Article Text

Abstract
Background Adolescence represents a pivotal period for the initiation of smoking behaviours. While family, peer and social groups serve as significant reference groups influencing adolescents’ decision-making process, there remains a paucity of research that examines how diversified reference groups influence their smoking decisions.
Objective The objective is to compare normative and informative influences given by different reference groups on adolescents’ smoking decision-making.
Design This study applied reference group theory and used the card sorting technique. Adolescents were presented with 16 cards portraying various reference groups and 27 cards portraying different types of reference group influences. They were asked to construct sentences as smoking-elicited and smoking-inhibited cues and ranked these influences based on their relevance to their smoking decision-making.
Participants The participants were recruited from four cities in the North, Central, South and East regions of Taiwan. The study sample consisted of 297 Taiwanese 11th graders drawn from high schools, vocational high schools and night schools.
Primary outcome measures The most influential reference group among smokers, former smokers and never smokers.
Results Our results of multivariable logistic regression show that for current smokers, having a smoking best friend (aOR=7.58, p<0.01), having a smoking colleague (aOR=3.83, p<0.01) and participating in ceremonial dance performances (aOR=4.62, p<0.01) are more likely to smoke. Peers play an important role in providing smoking-elicited cues for current smokers. Families provided the most smoking-inhibited cues for former and never smokers. Normative influences such as encouraging adolescent smoking provided more cues for adolescents than informative influences such as releasing stress by smoking.
Conclusions Adolescent smoking behaviour was influenced by peer norms, while former and non-smoking behaviours are associated with family norms. Therefore, tobacco prevention efforts should focus more on family-level interventions to discourage smoking initiation. Smoking cessation programmes for current smokers should address the reduction of peer pressure to smoke. Moreover, schools and community partners should collaborate to develop effective smoking cessation strategies, particularly for high-risk groups such as adolescents who involved in ceremonial dance performance.
- Adolescent
- Peer Group
- PUBLIC HEALTH
- Family
Data availability statement
Card statements of reference group influence were displayed in online supplemental data. Data are also available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study’s notable strength is the use of card sorting techniques, which allowed adolescents to simultaneously compare and prioritise sentences in relation to their reference groups and influences.
A limitation is that this study presents reference group influences on adolescents’ current smoking status. Changes in smoking initiation and continuation in the reference group were not examined.
Introduction
Smoking behaviour often begins in high schools and continues into adulthood. The Global Burden of Diseases study showed that the global smoking prevalence increased from adolescence (15.5%) to a peak in the middle adulthood (28.8%).1 Approximately 82.6% of current smokers began smoking between the ages of 14–25 years. Among current smokers aged 25–54 years, 18.5% started by age 15 and 65.5% by age 20. In 2019, the average age of smoking initiation was 19.2 globally and 21.0 in Taiwan. In Taiwan, smoking prevalence among those aged 15–24 was 15.0, with 24.6% in males and 4.52% in females.2 Moreover, adolescent e-cigarette use has been increasing in many countries.3 4 Adolescent smoking is a strong predictor of adult smoking, leading to significant health and economic burdens.5 6 These findings highlighted the need for more research and targeted antitobacco interventions aimed at adolescents.
Adolescents, in the midst of developing ego identity, are heavily influenced by reference groups in their smoking decisions. According to reference group theory, a reference group refers to a group whose attitudes or behaviours can be compared with other reference groups or at the individual level.7 Reference group influences consist of two types: normative and informative. Normative influence refers to an influence that conforms to others’ expectations, while informative influence refers to the influence of information provided by the reference groups.8 Previous studies have shown that families, peers and other social groups influencing the smoking decisions of adolescents.9–11 Both family and peers can act as both facilitators and inhibitors of smoking behaviour. When parental and peer opinions conflict, adolescents tend to behave and imitate their peers, and parental influence decreases with adolescents’ age.9–11 However, Trucco et al 12 found that while peer norms positively influenced e-cigarette expectancies, parents’ disapproval reduced adolescents’ intentions to use e-cigarette. On the contrary, those with religious beliefs were less likely to smoke compared with their counterparts, likely adhering to doctrine of abstinence.9 13 During social interaction, the positive or negative effects from their family, peer and social groups provide cues that either promote or inhibit smoking. Therefore, it is imperative to investigate how reference groups influence adolescents and whether the influence varies by smoking status.
