Article Text

Abstract
Background Over 50% of annual deaths in low-income and middle-income countries (LMICs) could be averted through access to high-quality emergency care.
Objectives We performed a scoping review of the literature that described at least one measure of emergency care access in LMICs in order to understand relevant barriers to emergency care systems.
Eligibility criteria English language studies published between 1 January 1990 and 30 December 2020, with one or more discrete measure(s) of access to emergency health services in LMICs described.
Source of evidence PubMed, Embase, Web of Science, CINAHL and the grey literature.
Charting methods A structured data extraction tool was used to identify and classify the number of ‘unique’ measures, and the number of times each unique measure was studied in the literature (‘total’ measures). Measures of access were categorised by access type, defined by Thomas and Penchansky, with further categorisation according to the ‘Three Delay’ model of seeking, reaching and receiving care, and the WHO’s Emergency Care Systems Framework (ECSF).
Results A total of 3103 articles were screened. 75 met full study inclusion. Articles were uniformly descriptive (n=75, 100%). 137 discrete measures of access were reported. Unique measures of accommodation (n=42, 30.7%) and availability (n=40, 29.2%) were most common. Measures of seeking, reaching and receiving care were 22 (16.0%), 46 (33.6%) and 69 (50.4%), respectively. According to the ECSF slightly more measures focused on prehospital care—inclusive of care at the scene and through transport to a facility (n=76, 55.4%) as compared with facility-based care (n=57, 41.6%).
Conclusions Numerous measures of emergency care access are described in the literature, but many measures are overaddressed. Development of a core set of access measures with associated minimum standards are necessary to aid in ensuring universal access to high-quality emergency care in all settings.
- ACCIDENT & EMERGENCY MEDICINE
- Health policy
- International health services
- PUBLIC HEALTH
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
We performed an extensive search in multiple databases and the grey literature of all emergency care access measures according to known the best principles of scoping reviews.
Categorisation of measures was performed according to three separate frameworks of access and emergency care.
This study is limited to the available English-language literature.
Given limitations in the data, we cannot comment on the feasibility of implementing the categorised access measures, provide consensus on which measures correspond to more likely improvements in patient outcomes, nor provide minimum standards for measures.
Introduction
The past 20 years have been called a golden age of public health.1 A dramatic increase in global health funding has expanded healthcare resources in low-income and middle-income countries (LMICs).2–4 As a result, significant reductions in infectious disease-related, neonatal and maternal mortality have been achieved in line with the United Nations Millennium Development Goals.5 Further reductions in global mortality attributable to non-communicable diseases and trauma have been far less substantial.6 While a shift from disease-specific programmes to health system strengthening, equity and social protection has been an important first step, progress on current Sustainable Development Goals remains lacking and has been further hampered by existing health inequities made worse by the COVID-19 pandemic.7
Improvements in both prehospital and facility-based emergency care have the potential to impact many of the SDGs, lead to marked improvements in healthcare systems and reduce deaths across multiple disease categories.8 Estimates suggest that over 50% of annual deaths in LMICs could be averted by the implementation of quality emergency care systems.9–12 The increasing mortality burden of non-communicable diseases, including injury and chronic conditions, coupled with the acute medical needs of emerging pandemics, such as SARS-CoV-2, requires the development of robust emergency care systems.1 13 14
In 2018, the World Health Assembly passed resolution 72.16. ensuring the role of emergency care in all health systems.15 In order to provide further clarity to practitioners and policy-makers on the role of emergency care, the WHO developed the Emergency Care System Framework (ECSF). The Framework defines a set of core essential functions of an emergency care system at the scene of illness, during transport and within health facilities.16 Unfortunately, many who live in resource-limited settings lack access to the human resources, equipment and information technologies needed for a capable high functioning emergency care system.17
Previous descriptions of known measures of emergency care quality18 19 and barriers to emergency care access20 21 have highlighted gaps in emergency care in LMICs, but no comprehensive review on measures of emergency care access in LMICs has been completed to date. The aim of this scoping review is to categorise all known measures of emergency care access in LMICs in order to help standardise and prioritise emergency care development.
