Article Text

Abstract
Objectives There is significant burden on caregivers of patients with amyotrophic lateral sclerosis (ALS). However, only a few studies have focused on caregivers, and traditional research methods have obvious shortcomings in dealing with multiple influencing factors. This study was designed to explore influencing factors on caregiver burden among ALS patients and their caregivers from a new perspective.
Design Cross-sectional study.
Setting The data were collected at an affiliated hospital in Guangzhou, Guangdong, China.
Participants Fifty-seven pairs of patients with ALS and their caregivers were investigated by standardised questionnaires.
Main outcome measures This study primarily assessed the influencing factor of caregiver burden including age, gender, education level, economic status, anxiety, depression, social support, fatigue, sleep quality and stage of disease through data mining. Statistical analysis was performed using SPSS 24.0, and least absolute shrinkage and selection operator (LASSO) regression model was established by Python 3.8.1 to minimise the effect of multicollinearity.
Results According to LASSO regression model, we found 10 variables had weights. Among them, Milano-Torinos (MITOS) stage (0–1) had the highest weight (−12.235), followed by younger age group (−3.198), lower-educated group (2.136), fatigue (1.687) and social support (-0.455). Variables including sleep quality, anxiety, depression and sex (male) had moderate weights in this model. Economic status (common), economic status (better), household (city), household (village), educational level (high), sex (female), age (older) and MITOS stage (2–4) had a weight of zero.
Conclusions Our study demonstrates that the severity of ALS patients is the most influencing factor in caregiver burden. Caregivers of ALS patients may suffer less from caregiver burden when the patients are less severe, and the caregivers are younger. Low educational status could increase caregiver burden. Caregiver burden is positively correlated with the degree of fatigue and negatively correlated with social support. Hopefully, more attention should be paid to caregivers of ALS, and effective interventions can be developed to relieve this burden.
- ALS
- caregiver burden
- LASSO
- social support
- MITOS
- fatigue
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This was the first time we study influencing factors on caregiver burden among amyotrophic lateral sclerosis patients and their caregivers through data mining based on least absolute shrinkage and selection operator regression.
The research method solves the problem of small sample size and multicollinearity among independent variables.
Different kinds of continuous variables and categorical variables were involved in the study.
This was a study conducted in south-eastern China, which may only represent a part of the Chinese population.
Our analysis did not include intervention effects with quantified coping strategies in a prospective study.
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease with progressive muscle weakness, dysarthria, dyspnoea, dysphagia and other associated symptoms which prevent patients from taking care of themselves. Patients become increasingly dependent on their partners, family members and other relatives for increasing support and assistance. For one thing, the high cost of medical care, drugs and other supportive services exert huge pressure on families with ALS patients. Moreover, the influence on family in caregiving of patients with ALS is great.1 2 The role of caregivers is critical because their health and well-being are not only important for patients.3 4 Moreover, as the disease progresses, patients will suffer from worsening health and diminishing quality of life. Thus, as the disease progresses, the concomitant psychological distress and mental stress of informal caregivers of ALS increase significantly.5 This phenomenon has also been observed in other neurodegenerative diseases.6 7 Kim et al found a negative correlation between the time spent in caregiving and quality of life of caregivers.8 In Burke’s study, patients’ cognitive and behavioural status is of great importance as mediators of caregiver burden.9 While these studies have demonstrated factors that were associated with an increasing burden for caregivers, we only found a few studies that have focused on influencing factors of caregivers, such as physical health, psychological symptoms, social background, social support and the patients’ condition, and most of them were designed as cross-sectional studies or case-control studies.10–15 Also, knowledge about the action of interventions in relieving caregiver burden is still limited.
This study aimed to determine the effect of factors that influence caregivers’ burden and physical and mental health through data mining based on least absolute shrinkage and selection operator (LASSO) regression model. Hopefully, effective interventions can be developed to improve the health status of caregivers and help relieve caregiver burden.
Materials and methods
Resource of data and participants
Caregivers of patients registered at the First affiliated hospital of Sun Yat-sen University (FAH-SYSU) from August 2015 to February 2017 and with a patient diagnosis of ALS according to the revised El Escorial criteria were recruited in the study. As this cross-sectional study was an analysis of existing data, which did not involve patients’ or caregivers’ diagnosis and treatment, no ethics approval was required from the ethics committee of FAH-SYSU. Even though, participants enrolled have been fully informed and consent was obtained. The informed consent claimed that both the patients and their caregivers knew and agreed that their medical records were used in the study anonymously. Healthy caregivers with at least 3 months’ caregiving experience were included in the study, and caregivers were restricted to relatives such as spouses, parents, children and siblings of the patients. Informal, casual or multiple caregivers and those with confirmed physical and mental problems were excluded. Patients who had rapid deterioration since diagnosis or with bulbar/spinal/respiratory breakdown were excluded from the sample.
