Article Text

Abstract
Objective Longitudinal learning often faces implementation challenges within UK medical schools. Some have suggested that the hidden curriculum may be implicated, but there is little evidence regarding how the hidden curriculum influences student experiences of, and engagement with longitudinal learning. Given this, our objective was to explore the impact of the hidden curriculum on student experiences of a longitudinal curriculum based in primary care at a research-intensive medical school.
Design We conducted a longitudinal qualitative study. Students participated in three serial, in-depth semistructured interviews. We conducted a longitudinal thematic analysis.
Setting One research-intensive medical school based in the UK. Data collection occurred in 2021–2022.
Participants 12 penultimate year medical students taking part in a longitudinal primary care placement for 1 day a week over the course of one academic year.
Results We constructed four themes capturing insights on how hidden curricula influenced students’ experiences: (1) A culture which stresses assessment influences student engagement with longitudinal learning; (2) Longitudinal relationships can challenge the hidden curriculum; (3) Support and continuity within primary care improves skills and can influence belonging and (4) Logistical issues influence engagement with longitudinal learning.
Conclusions The hidden curriculum, particularly related to assessment, plays a large role in student perceptions of educational value and subsequent engagement with curricula. In a research-intensive institution, longitudinal learning, particularly within primary care, was perceived as at odds with what was important for assessments. Where longitudinal relationships were successfully established, students became more aware of the benefits of person-centred practice. For primary care longitudinal education to succeed in more research-intensive institutions, there must first be advocacy for greater representation of primary care and person-centred values within organisational structures to ensure meaningful curricular alignment.
- MEDICAL EDUCATION & TRAINING
- Primary Care
- Physicians
Data availability statement
No data are available. As ethical approval was not obtained to make data sharing possible outside of the listed research team, no additional data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This article offers an in-depth, longitudinal analysis of student experiences of the hidden curriculum in relation to longitudinal learning.
A qualitative, interpretivist approach has allowed us to explore the contextual factors influencing student experiences, generating findings for educators interested in implementing longitudinal approaches to education.
Addressing the hidden curriculum as an educator can be challenging; this study draws on the findings of its participants to offer educational recommendations.
Data were influenced by the pressures of the COVID-19 pandemic within the healthcare system which could limit transferability, though many issues brought about by COVID-19 (eg, educational supervisor availability and move towards remote consultations) remain.
We chose not to interview students who dropped out of the programme as we wished to keep our three serial interview time points for consistency of approach—there may have been additional insights from interviewing students immediately following programme exit.
Introduction
Context is crucial. Yet, within medical education, we often assume that approaches to education developed elsewhere can be adopted into our own contexts.1 When things go wrong, and institutions are mired in the heavy cost of unsustainable change, those involved turn away from change and its usually well-intentioned principles.2 Within the UK, longitudinal learning (LL) is a new approach to clinical education that has received mixed reviews from medical students and failed to be sustained beyond a pilot stage at several institutions.3–5 This contrasts with experiences internationally, with some tentatively suggesting that hidden curricula within the UK that marginalises holistic approaches to care, and subsequent impact on student engagement, might be a key factor.3 6 Given the critical need to graduate holistic doctors7 and LL being an effective way to achieve this,8 9 research is necessary to explore the possible ways hidden curricula across medical education and healthcare environments influence student experiences of LL. Through exploring this complex relationship, we can better offer recommendations for advancing the mission of holistic care and enhance LL implementation.
What is LL?
LL is an umbrella term inclusive of a spectrum of educational approaches which prioritise longitudinality (ie, activities which are sustained over time.10) The spectrum of longitudinal approaches to education includes longitudinal integrated clerkships (LICs), spiral curricula, educational portfolios and longitudinal placements (which encompass some longitudinal contact but do not meet formal international LIC criteria.)4
Divisions exist regarding terminology and the structure of longitudinal education that is necessary to achieve evidence-based benefits.11 However, there is agreement that some longitudinality is better than none in advancing the mission of facilitating holistic, person-centred care.12
What are the barriers to LL?