Materials and methods
Search strategy
A rigorous search strategy was employed with the goal of identifying all peer-reviewed studies that described measures of access to emergency care in LMICs. For this review, we use the term measure to describe indicators, metrics and other measurable components of access to emergency care. We performed a scoping review using the following databases: PubMed, Embase, Web of Science and CINAHL. A subsequent grey literature search was conducted via both Google and Google Scholar, with searches targeted towards organisations that work on global emergency care.
The initial search strategy (online supplemental appedix 1) was developed within PubMed and adapted for the remaining databases. Search terms included various iterations of access, emergency care and LMICs. Free-text terms and standardised MeSH headings/subheadings were used to optimise sensitivity for relevant literature while minimising excess search results. The reference lists of relevant primary studies and reviews likely to meet inclusion criteria were also reviewed manually to both verify search sensitivity and identify other potentially relevant studies that were not identified by the electronic search. The initial search was performed in 2020, with a subsequent updated search in November 2022.
Supplemental material
The grey literature search was completed via Google and Google Scholar. We performed targeted searches using similar terms relevant to access, including affordability and barriers to care. The search was targeted towards government ministries of health, professional organisations specific to emergency care and among well-established non-governmental organisations, including development agencies and those specific to healthcare policy. There were no initial regional or income-level specifications given to this search.
Studies published between 1 January 1990 and 30 December 2020, English-language, and describing at least one discrete measure of access to emergency care services in at least one LMIC were included. LMICs were defined by World Bank economic definitions as the gross national income per capita of the year the research was performed. Articles were excluded that were clearly irrelevant to the topic, did not involve emergency care, did not describe a measure of access or measurable barrier to emergency care, or did not include data from at least one LMIC. For the purposes of this review, we excluded data specific to emergency obstetric and newborn care seeking (we anticipate a separate forthcoming review on the subject).
Patient and public involvement
Given the nature of this study it was not possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Data processing
Manuscripts meeting initial broad search criteria were imported into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia) and duplicates removed. Initial title and abstract review were performed by two independent authors (SH and JD). Disagreements were resolved by a third reviewer (CBB). The same procedure was followed for full-text review.
Data from included manuscripts were extracted and included the following: author(s) and full citation, publication date and study time frame, location, study type, setting, methodology, access measure(s) reported, and the primary outcome(s). Countries under study were categorised by income level, WHO region, whether the study was local, regional, national or multinational in scale, and whether the populations under study were rural or urban.
Data analysis
A structured data extraction tool was used to identify and classify both the number of ‘unique’ measures, and the number of times a unique measure was studied in the literature. In this manuscript, the summation of all of the times each unique measure was studied is referred to as ‘total’ measures. Unique access measures were aggregated and categorised by access type.