Compared with developed Western and developing Asian countries, the overall smoking rate among Taiwanese adolescents was relatively low2; however, smoking prevalence varied by the types of high schools attended. Lin and Gebel14 found that the type of school adolescents attended—whether vocational or academic track—was associated with smoking behaviour. Adolescents in vocational schools had a higher risk of smoking compared with their peers in academic high schools.15 According to the Health Promotion Administration (2022), smoking rate in 2019 was 2.8% in senior high schools, 7.9% in vocational high schools and 31.7% in nigh schools.14 The low adolescent smoking prevalence may be attributable to the implementation of smoke-free school policies and tobacco control campaigns in Taiwan.16 As Taiwan is a hybridised country that has been able to embrace the features of both Eastern and Western cultures, how reference groups and their influences interweave and thus affect adolescent smoking decisions should be clarified. Furthermore, most studies used a traditional approach by analysing the effect of reference groups using regression analyses.17 18 Few studies consider both smoking-elicited and smoking-inhibited cues from various groups simultaneously. Understanding the crucial reference groups and how they play a role in influencing adolescents with different smoking statuses could better inform the future development of intervention, especially tailoring strategies to influence adolescents’ smoking decision-making. Therefore, the objective of this study was to understand normative and informative influences given by different reference groups on adolescents’ smoking decision-making, and how these influences differ according to the adolescents’ smoking status.
Methods
Study design
This study used card sorting techniques developed by Spencer and Garrett.19 Card sorting is a user-centred technique and a quick and valuable way to explore personal perspectives on specific topics. Researchers created card samples by synthesising the information of transcripts from tobacco control focus groups. A previous study suggested that 15–25 participants be enrolled in each cart sorting group.20 In addition, a self-administered questionnaire was used to collect adolescents’ backgrounds in order to analyse their associations with the reference group ranking. Based on the rule of thumbs, the number of participants should be 10 times the number of predictors.21 In the questionnaire, there were 15 predictors and three dummies, so the sample size should be more than 180. We applied purposeful sampling as we targeted high-risk adolescents. After obtaining agreement from the schools, we conducted class-based card sorting in four cities in Taiwan from December 2014 to May 2015.
Participants
We selected 11th graders as our study participants due to the highest prevalence of current smoking rates (13.1%) in high schools.22 To reach more high-risk participants, adolescents with a percentile rank lower than 50 on the high school entrance exams were selected because previous studies revealed that smoking was more prevalent in adolescents with lower academic performance than in those with higher academic performance.23 24 To cover diverse geographic areas, we purposively selected participants from four cities in Taiwan: New Taipei, Taichung, Tainan and Taitung. In each city, we selected one class from one high school, one vocational high and one night school, respectively. Adolescents aged 16–18 without intellectual disabilities were invited to participate in this study. A total of 297 participants completed the card sorting. The response rate was 89.6%.
The development of card samples
In this study, the cards samples used were developed based on the data collected from a subproject of the collaborative international project on programmes and policies for tobacco control (Health Promotion Administration, Ministry of Health and Welfare, Taiwan, 2014, Project Number (withheld for anonymity)), in which 13 focus groups of high school faculty members participated in tobacco control programmes and 18 focus groups of current and former adolescent smokers in high schools were conducted.
We designed the contents of card sample based on the framework of reference group theory, including reference group and reference group influence. Individuals who were mentioned in the focus group transcripts were extracted and were categorised into a ‘reference group’. In the category of the reference group, we identified three overarching categories: family, peer and social group. Family refers to adolescents’ immediate family members and their relatives. Peer refers to adolescents’ friends or those in similar age cohorts. The social group refers to people who engage in particular social activities or other non-relative elders. There were 16 cards of reference groups, including six cards in the ‘family’ reference group (mother, father, older siblings, etc), four cards in the ‘peer’ reference group (classmates inside the school, friends outside the school, etc) and six cards for ‘social group’ (eg, church member, colleague, ceremonial participant, club member, etc).
