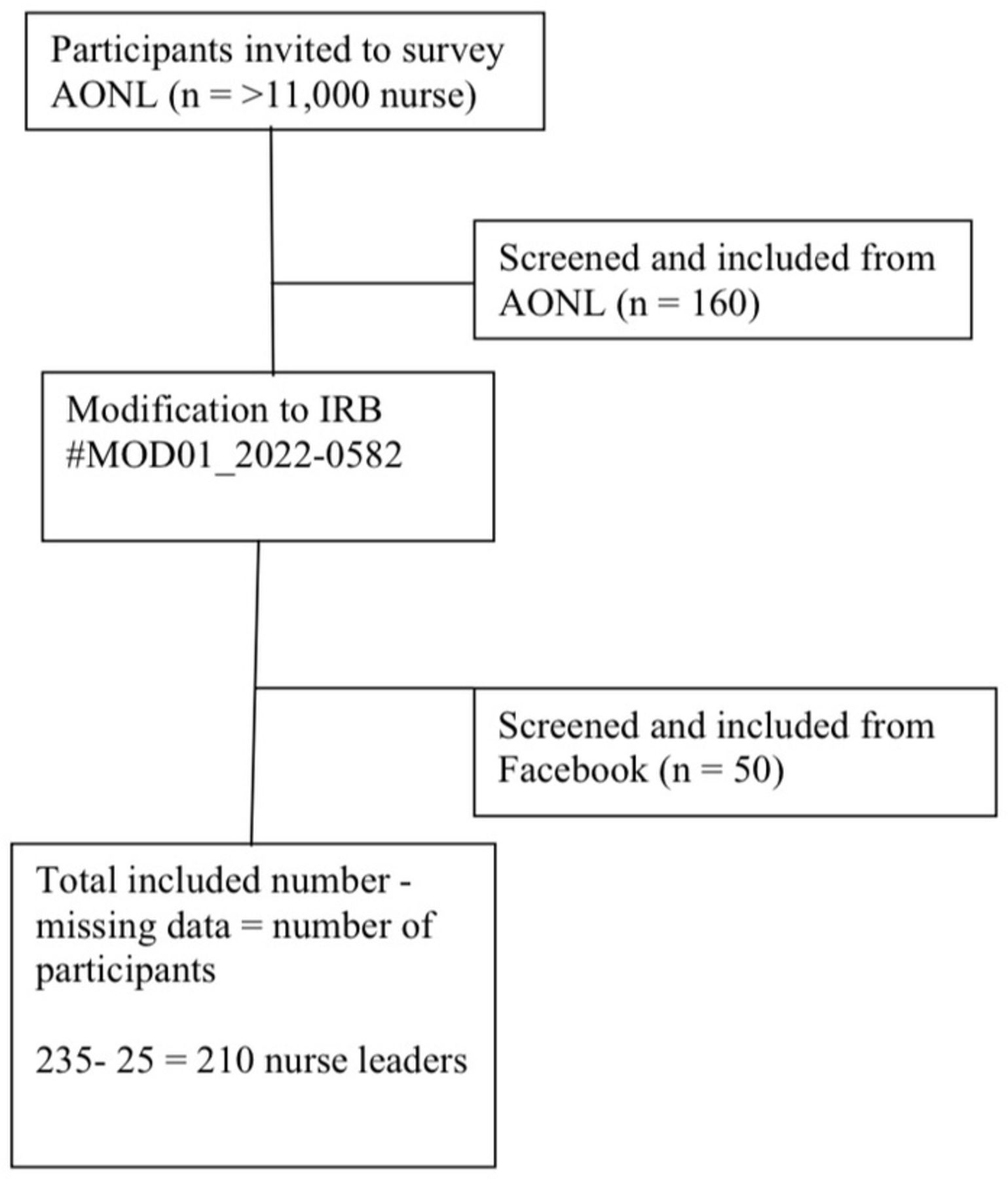
Several methods were used for study recruitment. First, members of AONL (>11 000 nurse leaders) were invited to participate through the AONL weekly e-newsletter. Second, an invitation was sent to nurse leaders on the AONL Leader2Leader Community forum. Finally, a survey link for the study was posted on the AONL webpage (https://www.aonl.org/research).