Harding6 explores differences between the US and the UK geography and student demographics (eg, graduate entry) which could contribute to poorer student engagement in LL in the UK. Harding6 also suggests that institutional barriers exist, including the funding of the scale of change necessary for LL. Brown et al3 develop this point, and speculates the existence of a hidden curriculum that marginalises the importance of LL for medical students and hampers engagement.
The hidden curriculum sits outside of what is formally taught and impacts knowledge and behaviour (such as peer groupings, how role models behave and what is said vs what is done)13 it plays a critical role in whether educational innovations succeed.14 It is formally defined as ‘a set of influences acting on students as a result of their presence within a specific organisation’,15 and can have neutral,16 negative17 and positive impacts.18 It involves messages conveyed to students as a result of mismatch between what an organisation says, and what an organisation does in practice.19
UK LICs are often based in primary care and often, a hidden curriculum exists that marginalises the importance and impact of primary care contributions and careers.20 It is likely therefore that LL in the UK (often based in primary care) will be influenced by several factors operating at the level of the hidden curriculum.
Purpose of this study
To the best of our knowledge, no studies have explored the ways in which the hidden curriculum influences student experiences of longitudinal programmes. This is a critical gap, given the variation in student experiences evident between the UK and international literature and due to the emphasis placed on student feedback in organisational decisions about programme delivery and development.
Therefore, in this study, we explored the impact and influence of the hidden curriculum on student experiences of a longitudinal curriculum in a research-intensive medical school. In doing so, we hope to begin a conversation regarding how the hidden curriculum can influence LL and offer recommendations for enhancing engagement and improving the sustainability of LL within medical schools.
Methods
We conducted a longitudinal qualitative study to explore penultimate year medical students’ experiences of a longitudinal primary care placement at a research-intensive university over the course of one academic year.
Context
In 2021–2022, a pilot Longitudinal Integrated Apprenticeship (LIA) was run in a research-intensive university, for 48 self-selected penultimate year medical students for 1 day a week over an academic year (41 weeks). The placement was delivered in primary care and drew on the principles of continuity and relational approaches to education, central to LL and international definitions of LIC’s model. However, the LIA was not restricted by the time-based definition stipulating that LICs should be run on a full-time basis for the duration of the programme.21 The purpose of the LIA was to provide an authentic, longitudinal apprenticeship, anchored in primary care with cross-specialty collaborative learning. Student objectives ultimately remained the same as non-LIA peers in year 5, with students sitting the same year 5 summative exams at the end of the LIA as the rest of their general cohort.
The morning of the LIA consisted of time in a general practice within the city of London, where students established a caseload of patients to consult with repeatedly. This longitudinal caseload was aligned to the clinical foci of their year—paediatrics, obstetrics and gynaecology and mental health. It is important to note that students also consulted with patients more broadly than this, seeing patients as they presented to each practice, but students and tutors were encouraged to focus on these areas in preparation for students’ year 5 summative assessments.
The general practices involved in the LIA were all urban practices, were of varying sizes (with consequent variations in multidisciplinary team staffing), and many served underserved communities. All practices were assessed prior to students joining for LIA on their ability to meet the requirements of teaching in the LIA and trained regarding course expectations.