The smoking-related actions or behaviours perceived by individuals were recorded in the category of ‘reference group influence’. Normative reference group influence refers to adolescents perceiving rewards, punishment or values received by the reference groups from social norms due to their smoking or non-smoking behaviours. Informative influence refers to smoking or non-smoking messages that reference groups deliver to adolescents. The reference group influence categories consisted of 12 cards for normative influence (eg, encourage me to smoke, enforce me to smoke, etc) and 15 cards for informative influence (eg, release stress, become popular, etc) Smoking-elicited cues refers to the smoking temptation that adolescents are elicited by reference groups and their influences, whereas smoking-inhibited cues refers to the smoking cues that adolescents are inhibited by reference groups and their influences (Rehme et al, 201825). The card statements were displayed in the online supplemental appendix tables A1 and A2). To avoid statements not mentioned in the cards, six extra blank cards were provided to the participants. We consulted three experts in the tobacco control field for suggestions and chose two current smokers, one former smoker and two never smokers to pilot test the card sorting procedures and content of the cards. We then modified the card samples and adjusted the procedures for the formal survey.
Supplemental material
Card sorting process
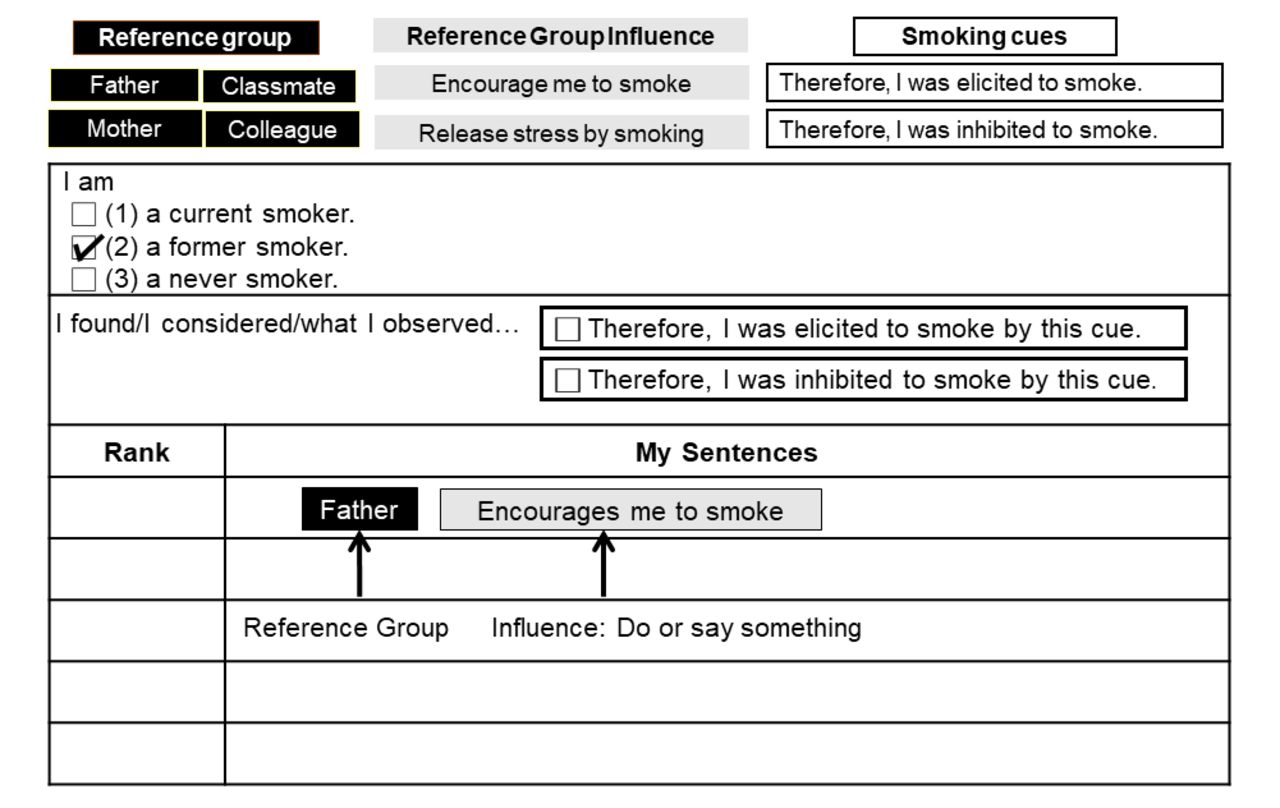
In card sorting, adolescents chose their smoking status first. Those who had smoked any kind of tobacco products currently or in the past 30 days were defined as ‘current smoker’. ‘Former smoker’ refers to youth who had never smoked in the past 30 days but had tried any kind of tobacco products in the past.5 ‘Never smoker’ refers to adolescents who had never smoked as of the time of the survey. After choosing smoking status, adolescents then started to make sentences. In each sentence, one ‘reference group’ card, one ‘reference group influence’ card and one ‘smoking cue’ item was chosen. If one reference group had multiple roles, for instance, a friend who both is an adolescent’s ‘best friend’ and ‘classmate,’ adolescents were asked to fill in the most preferred role. Five sentences were asked to be made as possible as they could. After making sentences, adolescents ranked with the most important sentence as ‘1’ and the least important being ‘5’. If no enough sentences could be made, at least two sentences should be made for comparison. The cards were made of stickers; therefore, participants could easily tear off and paste them on the answer sheet (figure 1).