To reach the projected number of study participants, a modification to the IRB was made to be able to recruit study participants from the Kentucky Organization of Nurse Leaders Facebook page (297 members). The link was distributed on both sites only once. During the recruitment phase, a screening instrument was created to determine whether a prospective respondent fits the study’s eligibility criteria. Inclusion criteria was for those who have at least a diploma or an associate degree and worked at least 6 months in the hospital as a nurse leader, director, manager, assistant manager or a charge nurse. Nurse leaders with less than 6 months in the leadership position were excluded from the study. Other respondents who were not identified as nurse leaders and work outside the USA were excluded from the study. When accessing the link, the participants were provided with an information letter as a component of informed consent. All data was collected confidentially, then entered directly into REDCap by respondents. Only research investigators were able to access data and responses were kept confidential and not linked to their email addresses to prevent matching. The data was then screened for missing data and cleaned through running missing value analysis. There were 25 respondents with missing data, that is more than 10% at random; those cases were deleted. The remaining respondents answered all items. Because of this, missing variables were not imputed.
Participants
The analytical sample size consisted of 210 respondents each was provided a $10 Amazon eGift Card. The completion time for participants was estimated to be less than 15 min. The actual completion time averaged 7 min. There was no report of adverse events resulting from participation in the study. Posting the participation link on a professional organisation page and on Facebook page reduced the risk of selection bias. This provided the opportunity for nursing professionals to participate from across the country. The same research link was provided on all sites with the request for participation in the study. See flowchart of subject’s enrolment in figure 2.

{kind=link}
{kind=link}
Flowchart of subject’s enrolment. AONL, American Organization for Nursing Leadership.
Instrumentations
The respondents completed four questionnaires: demographic questionnaire, Copenhagen Burnout Inventory (CBI), COVID-19 scale and Work-Life Balance Questionnaire. The CBI consists of 19 items that measure three dimensions of burnout: Personal (PB, six items), Work-related (WB, seven items) and Client-related (CB, six items) burnout.5 PB measures the overall burnout unrelated to one’s job. WB and CB measure burnout as related to one’s work and their work with clients (or colleagues). The CBI has evidence of face validity based on its wide usage as a measure of burnout and the utilisation of its aspects in the assessments of relatively focal aspects of the constructs.32 Cronbach’s alphas were assessed and found to be excellent for PB, WB and CB: 0.91, 0.89 and 0.92, respectively.33 In this study, the CBI was scored with the original answering options, which were then re-coded into the original format labels of 100 (always/to a very high degree), 75, 50, 25 and 0 (never/almost never, or to a very low degree).5 Each subquestion is assessed on a Likert scale with five levels ranging from 0 to 100 in increments of 25. The total scale score consists of the average score of the items in each subscale.
Work-life balance as a covariate, was measured using a 4-item work-life balance scale developed by Brough et al.29 Participants were asked to rate their level of agreement with statements related to work-life balance. Responses were marked on a 5-point Likert scale ranging from 1=strongly disagree to 5=strongly agree. The scores of the four items were summed to create a total score reflecting the level of work-life balance. Brough et al 29 tested the work-life balance scale on four different samples and reported a Cronbach alpha value ranging from 0.84 to 0.94, demonstrating sound psychometric properties. COVID-19 outbreak impact was measured using a scale ranging from 0 (no impact) to 10 (significant impact) with a single question: ‘How affected was your practice by the COVID-19 pandemic?’.34 Demographic items included questions about age, gender, educational attainment, years of experience and leadership position type. No Cronbach’s alpha of this question was reported.
Human subjects protections
Using an information sheet for research, each respondent was informed of the purpose of the study, the estimated time required to complete the surveys and their right to withdraw without penalty. Data were collected confidentially and entered directly into REDCap by respondents. Participants’ emails were kept private and stored separately from the data in REDCap to prevent matching.
Data analysis
The data were first screened for missing data and cleaned by running a missing value analysis. There were 25 respondents with missing data, more than 10% at random; those cases were deleted. The remaining respondents answered all items. Because of this, missing variables were not imputed. Variables then were screened for outliers and normality, and the modelling type of the variables also was corrected. Histograms showed a visual clue that the data were likely normally distributed. Descriptive statistics (eg, frequencies, percentages) were used to describe the characteristics of the study sample. Continuous variables (ie, personal burnout, work-related burnout, client burnout, work-life balance and COVID-19 impact) were assessed in relation to gender using analysis of covariance (ANCOVA).