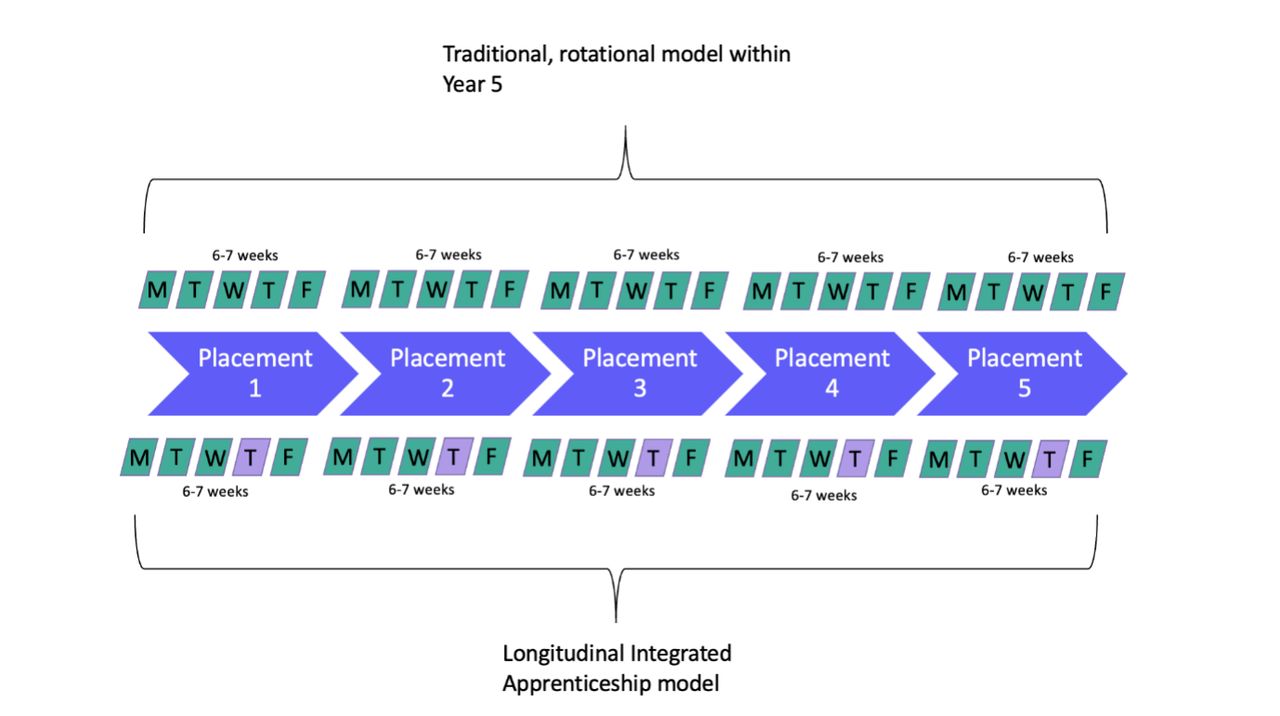
The afternoon was spent in tutorials with local general practitioners, central programme faculty or engaging with a project in a local secondary school. Students remained in the same peer groups for each of these activities and the rest of their week was spent on traditional rotations. A representation of the programme’s structure is provided in figure 1.

How the LIA was structured in comparison to conventional approaches to year five clinical education within the medical school. Purple blocks were days spent on the LIA programme. LIA, Longitudinal Integrated Apprenticeship.
The timing of the LIA programme meant the students were directly impacted by the COVID-19 pandemic. Primary care shifted quickly to remote consultations with reduced face to face patient interactions and many LIA tutorials were held online. The pandemic also led to a detrimental impact on clinical workloads.
Research approach
We worked within an interpretivist paradigm, using a relativist ontology and subjectivist epistemology.22 We chose this approach as we were interested in an in-depth examination of how individual students rationalise their experiences of LL through time.
Sampling and recruitment
All 48 LIA students were eligible to participate. The study was advertised to students within their first LIA tutorial by MB, in August 2021. Interested students submitted contact details on an online form. They were sent a study information sheet and an online consent form. Twenty-four students volunteered to participate; 12 participating students (the maximum number our resources permitted) were selected at random using an online number generator.
Data collection
Participants were invited to complete three serial 1-hour semistructured qualitative interviews conducted online (see figure 2 for details). Recruitment was incentivised, students received a £20, £30 and £40 shopping voucher following their first, second and third interview, respectively.

{kind=link}
{kind=link}
Structure of serial interviews and participant numbers.