The term ‘access’ is often used as shorthand for distance, leading to a focus on individual patient proximity, either spatial or temporal, to a given health service.22 While vital, proximity is but one component of accessibility and may not correlate with the true ability to receive quality emergency care.23 For this scoping review, we revert back to a more expansive definition of access, one rooted in a rights-based approach to emergency care and reflecting the spectrum of fit between user and service and inclusive of five dimensions of access—availability, accessibility, accommodation, affordability and acceptability—as described by Penchansky and Thomas (table 1).24 25 We also reference a modified version of this framework which includes awareness.26 In Penchansky and Thomas’ framework, access is examined through the ‘fit’ of the patient with the healthcare system. For example, a healthcare facility may be available (ie, it exists), but not accessible because of transportation barriers. In addition, the healthcare facility may not have necessary measures to accommodate a patient (such as 24-hour-access or childcare), may be unaffordable, or may be unacceptable (ie, due to poor quality or corruption). While dated, and originally validated in the consumer patient satisfaction world, multiple recent studies on healthcare access in low-income and middle-income studies have shown utility and validity for this framework, including among geriatric healthcare in Southeast Asia, on HIV treatment access during Covid in Ghana, and among displaced in the Lake Chad region of Cameroon, Chad, Niger and Nigeria.27–29
Proposed emergency care access measures for monitoring, evaluation and comparative analysis by access type
More recently, other models have emerged that may provide greater applicability to emergency care. With this in mind, we provide analyses and categorise access measures via two additional frameworks. The ‘Three Delay’ model was originally conceptualised to understand delays in care leading to increased maternal mortality but has been more recently applied to emergency care.30 31 The Three Delay model defines three critical phases of timely care: seeking, reaching and receiving care. The WHO’s ECSF provides another method of understanding emergency care access. The ECSF defines the human resources, equipment and functions necessary for a fully functioning emergency care system at the scene of illness, during transport to a health facility (prehospital) and within healthcare facilities.9 16
All extracted access measures were collected, with similar measures collapsed into singular unique measures. We report the number of unique measures and the total number of times a measure is reported as a number and per cent. Each measure was then categorised according to the three frameworks listed above. Given the heterogeneity of study methods and types, a qualitative analysis and narrative synthesis was undertaken. Thematic analyses focused on the number and general quality of the measures used. Trends and ranges among studies with comparable numeric measures are reported where appropriate. We did not perform a grading of the literature given the overall observational nature of most studies. Criteria proposed by the Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews statement were adhered to in reporting.32
Results
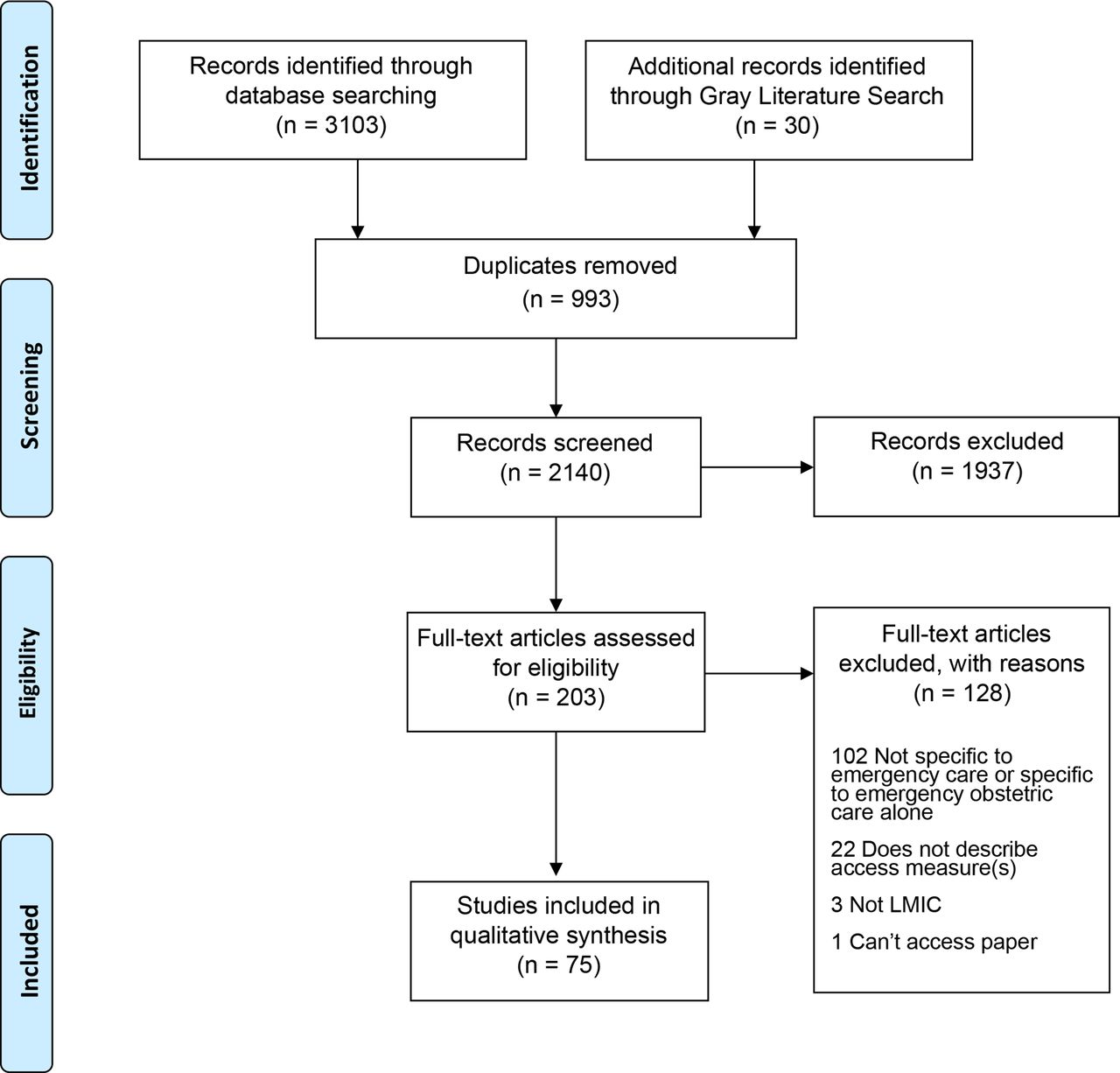
A total of 3103 articles were identified for screening via database searches, and 30 were included from the grey literature and hand searches of relevant literature (figure 1). After removal of 993 duplicates, 2140 articles were screened by title and abstract, 203 articles met criteria for full text screening, after which 128 articles were excluded. In sum, 75 articles met full criteria for inclusion (online supplemental eTable 1).