An example of card sorting.
Recruitment procedure
In each school, researchers contacted the superintendents in charge of implementing a smoke-free campus. The admin leader who agreed to assist with this study selected one of the classes of 11th graders. To enhance research credibility, passive informed consent was used. Teachers distributed study information to parents 1 week before the study. School faculty members were asked not to present in the classroom, and adolescents were asked not to discuss their answers with their classmates during the research. The whole procedure took one class time (50 min) to complete. Researchers explained the study in the first 10 min. Adolescents who were eligible signed the informed consent, filled in the questionnaires and then sorted cards for 30 min. After adolescents completed the study questionnaire and card sorting, researchers rechecked whether there were missing data in the remaining 10 min of class time to assure the quality of data collection. Vouchers or stationery were given as incentives to participants, and tobacco control leaflets were provided for health promotion purposes.
Statistical analysis
Quantitative data were analysed by IBM SPSS Statistics V.22.0 and Microsoft Excel 2016. Pearson χ2 test was used to analyse participant background information. Adjusted standardised residual analysis was performed to determine which cell contributes most to the χ2 value.26 To examine the risk factors for being a current smoker, we grouped former smokers and never smokers together as ‘not current smokers’. Variables with p values less than 0.05 were included in the multivariable logistic regression analysis.
To weigh the importance of reference groups, reversed ranking scores were calculated. According to adolescents’ rank orders, the sentence that ranked first received five points, the second order received four points, and so on, and the fifth received one point based on the method used in a previous study.27 Next, we conducted stratified analysis by smoking status and used stacked bar charts to display the elicited and inhibited cues of reference groups that influenced adolescent smoking decisions.
Results
Among 297 students, 62 (20.9%) were current smokers, 78 (26.3%) were former smokers and 157 (52.9%) were never smokers. Table 1 shows types of school systems, cities and gender by different smoking statuses. There was no significant difference in gender (p=0.08), but were in school systems (p<0.01) and in city (p=0.03). A higher smoking rate was significantly found in night school students and adolescents who lived in Taitung.
School systems, cities and gender among current and not current smokers (n=297)
Table 2 shows the association between reference group smoking and adolescent smoking status. For current smokers, mothers, older siblings, best friends and colleagues are significant smoking reference groups (p<0.05). For never smokers, father, older sibling, best friend and colleague are significant non-smoking reference groups (p<0.05). In addition, our residual analysis also indicated that there was a significant difference between current and never smokers who had colleagues (p=0.01) and who participated in ceremonial dance performances (p<0.01) and school clubs (p<0.01), but there were no significant differences among the three-different-smoking status in church members (p=0.54) (table 3).
Reference group smoking among current smokers and not current smokers (n=297)
Social activities participation among different adolescent smoking statuses (n=297)
Table 4 presents the results from the multivariable logistic regression analysis. The findings indicate that, adolescents with a best friend who smoked were significantly more likely to be smokers compared with those without a smoking best friend (aOR=7.58; 95% CI=3.08 to 18.63, p<0.01). Similarly, those with a colleague who smoked were more likely to be smokers compared with those without a smoking colleague (aOR=3.83; 95% CI=1.60 to 9.19, p<0.01). Furthermore, adolescents who participated in ceremonial dance performances were more likely to be current smokers than those who did not participate (aOR=4.62; 95% CI=2.10 to 10.13, p<0.01).