We created interview question stems following review of literature, which explored students’ early experiences of the LIA, their thoughts and opinions on possible impact and issues; and memorable experiences or interactions. In interviews 2 and 3, we based questions on students’ prior interviews, shaping prompts around previous contributions and evolutions in experience. See online supplemental material 1 for a full list of question stems.
Supplemental material
Mean interview duration across the three time points was 42 min. Interviews were transcribed verbatim by a transcription company.
Data analysis
We conducted a longitudinal thematic analysis across three interview time points. We analysed data iteratively, and analysis informed subsequent questioning. Following each interview, MELB assigned descriptive codes to each transcript in the software Dedoose. VC second coded two transcripts at each time point to deepen analysis. Following initial descriptive coding at each time point, MELB and VC met to discuss interpretations. MELB made reflective and analytical memos to capture thoughts during coding, and insights from discussions. Following double coding of the third interview, and discussion of this coding, MELB and VC adopted a more longitudinal approach, examining each students’ journey case by case through time, exploring moments of change. MELB and VC created longitudinal memos describing each students’ journey through time. MELB reviewed all study memos alongside descriptive coding and created a set of initial themes. MELB refined these themes through discussion with VC and the wider team and synthesised findings into a report.
Reflexivity
Given the active role that researchers within interpretivist and longitudinal approaches play, reflecting on our backgrounds adds rigour. Our research team consisted of clinicians (vs, NA, RP, SK), non-practising clinicians (MELB) and non-clinicians (VC). Three researchers had previous experiences of LICs and have previously researched their implementation (RP, MELB and SK). Two members of the team taught on the LIA (VS, NA) and so only accessed data once it had been anonymised.
Patient and public involvement
None.
Results
We constructed four themes following data analysis across and through time capturing insights on how hidden curricula influenced students’ experiences:
A culture which stresses assessment influences student engagement with LL.
Longitudinal relationships can challenge the hidden curriculum.
Support and continuity within primary care improves skills and can influence belonging.
Logistical issues influence engagement with LL.
Interview quotes are labelled with participant number, and I1, I2 or I3 to represent the interview number.
Theme 1: a culture which stresses assessment influences student engagement with LL
Throughout student transcripts, there is evidence of a culture which places key importance on assessments and end-of-year examinations.
The lack of perceived alignment between the mission and structure of the LIA (generalist, person-centred care), and their assessment content led to students not valuing the LIA learning opportunities. This tension was greatest during students’ first interviews, where this disconnect led to anxiety, and within the final interviews, given proximity to students’ exams.
Unfortunately, with our GP practice they don’t get many patients that let’s say are obs[tetrics]’ and gynae[cology] related, or even with paed[iatrics]… because of that it’s very difficult to concentrate on the specialties that we have this year.
Student 5, I1
Patients just come in and talk to me about a hundred things. And then I end up overrunning for three hours because I’m trying to sort things out…I just think to myself, all my other friends are in the library studying, I should be studying.
Student 9, I3
The language used to describe this disconnect was often conflict laden. Students felt the need to advocate aggressively for what would help them to succeed in their assessments.
My partner is a little bit more strong headed and will fight his corner. He started his GP placement last week…he told them straight away, ‘I want this and this is all that I want’ and they’re ‘OK’… I didn't really have a chance to fight my corner.
Student 1, I1
Value was placed on the efficiency of knowledge transfer, rather than holistic experience. Students were looking for rapid ways to learn facts. Experience-based learning through the LIA was seen as time-consuming and, therefore, of limited value.
There’s a lot of stuff that we could do in a lot shorter time…we’ve just learnt to become the most efficient learning machines ever… We’re in GP from 9 to 12:30, and then we travel back an hour, and then we have a three hour tutorial. It could definitely fit in a shorter time and then you’d have more free time in the afternoon to study.
Student 9, I1
I'm definitely learning because it’s nice to see how the child is progressing etc. But I suppose it’s not as high efficiency as other forms of learning… rather than just having like a video on a child as they develop
Student 1, I1
A hidden curriculum which promoted assessment-driven learning led to participants finding patients for their longitudinal caseload in a reductionist way (as conditions that aligned with course requirements designed with examinations in mind).