This study primarily assessed the influencing factor of caregiver burden including age, gender, education level, economic status, anxiety, depression, social support, fatigue, sleep quality, as well as the duration and stage of disease (Milano-Torinos (MITOS) stage). The quantitative questionnaires of standardised design assessed caregiver burden on different dimensions. Standardised scales were used for the caregivers, listed in the following section. In total, 60 caregivers of ALS patients were selected for the survey through internationally accepted questionnaires. Among all the 60 questionnaires sent out to the caregivers, 57 valid responses were received, with a valid rate of 95%.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Assessment measures and data collection
Patients’ status
Disease duration was measured by months. Disease severity was mainly measured by the clinical staging system of MITOS.16 According to this staging system, patients with ALS are categorised as follows: stage 0, functional involvement but no loss of independence in any domain; stages 1–4, which refer to the number of domains in which independence was lost, for example, movement, swallowing, communicating and/or breathing; and stage 5, death.
Caregiver burden
Zarit Burden Interview (ZBI) was used to evaluate caregiver burden.17 18 ZBI consists of a self-administered 22-item questionnaire, including caregivers’ psychological health, finances, emotional well-being, social and family life, and degree of control over their life. Total scores range between 0 and 88.
Social support
The Social Support Rating Scale (SSRS) is a brief questionnaire designed by Xiao Shuiyuan in 1986–1993, which mainly reflects social support and satisfaction with social support from the respondents.19
Physical and mental health of caregivers
The sleep quality of caregivers was assessed using the Pittsburgh Sleep Quality Index (PSQI).19 Fatigue scale-14 (FS-14) was used to measure the severity of physical and mental fatigue and its effect on a person’s activities and lifestyle.20 Anxiety and depression status were evaluated using the Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale-17 (HAMD-17).21 22
Statistics
General characteristics
Statistical analysis was performed using SPSS 24.0 and Python 3.8.1. Descriptive statistics were used for categorical variables. Means with an SD and IQR were used for continuous variables. Bivariate correlations between continuous variables were performed by Pearson correlation analysis. Correlations between caregiver burden and categorical variables were analysed by visualisation analysis. All tests were performed with an alpha value of 0.05.
LASSO
LASSO regression was used to establish a model to predict the relationship between caregiver burden and variables with high multicollinearity. LASSO was a regression technique for variable selection and regularisation to enhance the prediction accuracy and interpretability of the statistical model that it produces. It was a constrained version of ordinary least-squares regression and typically used for regression of a single response variable y on a predictor matrix X, which was widely used in dealing with data situations of low sample size and high dimension, especially when there were both continuous variables and categorical variables in the regression.23
Compared with other linear regression, LASSO was more applicable to analyse complex multicollinear data by adding a penalty equal to the absolute value of the importance of coefficients and minimising insignificant coefficients to zero, thus the high weight variables will be selected. The absolute size of the regression coefficients β was constrained. The higher the penalty, the more regression coefficients were shrunk towards zero. The regularised regression is quite sensitive to the selection of the penalty coefficients.24–26
To appropriately tune the best parameter, the approach was to estimate the performance with different values using cross-validation (CV).27 Compared with other methods, LASSO was fast and accurate with the advantage of avoiding overfitting automatically.
Prediction performance evaluation
The mean square error (MSE) between the predicted value and the actual value was used to evaluate prediction performance. The coefficient of determination R2 was used to reflect the regression fitting effect of the prediction model. The coefficient R2 is defined as (1 - u/v), where u is the regression sum of squares ((y_true - y_pred) ** 2).sum(), and v is the residual sum of squares ((y_true - y_true.mean()) ** 2).sum(). Best possible score is 1.0, and lower values are worse. LASSO best (alpha) parameter was obtained by CV.
The algorithms were implemented using the LASSO CV package of sklearn in Python 3.8.1.
Data processing and dummy variables
In order to incorporate categorical variables and continuous variables into the LASSO regression model, each variable was processed according to the research purpose. Since continuous variable ‘age’ followed a skewed distribution by calculation of skewness and kurtosis, age was categorised into two groups as categorical variables. Categorical variables were reclassified and served as dummy variables to make the regression result with a positively explanative sense.