Multivariable logistic regression of factors associated with current smokers
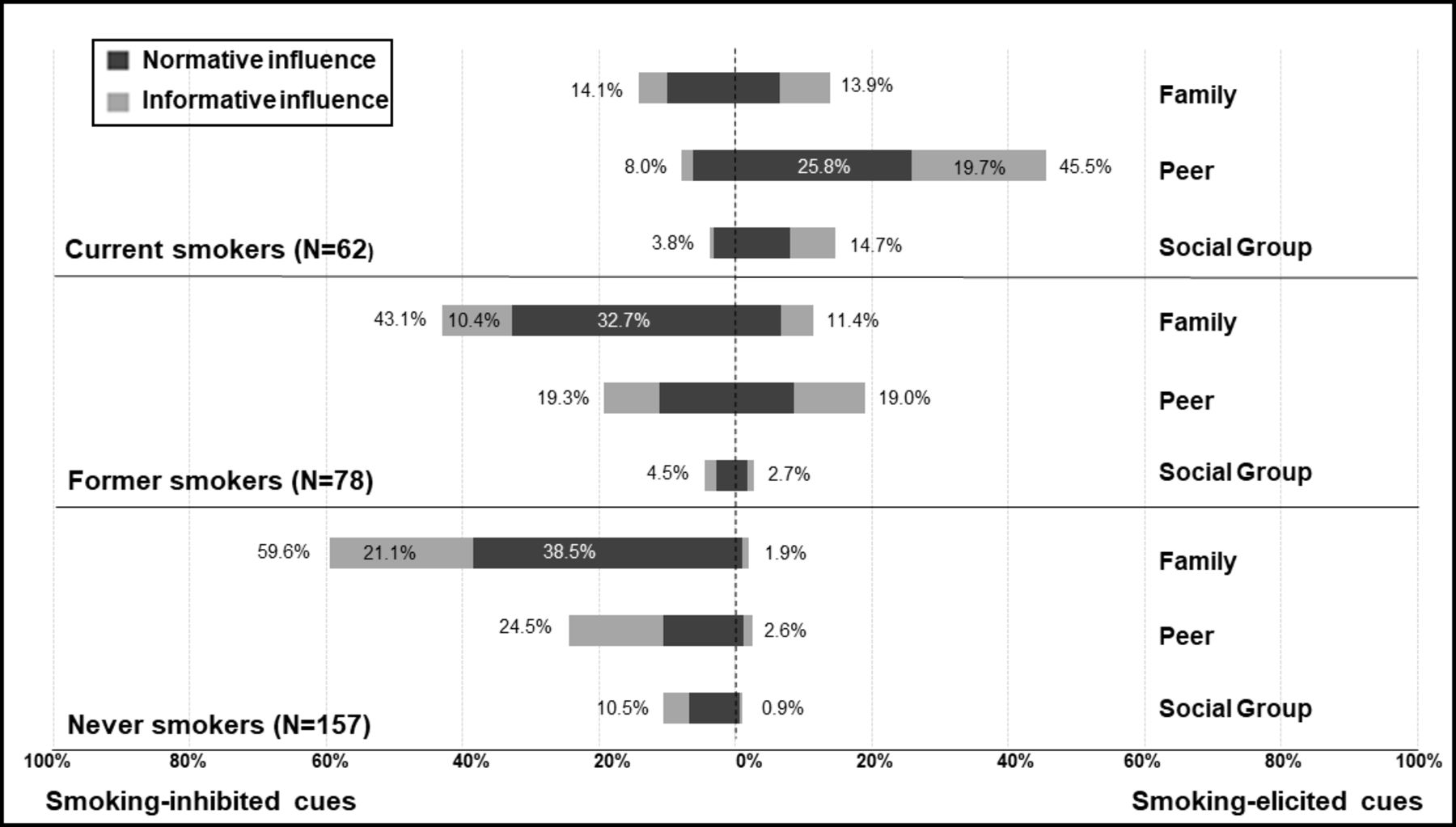
Figure 2 shows stacked bar charts of smoking-elicited and smoking-inhibited cues stratified by smoking status. After weighted scoring, ‘peer’ was placed as the most dominant reference group that elicited adolescents to smoke (45.5%). Adolescent current smokers received comparable smoking-elicited cues (13.9%) to smoking-inhibited cues (14.1%) from their family reference groups. Among former smokers, 43.1% of them reported ‘family’ as the majority reference group that inhibited them from smoking. Adolescents received comparable weighted percentages (19.3% vs 19.0%) on smoking-elicited cues and smoking-inhibited cues in the category of the peer reference group. Among never smokers, 59.6% of them found that family reference groups inhibited them from smoking most. Current smoking adolescents mentioned their ‘friend outside of school’ and ‘best friend’ were the top two influential reference groups. Former and never smokers placed ‘father’ and ‘mother’ as the first and second influential reference groups. Additional cards that adolescents filled in included ‘relatives who do not live together’ in the reference group and ‘smoking smells bad’ was mentioned as one of the reference group influences. We further analysed ceremonial dance performers and colleagues in our card sorting because participants in ceremonial dance and those with colleagues were identified as high-risk groups based on the results of the multivariable logistic regression analyses. The ceremonial dance performance refers to a group of adolescents or young adults who perform dance alongside religious parades or in front of temples on holy days. Such activity is a Chinese traditional culture. Our results show that half of the current smokers (50.0%) had ever participated in cultural ceremonial performance and among them, 45.2% of adolescents mentioned that ‘ceremonial dance performer’ was one of their top five reference groups that elicited smoking behaviours. Furthermore, 61% of current smokers had a full or part-time job, and 31% of those smokers referred to their colleagues as smoking reference groups.