We’ve got one psych[iatric] patient so far, we’re trying to get another… paed[iatrics], we luckily have a patient, a mother, with twins.
Student 2, I1
95% of [my patients] aren’t specialities and I've told them about 500 times now and this is just the way it is and I'm done fighting them because it’s just not going to happen and whatever, it’s fine now.
Student 9, I2
Even for those who discussed understanding the benefits of the LIA, it was still framed as a loss—students were losing a day peripheral to their needs and success. In addition, there was tension between primary and secondary care, with the hidden curriculum supporting the superiority of secondary care for learning. The student below left the programme following this interview.
One thing that’s been quite challenging, is whether I feel it would be sensible to continue LIA. Because on the one hand, LIA… has been a very beneficial experience, but the con of how the year has been scheduled is the fact that I get two less days in hospital, and that has been a big challenge, because it’s impacted how many hours I get.
Student 12, I1
Theme 2: longitudinal relationships can challenge the hidden curriculum
During students’ first interviews educational value was seen as time-efficient knowledge transfer to help pass exams; however, there were critical shifts in how students discussed educational value through time. Some students began to challenge previously held assumptions that the content of their end-of-year examinations was paramount.
LIA is really, really valuable for learning to be a doctor… if the exams were aligned with what being a doctor actually is, then LIA would be more useful.
Student 7, I2
The way we’re examined…pushes us to try to learn these patterns … I don’t think these are great markers of being a good doctor… I know people that aced the exams, and I wouldn't want them treating me…you don't need to go to your placements to pass medical school. I find that so amazing. I tend to go to the placements quite a lot, and I see most of my colleagues and peers not turning up. It’s purely because you don't need to do it to do well in exams.
Student 3, I2
As time progressed most students had longitudinal contact with patients by the second and third interviews.
Before I wasn’t getting too many panel patients from each of the three specialities, whilst now I’ve had a few more… the two [tutors] we see regularly… they [sorted] it
Student 6, I2
Longitudinal contact with patients facilitated students’ involvement in their care. Students described roles which included organising patient care, outreach (eg, giving vaccinations to patients at home), screening, acting as a point of contact for families, encouraging compliance and greater detailed communication with patients.
We did this home visit on a patient…I did a GPCOG [General Practitioner Assessment of Cognition] assessment for dementia. I actually found that he had terrible, terrible memory issues.
Student 3, I3
Pervading all these roles was a perception that students were adding value to patient care.
This patient who came in with gynaecological problems…they came with a bunch of symptoms… the GP supervisor…came in and they were like ‘yes, sure, we can do the gynae[cology] referral… the doctor was literally about to leave the room… I was like ‘oh, and also shall we prescribe something for the constipation’ … the patient was really happy about it because they were saying it had been bothering them a lot… that was nice because it felt like it made a difference.
Student 8, I3
As students developed relationships with their supervisors and with patients, several changed their opinion during their second interviews that the value of learning lay not in passing exams, but in preparing for practice as a doctor through enhancing their ability to connect with patients. This shift is evident in excepts from Student 6’s first and third interviews.
It’s mainly just trying to get the most relevant patients for this year… that’s the main thing that we’re struggling with… I’m worried about exams…. because I’m not getting the actual patients I need. It’s useful for being a doctor, but it’s not useful for this year
Student 6, I1
Because you’re encouraged on the LIA to follow up on patients… I phoned [a patient] again. And she opened up to me…because I’d seen her before…it was a moment of development as a medical student because you feel like you’re becoming a better student doctor…often you feel like…I don’t know what I’m doing. And then suddenly, something clicks and you feel like things are coming together more in this year because I’ve seen so many patients.
Student 6, I3
However, this shift was not evident among all students with two dropping out entirely. Some maintained their views that the LIA was of little educational value, or became more adamant of this as exams approached in interview 3. Where student perspectives seemed not to shift, there were notable issues with longitudinal patient contact and supervision including: a lack of supervisor support in establishing a longitudinal patient panel; issues with student–supervisor relationships and issues with supervisor availability.