Dummy coding method represents group membership with dummy variables that take on values 0 and 1, meaning that membership in a particular group is coded one, whereas non-membership in the group is coded zero. When dummy coding is used in the regression analysis, the overall results indicate whether there is a relationship between the dummy variables and the dependent variables.28 The values of the intercept and the regression coefficients of the resulted regression model can be obtained using least squares estimation procedures. The coefficient of multiple determination, R2, for the regression model with dummy variables can be interpreted in terms of the proportion of variance in the dependent variable that is accounted for by the categorical independent variable.29 The regression model from the dummy coding can be written as:
Yij=B0 +  Bj Dij + εij.
Bj Dij + εij.
where:
Yij: the score on the dependent variable for subject i in group j.
B0: the intercept that represents the mean of the group coded 0 on all the dummy variables.
k: the number of categories of the independent variable.
Bj: the regression coefficient associated with the jth group, and it represents the difference between the mean of the group coded 1 on the corresponding dummy variable and the mean of the group coded 0 on all the dummy variables.
Dij: the numerical value assigned to subject i in the jth group.
εij: the error associated with the ith subject in the jth group.
To be specific, categorical variables were recoded with dummy variables, including two dummy variables suggesting age, two dummy variables suggesting MITOS stage, two dummy variables suggesting economic status, two dummy variables suggesting household and two dummy variables suggesting educational level (table 1). The principle of the setting of dummy variables was to equalise numbers between groups and accord with the meaning of each variable value. For example, educational level (low) represented the sum of educational status including illiterate, primary school, middle school and high school, while educational level (high) represented the sum of educational status including junior college, undergraduate and master. Overall, 6 continuous variables together with 12 dummy variables of 6 categorical variables were introduced into the model.
The variable weight of the LASSO regression and description of dummy variables
Results
Descriptive analysis of characteristics of caregivers and ALS patients
The majority of this cohort was two-thirds female caregivers (38, 66.7%), and the other one-third were male caregivers (19, 33.3%). The mean age of all the caregivers was 45.32±13.74 years (IQR: 33.5–56.5), ranging from 22 to 72 years. The average disease course was 28.98±15.36 months (IQR: 18–36), with the longest being 60 months and the shortest being 6 months. The average score of caregiver burden scale was 39.28±17.11 (IQR: 25–55). The average scores of PSQI and FS-14 were 7.89±4.57 (IQR: 4–10) and 6.58±3.60 (IQR: 4–9), respectively. The average HAMA scores of patients were 10.70±6.62 (IQR: 5–15). The average HAMD scores of patients were 10.16±8.78 (IQR: 4–14.5). The mean score of the SSRS was 40.18±7.47 (IQR: 33.5–46). Forty caregivers were considered ‘anxious’ to different degrees, and the number of possible, definite, obvious and severe anxiety status caregivers were 20, 15, 4 and 1, respectively. Similarly, 27 caregivers were considered ‘depressed’, and the number of possible, moderate and severe depression status caregivers were 16, 10 and 1, respectively. For categorical variables, the number of patients with MITOS from stage 0 to stage 4 was 10, 16, 20, 4 and 7, respectively. Most of the caregivers were junior high school graduates (17, 29.8%). Overall, 34 participants (59.6%) had an education level of at least high school, of which two held a master’s degree. Urban dwellers constituted a proportion of 56.1% of all the caregivers, while the rest of the individuals were from suburban or rural areas. Economic status varied from general to good condition among the participants (table 2).