COVID-19 impact, and work-life balance scores were assessed as continuous covariates that could affect the findings of this current study. Researchers identified work-life balance as one of the main factors that have psychological impacts on individuals22 and work-life balance can be influenced by environmental factors.23 Many environmental factors related to COVID-19, such as social distancing regulations, have increased uncertainty among nurse leaders while trying to balance their work and life activities.26 Continuous variables along with gender as a categorical variable were put together to evaluate ANCOVA assumptions (normality, homogeneity of variance within groups, linear relationship between covariates and the dependent variable, and homogeneity of covariate effect across the groups) was carried out by visual inspection of the variables. Three different ANCOVA models were performed for personal burnout, client-related burnout and work-related burnout to compare mean scores for female and male nurse leaders while controlling for the influence of work-life balance and COVID-19 impact. The items within each scale and subscale were averaged. Alpha was set at 0.05. Analyses were completed using JMP-pro16.
Results
The analytical sample size consisted of 210 respondents. Table 1 shows the demographic characteristics of the sample. Descriptive statistics (eg, frequencies, percentages) were used to describe the characteristics of the study sample. Most of the participants were female nurse leaders (n=167, 80%). Even though having unequal sample sizes might decrease the power to detect differences across the groups, other means were tried to enhance the statistical power of the study such as using a precise and accurate measurement tool. The questions on burnout have been validated and used with nurse managers.35 The use of a validated instrument with a clear operational definition5 makes it possible to compare research results. Investigating gender differences in burnout among nurse leaders is still necessary even though we did not have exactly equal sample sizes. Talking about the distribution of male and female nurse leaders across the USA would maybe support this importance. Based on articles published within the 5 years preceding data collection, it was anticipated that there would be 20% male and 80% female leaders within the AONL.36 Additionally, Zippia2 estimated that there were 86.5% women and 13.5% men nurse managers in the USA. Researchers anticipated the probability of a man achieving one of the management positions in hospitals to be 3.85 times higher than that of a woman.37 Even though male nurses are more likely to be in senior roles than their female counterparts,20 male nurses were more likely to leave the profession than females.21 This might explain the discrepancy in sample sizes between the two demographic groups. Exploring the differences in burnout between male and female nurse leaders will benefit healthcare systems to alleviate workforce shortages.
Characteristics of the study sample
Results of the current study showed that the mean age of respondents was 43.6 years (range 25–78 years). The mean number of years as a nurse leader was 5.5 (range 0.1–23 years) and the main area of work was in the hospital. Most participants had a diploma/associate degree (27%) or a master’s degree (36%). As a function of male and female, the mean age of males was 40.4 with an SD of 12.4 and the mean age of females was 44 with an SD of 12.0. The mean length of experience for males was 6.2 with an SD of 4.0 and the mean length of experience for females was 5.2 with an SD of 4.1. Most male participants had a diploma/associate degree (13.3%) and most female participants had a master’s degree (30.9%). Variables were screened for outliers and normality, and modelling type of the variables also was corrected. The histogram shapes showed a visual clue that the data is likely to be from a normal distribution. Descriptive statistics (eg, mean, SD) were used to describe each continuous variable. The average PB score was 54.8 (SD=15.6), WB score was 53.0 (SD=14.8) and CB score was 37.0 (SD=19.2). The average of work-life balance scores was 2.9 (SD=0.6), and the average of COVID-19 impact scores was 6.9 (SD=2.8).
The evaluation of the ANCOVA assumptions (normality, homogeneity of variance within groups, linear relationship between covariates and the dependent variable and homogeneity of covariate effect across the groups) was carried out by visual inspection of the variables. Continuous variables (ie, personal burnout, work-related burnout, client burnout, work-life balance and COVID-19 impact) were assessed in relation to gender using ANCOVA. Three ANCOVA models were performed for personal burnout as the first dependent variable in the first model, client burnout as a dependent variable in the second model and work-related burnout as a dependent variable in the third model. We controlled COVID-19 impact and work-life balance as covariates in all three models. Results showed that female nurse leaders had significantly higher personal burnout levels compared with male nurse leaders (56.2 vs 49.3, p=0.019). Male nurse leaders had significantly higher client burnout scores compared with female nurse leaders (45.3 vs 34.8, p=0.008). There was no significant difference in work-related burnout levels between male and female respondents (F=0.845, p=0.359). Table 2 shows a comparison of burnout subscales, COVID-19 scores and work-life balance scale by gender.