LIA has very much nothing to do with my exams…the way it just ended up being for me is me just doing medication reviews and seeing patients that just came in with nonspecific complaints and isn’t tailored…with my GP tutor…I wouldn’t say it’s the closest of relationships…she’s… the only partner…she has loads of difficult patients that will just walk in, demanding to see her. And then I have to see her after every patient… it has put a strain on the relationship because I am just a lot of work
Student 9, I3
Theme 3: support and continuity within primary care improves skills and can influence belonging
Just as relationships with patients and supervisors were influential in whether students’ perspectives of educational value shifted throughout the LIA, they also had large impacts on skill development, and belonging.
Students described the development of several skills following involvement in the LIA. In early interviews, skills discussed were mostly to do with application of knowledge to practice (eg, diagnostic skills). However, in later interviews, students discussed higher level skills around diversity and developing counselling skills.
In GP, I find that a lot of our caseload so far have been psychiatry. Given that my first big placement in fifth year has been psychiatry, it’s been pretty useful being able to see psychiatry cases that are in the community in a GP setting as well as in the hospitals.
Student 12, I1
… it was really humbling to realise that my perception of open [mindedness] is… the tiniest fraction of the breadth of diversity… I was talking to a Muslim patient, that’s fasting for Ramadan and [asked] ‘can you tell me a bit more, so we can use your medication around your fast, and how we can make this work?’
Student 2, I3
When students were supported by their supervisor to consult independently with patients, and when students’ responsibility was advanced over time, students felt more like they belonged as doctors.
I feel more like an equal member of the team…in LIA… what’s so good about it is that you’re seeing patients yourself… having your clinic gives you autonomy and it gives you more power to be a doctor in that sense and you’re an actual part of the team
Student 6, I3
Students felt continuity of location facilitated trust with their supervisors and, sometimes, other staff members. Trust enhanced students’ collaboration and active participation within their GP practice. Students also voiced the development of trust with patients, which they perceived to exist through increased patient openness over time, patient comfort and gratitude. Gratitude, in particular, had a large impact on students sensing they belonged, as they felt they were making a difference to patients’ lives.
You’re just an add on that floats around the ward. While in GP you are such a strong, active member, and you have a role and you are such a key to the whole consultation that, they're just a completely different experience.
Student 2, I2
…she brought in a card and some chocolates for me … it was really nice to be, gosh, I got a card from someone because you see so many patients and you can become quite distant from the fact that you do, genuinely, have a real impact on certain people.
Student 1, I3
The level of responsibility permitted varied within students’ experiences depending on the doctor supervising them. Throughout all interviews, discussion of ‘luck’ was common. Where students felt unsupported, impacts on skill development were less frequently described, and discussion of belonging was absent.
I feel like I did learn quite a lot from it, but then there’s always the possibility that you might not like the way that your GP supervisor supervises, so then that makes it so that every week when it gets to, it’s like ‘Oh God, Thursday is coming up again’.
Student 8, I3
Though some students discussed the LIA as confirming or advancing general practice career aspirations, some also spoke of their disillusionment with systemic issues currently affecting general practice, and the wider healthcare service. For one student, this confirmed their desire not to practice clinically once qualified.
…seeing some of the flaws in the medical system, and seeing how badly it works I… have been made aware of how some parts of the system are just not working…I think I've pretty much made my decision to go into [another career] and not continue in the field.
Student 3, I2
Theme 4: logistical issues influence engagement with LL
There were several logistical issues within LIA which influenced student engagement, including: long commutes to GP practices; perceptions of poor supervisor preparedness; scheduling difficulties with longitudinal patients and a tightly packed schedule outside of the LIA.
I’m travelling about three or more hours in one day… it’s wasting time.
Student 6, I1
Many students felt that the LIA represented something additional for them to engage in and so was seen as an extra challenge to cover secondary care assessment competencies (despite opportunities in LIA to formally meet these).