{kind=link}
{kind=link}
Reference groups and their influences categories by smoking statuses. The percentages outside the bar represent the total percentage of each reference group category in either smoking-inhibited cues or smoking-elicited cues. The actual weighted percentages categorised by smoking status are described in online supplemental table A3.
Discussion
This study applied reference group theory to explore the elicited or inhibited cues on adolescent smoking decision-making. Our findings showed that adolescents encounter conflicting cues from family and peer groups, which can either promote or discourage smoking among current and former smokers. Peers have the strongest influence in encouraging smoking among current smokers, while for former and never smokers, family reference groups play the most significant role in preventing adolescents from smoking.
The present study shows that peers were the predominant reference group influencing current smokers. According to Erikson’s theory of psychosocial development, adolescents may encounter the conflict between personal identity and role confusion. To establish their identities and behave independently, adolescents engaged in different tasks and compare with their peers.28 Moreover, in this study, 87.7% of current smokers had best friends who were also smokers. Our results align with previous studies, suggesting that having a best friend who smokes is a high-risk factor for current smoking behaviour. Due to peer influence and peer selection, smoking peers were more likely to make friends with smokers.29 30
The family was the predominant reference group inhibiting smoking among former and never adolescent smokers. The family reference group received a higher weighted score for smoking-inhibiting cues compared with smoking-elicited cues, regardless of smoking status. Two plausible explanations support this finding. First, in our study, ‘father’ and ‘mother’ were consistently ranked as the top two reference groups providing smoking-inhibited cues. It is well-established across cultures that parents serve as protective factors against adolescent smoking. Adolescents under parental supervision were less likely to smoke.18 31 Negative parental attitudes towards smoking also reduced adolescents’ intention to smoke and use e-cigarettes in high school.12 In Asian cultures influenced by Confucianism, adolescents are more likely to follow family rules out of fear of disrupting family harmony.32 Our card sorting results showed that ‘father’ received the highest scores for cues that inhibit smoking among former and never smokers. In East Asian cultures, which are largely patriarchal, fathers are seen as the family leader who teaches through example.33 Thus, our study supports that family, especially fathers, significantly influences adolescent smoking behaviour in collectivist cultures.
Our study indicates that adolescents face conflicting smoking-related cues from family and peer reference groups, a struggle particularly evident among current and former smokers. In Taiwan, where collectivism and individualism intersect, both family and peers play crucial roles in shaping adolescent smoking behaviours. Taiwanese adolescents are embedded in a context that blends elements of collectivism and individualism.34 35 On one hand, as collectivist values, particularly Confucian ideals of group harmony, hierarchical relationships and social norms, continue to guide parent–child dynamics in Taiwanese society.36 On the other hand, adolescents seek for their own peer identities.28 These intertwined values, beliefs and practices act as both encouraging and discouraging factors in adolescents’ smoking initiation and cessation decisions. Future antitobacco campaigns targeting adolescents should take into account the normative and informative interpersonal influences rooted in these cultural practices.