Comparison of personal burnout, client-related burnout and work-related burnout in the investigated subgroups
Discussion
Based on the transactional model of job-stress and burnout,10 which extensively studies job stress and burnout, this study analysed the burnout of nurse leaders. The model indicates that the interaction between the personal and contextual variables determines whether the situation puts pressure on the individual. Therefore, burnout can be interpreted as a result of interaction between triggering contextual and personal variables. This study contributes to our understanding of how gender affects burnout using CBI subscales among nurse leaders. In general, the results of this study indicated that female and male nurse leaders experience client-related and personal burnout differently. No significant differences were found between female and male nurse leaders based on work-related burnout. Studies that used CBI to measure burnout among nurse leaders did not re-address gender differences in nurse leaders.38 39 Literature from the current COVID-19 pandemic points to the importance of using a gender lens when examining experiences.40 While there is still much to be done to redress gender differences in nursing management and leadership, the signs are that progress is made especially in South Africa.41 Gender analysis in relation to psychological outcomes among nurses also was examined,42 but nothing was specific to nurse leaders during COVID-19. Higher rates of post-traumatic stress symptoms were reported by female healthcare workers in China43 and certain groups of female healthcare workers in Italy during the COVID-19 pandemic.44 Despite these findings, a lack of literature exists about differences in nurse leaders’ gender as a demographic factor in burnout among US nurse leaders during COVID-19.
In the current study, we found that female nurse leaders had significantly higher personal burnout levels compared with male nurse leaders (56.2 vs 49.3, p=0.019) while controlling for the effect of COVID-19 and work-life balance. Personal burnout was defined as psychological and physical exhaustion related to one’s own personal life.5 In studies of job burnout, it is important to consider how the burden of domestic responsibilities can intertwine and even disrupt paid work.18 A study found that being a mother with small children was considered as a factor associated with emotional exhaustion among nurses who are not leaders during COVID-19.19 Referring to studies that explored gender differences in occupational health processes by enrolling different working populations inclusive of nursing, the higher incidence of psychophysical disease among women workers is well-established.45 Other study findings suggested that female nurses who are not leaders appear to perceive demands, strain, and time devoted to work as interfering with their ability to deal with family responsibilities to a greater extent than male coworkers.42
In our current study, we also found that male nurse leaders had significantly higher client burnout scores compared with female nurse leaders (45.3 vs 34.8, p=0.008) while controlling for the effect of COVID-19 and work-life balance. The term, ‘client’, used in the CBI was not specific in the distributed questionnaires. For future research, it would be interesting to know how male nurse leaders define the term ‘clients’ and use that definition in place of the term ‘client’. For example, if male nurse leaders define clients as employees, future research could determine how their burnout response differs using this category of clients which might be critical to burnout prevention in male nurse leaders. This is important because burnout produces turnover and poor job satisfaction and focusing on the well-being of male nurse leaders is imperative. For both demographic groups education and preparation to achieve a high level of personal and professional competence are needed to provide nurse care in disaster situations.46 Other researchers suggested that the development of emotional intelligence skills during workplace education programmes can lead to the development of self-efficacy and help to retain administrative personnel.47
The results of the current study showed a significant effect of participant work-life balance as a covariate on personal burnout, defined as personal psychological and physical exhaustion.5 This finding confirms previous findings that in situations where medical needs rapidly emerge, nurse leaders experience challenges associated with COVID-19,48 while also finding it difficult to reconcile work and family life.49 Researchers suggested that family caregivers who have familial responsibilities experience various challenges and worries for their loved one’s physical and mental well-being.50
The results of this current study also showed a significant effect of COVID-19 as a covariate on client burnout, the psychological and physical exhaustion related to working with employees. In a phenomenological study, nurse leaders mentioned that ‘I had to absorb all their concerns’ under the theme ‘being there for everyone’ where nurse leaders felt overwhelmed and concerned about their employees.48 The impact of constant accountability doubled with the demand placed on nurse leaders during the COVID-19 pandemic leaving them more vulnerable to burnout.51 Nurse leaders reported that their values were challenged and that they sometimes lacked confidence in their own abilities during the COVID-19 pandemic.51 Tahernejad et al 52 suggested that healthcare employees as first responders endure a great deal of stress in emergency situations. These individuals are at risk of various psychological disorders, and they need to be continuously screened to prevent the germination of suicidal thoughts and attempts.52
Common method biases
This study has some limitations; one is the cross-sectional design, which does not allow causal relationships to be determined.31 A longitudinal study could be more appropriate because burnout is suggested as a sequential process that develops over time.7 Under-reporting of burnout may also be present in this study both due to a healthy worker effect,53 and because nurse leaders who are experiencing burnout may not participate in a survey like this. Despite these limitations, a major strength of this study is that addressed gender as an important social determinant of health that directly impacts one’s own health and well-being. Therefore, we proposed a broader approach, which addresses gender differences using a sample that adequately represented male nurse leaders in the workforce.