There’s a logbook that you have to do for oncology… the thing is, we have two fewer days because it’s a two week placement, but we’re not there on both Thursdays and we have to complete the logbook, the same logbook, which means that we have to do the tasks in a shorter period of time.
Student 4, I1
For some students nearing exams, engagement in the LIA wavered further with some negotiating time away from LIA to spend time in secondary care.
…if it’s going to be a particularly useful day in [hospital] placement to be able to just tell the GP that this is really important I’m going to prioritise this if that’s okay, and he’s always given me his blessing, so that’s quite useful.
Student 1, I3
Though some students developed positive relationships with their supervisors and with patients, community formation in a broader sense (with practice staff, the interprofessional team, and with local communities) was unsuccessful. In their limited time on LIA, students largely did not have the chance to get to know other staff members or get to know the needs of their patient community. Logistical issues with longitudinal patient follow-up compounded this further.
We don’t really see other nurses or GPs. We don’t interact much with the reception staff…we haven’t really built much of a relationship with them, but I think that’s probably because we’re there only once a week.
Student 6, I2
I’m not sure if I would say I have built up relationships in the community… because we didn’t see that many patients
Student 5, I3
Community formation as a peer group also seemed lacking. Most students appreciated being placed with a peer of their choice, but relationships with LIA peers outside of this were rarer (despite group teaching and a group outreach project). Peers sharing negative stories of their experiences during the LIA and comparing LIA experiences to peers outside of the programme had a large impact on student engagement.
…on Thursdays my peers are in hospital and some of them are having tutorials and they’re having clinical skill sessions…I’m not having this hospital placement activities and I'm having LIA but like, in terms of knowledge, can I balance that out?
Student 2, I1
Discussion
This study provides empirical evidence that the hidden curriculum plays a key role in the challenge to implement LL within the UK. In this study, the hidden curriculum, which manifests strongly in relation to assessment, plays a large role in student perceptions of educational value and subsequent engagement with formal curricula. In a research-intensive institution LL, particularly within primary care, is perceived by students as at odds with assessment regimens.
Students were influenced by a hidden curriculum which promoted exam achievement and knowledge acquisition at the expense of other aspects of clinical practice (such as person-centredness). The hidden curriculum is in-action when there is a perceived mismatch between what an institution says, and what an institution does.23 In this study, students perceived a mismatch between what they were being told formally to do (LIA focused on patient experience) and what was happening in assessment at both institutional and national levels. Students perceived assessments focused on knowledge retention and recall in secondary care specialties, rather than patient-facing or holistic generalist skills. It is well known that assessment influences learning24 and has importance to career progression.25 Faculty involved in the development of the LIA had limited control of students’ summative assessment meaning students were participating in LL, but were ultimately aiming for the same objectives as their non-LL peers. This is noted within wider LL literature as a particular challenge that can detract from engagement with longitudinal models.12 We suggest that an assessment-laden hidden curriculum can negatively influence student engagement with values of LL. The national medical licensing assessment (MLA) is due for full implementation in 2024, a move likely to further fuel a specialty condition ‘tick box’ culture.
There was also a tension between the generalist focus of the LIA, which was based in primary care, and a medical culture which promotes specialty driven knowledge. The hidden curriculum often promotes general practice as occupying a lower position in the hierarchy of medical specialties. Previous research has noted that undergraduate training reinforces this view that general practice is a low-prestige specialty and relatively less academic than secondary care specialties.26 This stereotype also exists internationally within the academic literature.27 28 This study supports the ongoing presence of this stereotype and expands on this by demonstrating the role of the hidden curriculum in shaping these hierarchical perceptions.