Supplemental material

{kind=link}
PRISMA flow diagram for review of literature on access to emergency care measures in LMICs. LMICs, low-income and middle-income countries; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
All but 1 of the 75 studies were published in peer-reviewed journals. The majority (n=44, 58.7%) of studies examined access related to general emergency care; 22 (29.3%) were relevant to prehospital care, 10 (13.3%) were specific to trauma care and 1 (1.3%) article focused on paediatric patients (table 2). Geographically, publications included data from all six WHO regions, with the majority from the African Region (n=35, 46.7%). The majority of included studies originated from lower-middle-income countries (n=37, 49.30%), with additional studies from upper-middle-income countries (n=15, 20.0%) and low-income countries (n=11, 14.7%). Twelve articles (16.0%) included data from multiple-income groups.
Characteristics of manuscripts for study inclusion
Methodologically, all studies were descriptive and relied on key informant interviews (n=14, 18.7%), surveys (n=13, 17.3%) or cross-sectional data (n=43, 57.3%). No manuscript reported a comparator group, and the majority of studies were qualitative in nature (n=47, 62.7%). Studies varied in the number and type (patients, clinical providers, administrators) of participants. The majority of studies (n=48, 64.0%) used cross-sectional data and did not specify the number of participants. Participant enrollment ranged from 11 to 32 774 individuals. The types of health facilities under study also varied, and included emergency care as accessed at clinics, district hospitals, referral hospitals (with access to intensive care) and more formal emergency units or departments.
Measures by access type
In sum, 137 unique measures of access were described in the 75 studies (table 3). Of the 75 total studies, most (n=49, 72.1%) reported more than one unique measure. Based on Penchansky and Thomas’ categories, the highest number of discrete measures of access described accommodation (n=42, 30.7%), followed by availability (n=40, 29.2%). In many instances, a single measure was studied reported more than once leading to a total of 306 total measurements. Among total measures, measures of availability (n=120, 35.7%) were disproportionality over-represented while measures of affordability were under-represented (n=34, 10.1%).
Unique and total number of access measure categorised by access type
Availability
Unique measures of availability, defined as the relationship of the volume and type of existing services to the clients’ volume and types of needs, totalled 40 (29.2%; table 3). Total measures of availability were studied most often (n=120, 35.7%). Of the unique availability measures, most (n=29, 72.5%, table 4) focused on receiving care. Measurements on receiving care often measured the presence or lack of basic emergency health facilities and resources relevant to emergency care. There was heterogeneity when describing resource service availability, such as the availability of emergency radiologic services (eg, CT and MRI) and emergency laboratory service (eg, blood smears for malaria). Measures owing to the presence or absence of clinical providers with qualifications relevant to emergency care were described in 9 of the 75 studies (12.0%).
Unique access measures categorised by type and delays in care
Accessibility
Unique measures of accessibility—the location of supply and the location of clients—totalled 19 (13.9%), with a disproportionate number of measures studied more than once, leading to 66 total measurements (19.6%). The majority of the unique measures of accessibility corresponded to the process of reaching care (n=13, 68.4%) with most measures on the distance or time to a health service (n=11, 64.7%). Among the 13 studies reporting time, travel times to emergency care ranged from 5 min to 2 hours. The range of distances to health facilities demonstrated similar variability, though most (n=13) measurements were in kilometres. An additional study (n=1) reported on the percentage of the population living within a given distance or time, while other studies (n=4) reported on a range of distances or times to specific EU care (eg, trauma, referral, cardiac). Other qualitative barriers to accessibility were also provided, including the effects of terrain, weather and road quality.