Another interesting finding is that adolescents who engaged in ceremonial dance were more likely to be current smokers. Unlike the dominant Christianity or Catholicism in the West, the main religions in Taiwan—Buddhism, Taoism and folk religion—often involve distinct forms of worship. Smoking, as part of these religious activities, appears to be embedded in Taiwanese subculture. Prasetyo36 similarly noted that in Indonesia, cigarettes were sometimes offered in Buddhism worship practice.36 Consistent with a previous qualitative study in Taiwan, adolescents who participated in ceremonial activities reported that smoking and betel nut chewing were considered essential element of folk religious events, with these risky behaviours often influenced by group members.37 These religion-related activities, though framed as celebratory, foster social interactions among ceremonial dance performers, leading adolescents to adopt behaviours such as smoking, fit in. A similar ‘lemming effect’ has been observed in Western contexts,38 where events such as music festivals bring together young people and contribute to a culture of substance use, as participants share their smoking experiences and establish a norm for such behaviours.39
The present study suggests that antitobacco interventions could focus on reducing peer norms that encourage smoking, while strengthening family norms related to smoking prevention. In Taiwan, there has been limited emphasis on engaging parents or guardians in efforts to influence adolescent smoking behaviour, leading to a lack of family-level interventions aimed at shaping family norms around smoking. Our finding indicated that adolescent smoking or non-smoking behaviour is largely driven by normative influences. A meta-analysis study suggested that interventions such as antitobacco parades or campaigns, common in Western cultures, may not be suitable for Eastern contexts.40 In individualism-oriented Western societies, adolescents were more likely to socialise independently and regain control over their autonomy, avoiding tobacco use.40 41 In contrast, in Asian cultures, group consciousness often takes precedence over individual autonomy. Rather than promoting independence, interventions could focus on group-oriented normative influences. For instance, smoking should not be seen as a means to strengthen friendships. Future interventions should be culturally tailored to address different cultural contexts.
In this study, several limitations should be acknowledged. First, the survey cards were developed based on input from smokers and faculty members in previous focus group studies, meaning that the perspectives of never smokers were not fully considered. However, blank cards were provided for adolescents to contribute additional ideas. Second, as a cross-sectional study, the reference groups identified only reflect the current smoking status of adolescents. Changes in these reference groups may occur as adolescents start or continue smoking, limiting the ability to draw causal inferences. Third, the definition of adolescent smokers, particularly former smokers, was not clearly specified. The category of former smokers may include regular former smokers, occasional former smokers and former triers,42 raising concerns about whether different reference groups influence various stages of smoking behaviour. Future research should more precisely define and categorise adolescent former smokers to enable more accurate analysis and provide targeted interventions. Fourth, this study focused exclusively on cigarette smoking, excluding the increasing variety of tobacco products used by adolescents. Future research could consider the use of multiple tobacco products.43 Last, to increase the sample size of smokers, we did not use proportional random sampling but instead purposefully selected school systems with higher smoking rates. As a result, the overall smoking rate, particularly among female adolescents, is higher than the national average. Therefore, the findings may not fully reflect the smoking behaviours of adolescents across Taiwan.
Notwithstanding, there are several implications for future studies. First, future studies could replicate our study design to further explore adolescent decision-making preferences. Second, our study suggested that tobacco prevention and smoking cessation programmes could focus on key reference groups, with an emphasis on strengthening the role of families in preventing adolescent smoking. Finally, our findings confirm that peer normative influence on Taiwanese adolescent smoking is similar to that observed in adolescents globally, despite the presence of a religion-related smoking subculture. These results contribute to the existing evidence by highlighting the need for culturally tailored interventions that are both acceptable and effective in the Taiwanese context.
Conclusion
Adolescent smoking behaviour in Taiwan is influenced by peer norms, while family norms play a protective factor against smoking. These findings can guide the development of more targeted antitobacco campaigns. To prevent never and former smokers from starting, the focus should be on fostering and reinforcing family-based norms. Efforts to help current smokers quit should concentrate on reducing the impact of peer smoking norms. Moreover, more resources should be directed toward preventing and intervening in high-risk smoking groups, such as adolescents involved in ceremonial dance performances or those with close friends who smoke. By engaging specific reference groups and addressing normative influences, tobacco prevention and smoking cessation efforts targeting adolescents can become more effective.
Data availability statement
Card statements of reference group influence were displayed in online supplemental data. Data are also available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional review board (IRB) of National Yang-Ming University (IRB approval number: YM103068F). Participants provided informed consent prior to their participation in the study.
Acknowledgments
The authors express their gratitude to the school faculty for their assistance and to the adolescents for their participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors H-YT: Conceptualisation, methodology, software, formal analysis, investigation, resources, data curation, writing—original draft, visualisation and project administration. S-FS: Formal analysis, writing—original draft, review and editing and supervision. T-IT: Conceptualisation, methodology, formal analysis, writing—review and editing and supervision. H-YT is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.