Demographic features of caregivers
Analysis of correlations between continuous variables
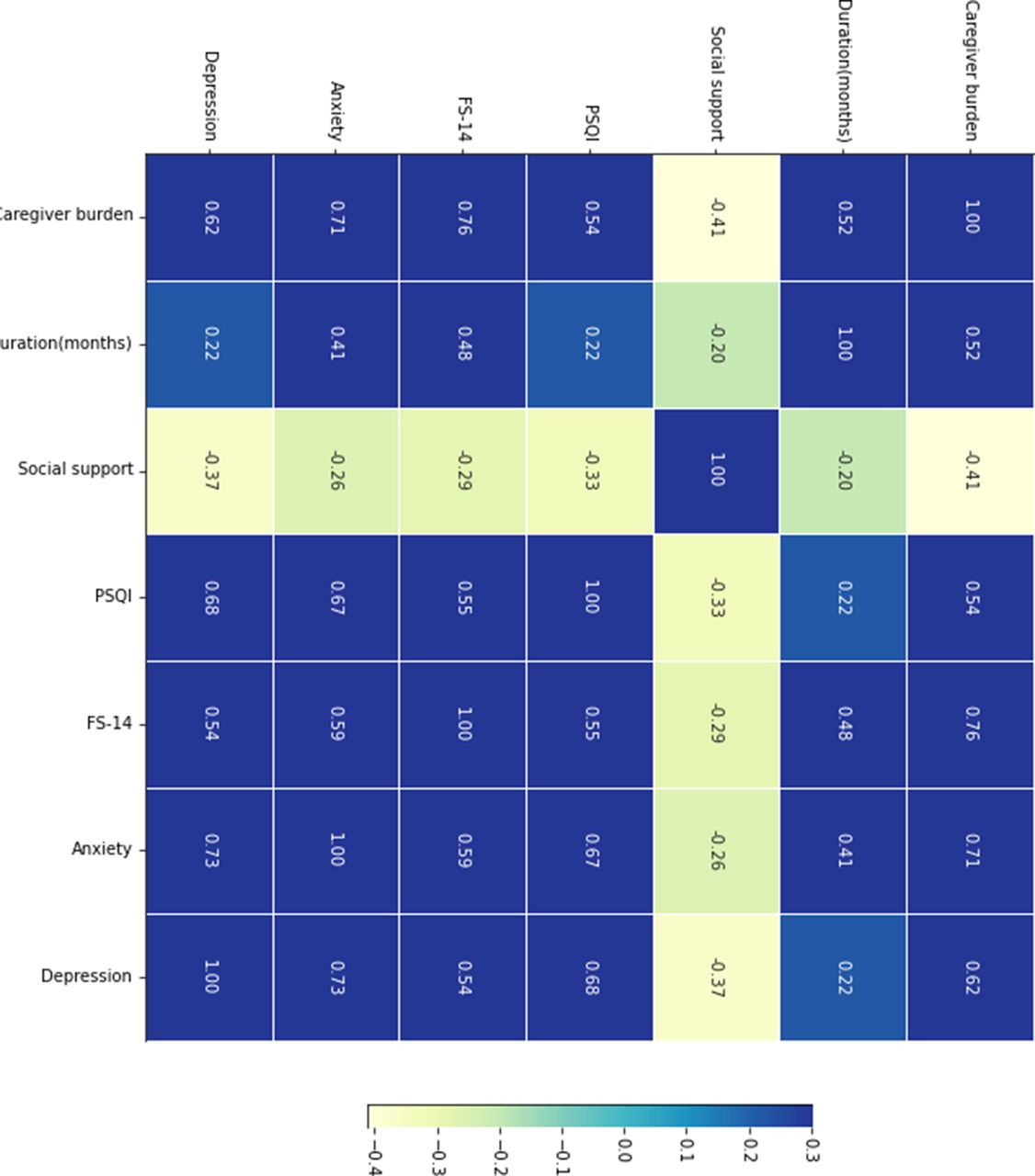
Correlations between continuous variables were demonstrated with heatmap chart shown in figure 1. According to Spearman correlation analysis, positive correlations were seen between caregiver burden and independent variables including duration of disease, PSQI scores, degree of fatigue, anxiety and depression (r=0.52, 0.54, 0.76, 0.71, 0.62, p<0.05), while a negative correlation was noted between caregiver burden and social support (r=−0.41, p<0.05). Interestingly, a slight negative correlation was noticed between social support and PSQI scores, degree of fatigue and depression (r=−0.33,–0.29, −0.37, p<0.05), indicating that social support could be a protective factor. Strong pairwise positive correlations were seen among PSQI scores, degree of fatigue, anxiety and depression (p<0.05).

Correlations among caregiver burden and continuous variables.