Accommodation
Accommodation measures are those that assess the manner in which emergency care resources are organised to accept patients. Measures of accommodation made up the greatest number of unique measures (n=42, 30.7%), but they were rarely studied more than once (total n=62, 19.6%). Adequacy of child care, concerns over personal safety and difficulties in getting through to prehospital providers were described as significant barriers in the process of seeking emergency care. The majority of unique measures on accommodation dealt with the process of receiving care (n=25, 59.5%). Among measures categorised as receiving care, facility-based measures (n=11, 44.0%) included measures of provider timeliness and availability, provider training, overcrowding and protocols for care. Among the unique measures of accommodation, 4 (8.9%) described the use of standardised protocols (3 related to prehospital care and 1 on facility-based care).
Affordability
Measures of affordability or assessing the cost of services relative to a patient or caregivers finances, were the least studied. While 17 (12.4%) unique measures were similar to the numbers for accessibility and acceptance, measures were rarely studied more than once (n=34, 10.1%). Of the unique metrics reported, most reported on different aspects of the cost of transportation in reaching care (n=8, 47.1%) and the cost of receiving treatment (n=5, 29.4%). Types of costs varied, including the cost of an ambulance ride, cost of deposit before treatment and total hospital bills. A single study described the lack of emergency care affordability based on lost wages from missing work.
Acceptability
Acceptability measures uncovered how well patient’s attitudes around emergency care matched those of providers or systems. Seventeen (12.4%) unique measures of acceptability were described in the literature. The majority were related to the process of care seeking (n=11, 64.7%). Measures largely described patient’s understanding, acceptability, willingness and fears in activating and navigating emergency care systems.
Awareness
Lastly, some have argued for inclusion of awareness as a sixth category of access. There were five unique measures of awareness, which largely overlapped with the previous five other categories, most specifically acceptability. These five measures were reported a total of 18 times.
Access measures by frameworks of emergency care
Individual metrics were also mapped to the Three Delay model, and categorised as either, seeking, reaching or receiving care (table 4). Unique measures of seeking care (N=22, 16.1%) largely dealt with prefacility care and included individual thought processes, the sociocultural forces underlying care seeking behaviour or systematic structural barriers to seeking care. Measures of reaching emergency care (N=46, 33.6%) largely measured the adequacy of out of hospital care, including the presence, number and proportion of ambulances to population, the time from community to care, the cost of ambulance services and distribution and systems of ambulance-based care. The majority of unique access measures described the processes of receiving care (n=69, 50.4%). Most measures dealt with the availability of facility-based care services.
Measures were also mapped to the WHO ECSF (table 5). The WHO Framework ‘captures essential emergency care functions at the scene of injury or illness, during transport, and through to emergency unit and early inpatient care’.16 Roughly equal proportions of measures were focused on prehospital care—inclusive of care at the scene and during transport to a facility (n=76, 55.5%) and facility-based emergency care (n=57, 41.6%). However, given the largely linear nature of the framework, a total of 4 (2.9%) unique measures could not be defined by this framework and were neither specific to prehospital nor facility-based care. The majority of out of hospital care measures focused on the transfer process (n=45 of 76, 59.2%), while most facility-based measures dealt with EU-based care (n=51 of 57, 89.5%). None of the included manuscripts measured EU disposition or elements of early inpatient care.
Unique number of access measures as defined by the WHO ECSF by access type
Discussion
Increased global access to quality emergency care has the potential to reduce mortality associated with non-communicable illness and trauma as well as infectious disease and pregnancy related complications.9–12 Analysis of emergency care access measures in detail elucidates gaps in health systems—made worse by the COVID-19 pandemic—that can guide strategies to address existing inequities in care. To date, this is the first review of access measures specific to emergency care in LMICs.
This review revealed several common themes. The majority of unique emergency care access measures focus on availability and accommodation, but total measures of accessibility appear to be more frequently described in the literature. This has led to the disproportionate emphasis on distance and time to a health facility as demonstrative of emergency care access. In reality, on arrival to a health facility with an emergency condition, most patients are met with limited, ineffective or non-existent emergency care provision.