As an educator the challenge of addressing the somewhat nebulous and wide-reaching concept of the hidden curriculum may seem daunting. Reassuringly, in our study, where longitudinal relationships between students, their supervisors and their patients were successfully established and supportive, students became more aware and critical of the dominant hidden curriculum. The triad between students, teachers and patients in LL is critical to facilitating learning,29 and these relationships facilitate identity development.30 In this study, students came to value continuity of care, and felt more like doctors as they took active, meaningful roles in patient care. This was not a universal experience for our students, several practical considerations may have limited students’ opportunities for relationship development, such as the impact of the pandemic on primary care, other curricular pressures (eg, logbook numbers), and the limited time of 1 day a week spent engaged in LL. More time may have shifted some students’ perspectives, however, in the face of dominant messaging regarding assessments and the value of primary care versus secondary care, longer longitudinal placements are unlikely to be a suitable remedy. Similar curricular changes such as excusing LL students from secondary care logbook numbers are likely to have a similar limited impact. Instead, we suggest educators should focus on ways to challenge and unpack such negative hidden curricula.
Approaches will vary depending on each institution but may include suggestions listed in box 1.
Suggestions for exploring hidden curricula from the literature
Frank discussion of students’ experiences of the hidden curriculum (which Neve and Collett31 suggest can empower students to think critically).
Assessment of organisational hidden curricula locally (a ‘hidden curriculum audit’).3
Advocacy for person-centred values to inform institutional and assessment strategies (using Bansal et al’s32 realist theory to inform development of this strategy).
Small curricula changes to enhance longitudinal relationship development (eg, longitudinal mentoring).33
Early longitudinal education to influence student value formation at the beginning of their medical careers (at early stages, medical student identity is still forming and receptive to integration of new values like person-centredness).34
A focus on exploring an institutions’ hidden curriculum in relation to assessment. Questions may involve what messages an institution shares with students given current assessment regimes, and which values and educational measures these regimes may devalue.
Limitations
The data of this study were gathered during the COVID-19 pandemic, some of the logistical challenges may not be transferable beyond a pandemic context. We chose not to interview students who dropped out of the programme and kept our three serial interview time points for consistency of approach—there may have been additional insights from interviewing students immediately following programme exit. We used a convenience sampling approach, guided by available resources and our previous experience of longitudinal qualitative research. Though we conducted 31 interviews with 12 participants, which allowed us to gather rich, qualitative data, our convenience approach may have meant we did not hear from the diverse range of participants in the LIA. Despite this, and though this is a single-site study, we maintain the results of this research are transferable, due to our in-depth consideration of study description, and consideration of key qualitative quality criteria such as reflexivity and transparency of reporting.
Conclusion
Without first exploring and challenging the hidden curriculum, the implementation of LL will remain challenging and will suffer from poor student engagement and prove unsustainable. For LL to succeed, particularly in primary care, there must first be advocacy for greater representation of person-centred values within organisational structures and cultures, including assessment.
Longitudinal placements in primary care offer an ideal educational model in preparing our future healthcare workforce to address increasing health disparities through patient-centred, holistic and generalist-driven practice. This study strongly suggests that the hidden curriculum works in direct conflict with these values and, unless this is addressed head on, further advances in the UK are likely to be hindered. The imminent advent of the MLA with its focus on specialty knowledge may further hinder meaningful progress in moving UK medical education towards what society needs, serving the priorities of its health service and its population.
Data availability statement
No data are available. As ethical approval was not obtained to make data sharing possible outside of the listed research team, no additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Imperial College London Education Ethics Review Process (EERP) (approval number: 2021-088). Medical students provided written informed consent. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Thank you to Dr. Zoe Moula, who assisted with interview data collection. Thank you also to the students who volunteered their time to participate in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Megan_EL_Brown, @Imperial_Medic
Contributors MELB, RP, VS, NA and SK were responsible for conception and design of this research. MELB and VC collected and analysed all study data. MELB prepared the first draft of this paper, and all other authors (VC, VS, NA, SK and RP) revised the work. All authors approved the final version of this manuscript submitted for publication and agreed to be accountable for all aspects of the work. RP is the study guarantor.
Funding This article presents independent research commissioned by the National Institute for Health Research (NIHR) under the Applied Health Research (ARC) programme for North West London.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.