Analysis of correlations between caregiver burden and categorical variables
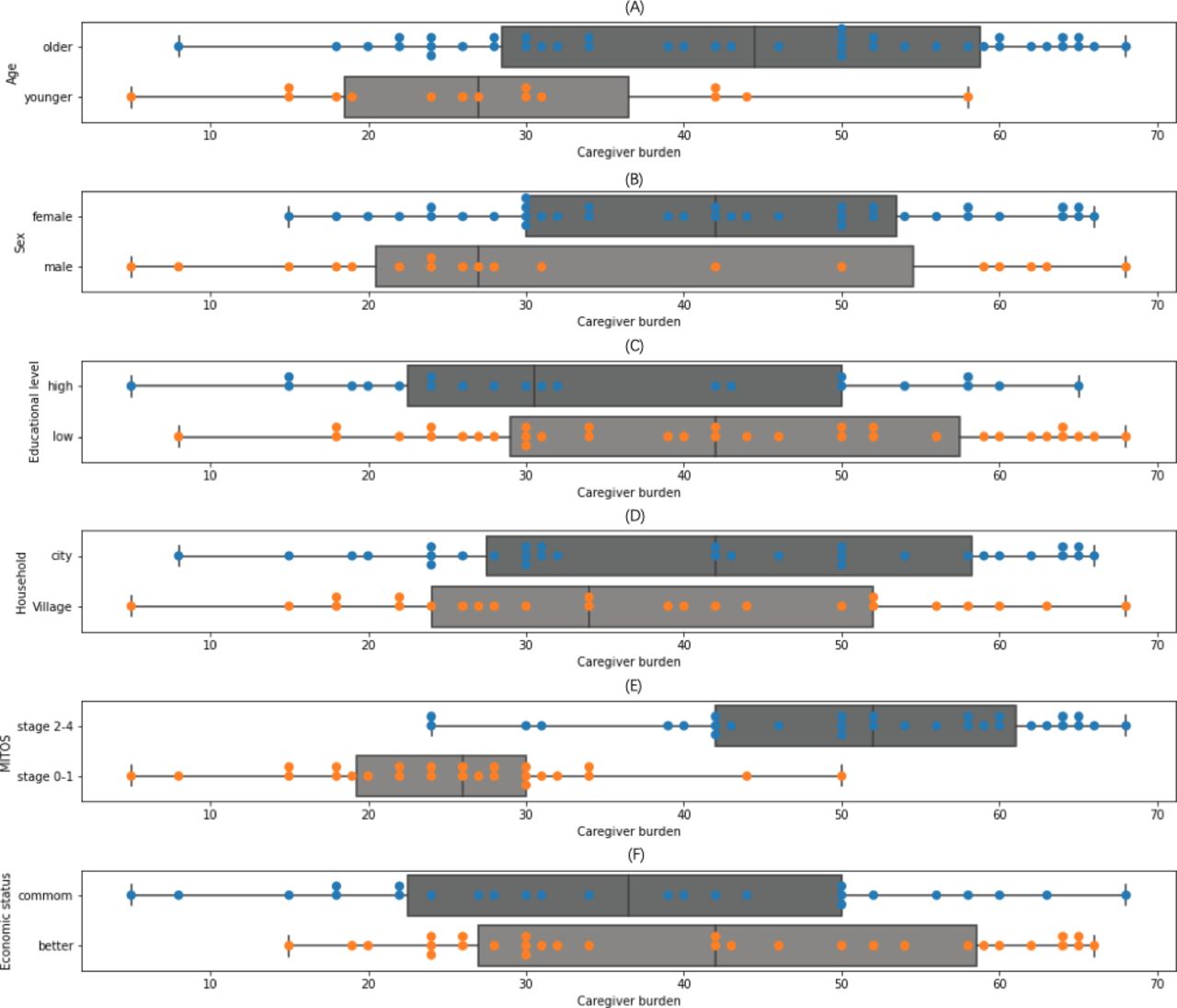
Correlations between caregiver burden and categorical variables were shown as visualisations (figure 2). We used layered data processing to rearrange categorical variables and convert them into dummy variables. The principle of the setting of dummy variables was to equalise numbers between groups. The descriptions of each dummy variable were shown in Table 1. Figure 2 (A) showed that there was a difference in caregiver burden between younger and older patients. Also, an obvious disparity in caregiver burden was seen between group MITOS stage (0–1) and group MITOS stage (2–4), suggesting that patients with ALS with severer symptoms created higher caregiver burden (figure 2 (E)).

Correlations between caregiver burden and categorical variables.
Model construction and evaluation by LASSO regression
Variable selection
The values of each categorical attribute were converted into dummy variables to build a regression model. With caregiver burden as the dependent variable and duration, PSQI, FS-14, anxiety, depression, social support, sex (male), sex (female), age (younger), age (older), MITOS stage (0–1), MITOS stage (2–4), economic status (common), economic status (better), household (village), household (city), educational level (low) and educational level (high) as independent variables, a regression model with multiple dummy variables was constructed shown in table 1.
In the LASSO model, we found 10 variables had weights. Among them, MITOS stage (0–1) had the highest weight (−12.235), followed by younger age group (−3.198), lower-educated group (2.136), fatigue (1.687) and social support (−0.455). Variables including sleep quality, anxiety, depression and sex (male) had moderate weights in this model. Economic status (common), economic status (better), household (city), household (village), educational level (high), sex (female), age (older) and MITOS stage (2–4) had a weight of zero (table 1).