Relative to other categories of access reviewed, measures of affordability were the least studied in the literature. These measures often lacked information to contextualise data relative to the gross domestic product of the study population’s cost of living. Cost is known to play a significant role in patient’s overall healthcare access in all health systems, not just LMICs.33 Costs associated with emergency health services are known to vary widely across health systems regardless of a country’s gross domestic product (GDP).34 35 Moreover, cost-effectiveness is a widely used method to inform resource allocation, yet evidence to better understand health inequity in all its forms, should include additional efforts to study the cost-effectiveness of emergency care interventions and emergency care systems in LMICs. Measures of access included in this study included both direct (user fees, medication costs, laboratory and imaging tests) and indirect (lost wages, travel costs). Further consensus-led efforts to determine measures most important for system comparison are necessary.
In 2018, the World Health Assembly passed resolution 72.16. ensuring the role of emergency care in all health systems.16 The WHO ECSF sought to provide further context to health policy-makers on the role of emergency care systems in ensuring universal health coverage.16 While prehospital and facility-based measures of access were equally represented on the literature, though significant gaps remained in both domains. Among prehospital care, most measures focused on the transfer process, with less focus on dispatch and provider response. Several areas of this framework had no associated measures described in the literature.
According to the ECSF considerably few studies described measures related to the emergency unit (EU) reception process (eg, registration, screening and triage) or the transfer of care between prehospital and facility-based providers. In addition, no measures described the process of EU disposition or transfer of care to the inpatient ward. Though disposition, transfer, referrals and transition of care from one provider to another are often cited as times of higher risk to patients, measures of this risk were not adequately described in this study.36 Several WHO initiatives have sought to strengthen EU quality globally. Future efforts should seek to define and refine a core set of measures specific to emergency care access to aid in the monitoring and evaluation of those efforts. The further validation of a core set of measures with minimum standards across low-income, middle-income and high-income contexts can help to further increase access to high quality emergency care and the expansion of universal health coverage.
Limitations
This study makes an initial attempt to describe measures of access to emergency care, but it is restricted in scope and possesses several limitations. First, this study is limited to English language articles only and does not include articles in other languages widely spoken in many LMICs, including French, Portuguese and Arabic. Second, while a grey literature review was conducted, we are likely missing measures in use by health facilities, global health organisations and health ministries. Further attempts at key informant interviews or focus groups with those in LMICs, undoubtably would uncover other measures, but were beyond the scope of this review. Third, given the limitations in study data, there was no attempt made to rank-order measures based on feasibility, nor the degree to which they correspond to specific patient outcomes. We recognise that not all measures have equal utility, with some better reflecting access to care issues and serving as more significant correlates of patient outcome. Fourth, though the actual corresponding outcome measures were collected (and described in online supplemental eTable 2), given the heterogeneity of measures and limitations of the search strategy, we were unable to provide reference (or minimum) standards for the access measures described. Future efforts hope to describe further the actual measurements. Other fields have attempted, at times with similar difficulty, to establish reference standards (eg, the Lancet Commission on Global Surgery has recommended a maximum 2-hour travel time to surgical services, while similar measures of time to surgery remain controversial).37 38 However, very few consensus derived standards exist for measuring access to emergency care.39 This lack of consensus makes further facility, regional, and national comparisons difficult and limits effective understanding of care. Similar to previous consensus work on measures of emergency care quality in LMICs, future efforts should aim to define a core list of indicators of access to emergency care.19 Lastly, risk of bias assessment was not performed given the descriptive nature of most studies. Other methodologic and search strategy sought to limit bias in the initial selection of articles.
Conclusions
Increasing access to quality emergency care is a key step in strengthening heath systems in LMICs. This scoping review demonstrates that while existing literature examines a wide breadth of access metrics, many gaps remain in our understanding of emergency care access in LMICs. As researchers continue to examine access and barriers to emergency care, special attention should be paid to those dimensions of access less commonly examined, such as affordability. Standardised, consensus-based measures of emergency care access in line with the ECSF should be developed to allow for more universal comparisons of healthcare functions.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
As a scoping review, this manuscript does not involve human subjects and is exempt from ethics review based on the corresponding author’s IRB.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @CoreyBBills
Contributors CBB, EJCH and SH contributed to the conception and design of the work. SH and JD contributed to data collection and review. SH and CBB contributed to data analysis and interpretation and drafting of the article. MCB, MR and EJCH contributed to critical revisions of the article. All named authors have approved of the version to be published and agreed to be accountable for all aspects of the work. CBB is the guarantor and accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.