Implications for future research and practice
Study findings suggest that work-life balance influences personal burnout, COVID-19 influences client burnout and gender differences influence client burnout and personal burnout. More exploratory research is needed to better explain these relationships because findings in the current study cannot explain why there were statistically significant differences between male and female nurse leaders in personal and client-related burnout. This is important because burnout produces turnover and poor job satisfaction and focusing on the well-being of nurse leaders is imperative. Male and female nurse leaders experience burnout differently, which demonstrates the importance of addressing gender when examining how nurse leaders react to different factors leading to burnout. In employing a gender lens framework, future researchers can engage in meaningful conversations on the role of gender in the daily practices of nurse leaders. Researchers also might study how the pressures that working women nurse leaders face intensified during the COVID-19 pandemic. These might widen the scope of conversations to include family-friendly policies and attention to the needs of women nurse leaders.
The current study suggests that hospital decision-makers could provide positive psychological support to avert and alleviate the personal burnout symptoms of male and female nurse leaders during COVID-19. Personal burnout might be experienced because of many unlimited reasons related to one’s own life. Why personal burnout was exacerbated among female nurse leaders during COVID-19 needs to be further explored using qualitative research methods. Taking into consideration that protective psychological skills can be taught, healthcare organisations can assume responsibility for teaching approaches to prevent burnout. This approach can encompass early identification of at-risk individuals such as being female and having a managerial or administrative nursing position, in an endeavour to reduce the long-term personal consequences of burnout. Therefore, both the prevention of personal burnout and effective wellness strategies can be incorporated systematically for female nurse leaders.
From another angle, this study highlighted that male nurse leaders during COVID-19 experienced burnout because of working with clients, patients and other employees. From the very beginning, researchers in this current study did not specify the exact definition of clients while distributing surveys. So, it is difficult to predict how to prevent client-related burnout for male nurse leaders, because they may have defined it differently. Future researchers might guide new areas of research specific to male nurse leaders by defining the word client for male nurse leaders who occupy different managerial positions in the healthcare sector and compare it with the results of this investigation.
Conclusion
This study examined personal burnout, client burnout and work-related burnout of female and male nurse leaders after the COVID-19 pandemic while controlling for the impact of work-life balance through a gender lens. The results of this study suggest that nurse leaders’ gender is significantly related to personal burnout and client burnout, work-life balance influences personal burnout, and COVID-19 influences client burnout. Gender is an important indicator to make this study hold for different groups considering the leadership differences between men and women nurse leaders. A gender lens framework should be employed in future research to identify other avenues to support nurse leaders in executing their difficult but important roles. Findings in the current study cannot shed specific information about why some relationships were significant. More exploratory research is needed to better explain these relationships. This is important because burnout produces turnover and poor job satisfaction and focusing on the well-being of nurse leaders is imperative. Employing a gender lens framework might help widening the scope of conversations about including family-friendly policies and attention to the needs of women and men as nurse leaders. These policies might include but are not limited to paid childcare, flexible time off, access to paid time off, mandatory overtime laws and the need to decrease nurse to patient ratios.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board approval (#2022-0582) and MOD01_2022-0582 were obtained before implementation of study procedures from the University of Cincinnati. Electronic informed consent was obtained from the respondents to make sure that they fully understood the risks and benefits of being included in the study.
References
Footnotes
Contributors LA and GLG contributed to the study design. LA and GLG, CS and KGD contributed to the data collection. LA contributed to the data analysis. LA wrote the main manuscript text. GLG suggested substantive editorial changes. GLG, CS and KGD revised the manuscript. LA is the guarantor of the study. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.