Performance evaluation
In this research, the MSE was selected as the evaluation index, and the best alpha value was obtained through CV. The relationship between the model MSE and alpha is shown in figure 3. When the best penalty factor ‘alpha’= 0.3, the MSE is the smallest, and the LASSO regression model has the highest accuracy. To evaluate prediction performance and fitting effect, the R2 and the MSE of the LASSO regression model were provided. The LASSO score (R2) and the LASSO MSE were 0.831 and 48.496, respectively.

Relationship between α and mean square error.
Liner regression analysis between MITOS stage (0–1), FS-14 and caregiver burden
Variable selection
In the previous section, we learned from the LASSO regression model that MITOS stage (0–1) had the highest weight among categorical variables, while FS-14 had the highest weight among continuous variables. Moreover, the coefficient of MITOS stage (0–1) was significantly higher than other influential dummy variables, and the coefficient of FS-14 was even hundreds of times higher than other continuous variables. Therefore, to further validate the action of the most influential factors in the model, a linear regression model was constructed with caregiver burden as the dependent variable, FS-14 and MITOS stage (0–1) as independent variables.
Performance evaluation
As was shown in figure 4, caregiver burden was positively correlated with FS-14 whenever dummy variable MITOS stage (0–1) was kept in the model or not. On the other hand, when FS-14 remained constant, caregiver burden was significantly higher when dummy variable MITOS stage (0–1) was absent. The distance between the red line and the green line demonstrated the influence of MITOS stage (0–1) on caregiver burden in the model. The intercepts of the linear regression model was 32.125. The LASSO score (R2) and the LASSO MSE were 0.783 and 62.46, respectively. The results were consistent with LASSO regression, suggesting that MITOS stage (0–1) had a strong effect on caregiver burden.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Linear regression between caregiver burden and FS-14.
Discussion
Based on the LASSO model, 10 variables had weights, whereas 5 variables had a greater influence on the model. MITOS stage (0–1) had the highest weight (−12.235), followed by younger age group (–3.198), lower-educated group (2.136), fatigue (1.687) and social support (–0.455). According to the results mentioned above, MITOS stage of patients with ALS was the most important factor influencing caregiver burden, and caregiver burden was significantly lower in patients of ALS with a milder type (MITOS stage 0–1). Interestingly, when another variable duration of disease was brought into the regression model, it did not show any effect on the model, indicating that compared with duration, the severity of patients with ALS had a greater influence on caregiver burden. Sarah K Bublitz found that thick mucus was a highly distressing symptom for both patients and caregivers, which caused a higher degree of bulbar impairment and had a strong impact on their quality of life.30
We draw a conclusion from our study that caregiver burden was positively correlated with the degree of fatigue, while the correlation between caregiver burden and psychological factors such as anxiety and depression was relatively weak. The research of Brizzi et al also showed that the pressure of caregiving in ALS originated from physical symptoms consisting of fatigue, pain, weakness, shortness of breath, difficulty sleeping and speech problems, as well as depression and other mood changes. It was worth noting that fatigue and weakness were the most common symptoms and happened in over 75% of respondents,31 which was in accordance with our study. In our LASSO model, fatigue had higher weights than anxiety, depression and sleep quality. Physical exhaustion was also a typical feature of caregiver burden of other progressive diseases, such as Alzheimer’s disease, Parkinson’s disease and cancer.32–35 Not surprisingly, the feelings of fatigue probably came from long-distance travel to the hospital for treatment, strenuous work in caregiving and loss of rest time. This could well explain our result that younger caregivers suffered less from caregiver burden because they were healthier and more energetic, although they needed to consider time-consuming costs and balance between work and caring. For those younger caregivers, their caring patients were also younger as most of the caregivers were their spouses. This could be another reason that younger caregivers experienced less caregiver burden.
In this study, we found that caregiver burden was negatively correlated with social support, which was consistent with a study in Korea.36 According to the epidemiology of ALS in China, we have a potentially lower incidence and prevalence of ALS than in foreign countries.37 It is still a rare disease, so doctors with less experience may fail to make a correct diagnosis in time and provide appropriate treatment. Even if the diagnosis is clear, effective treatment is not always available to every family due to the high cost of treating the illness. Fortunately, ALS is gradually being covered by health insurance in many provinces of China. The guarantee of a new policy is of great importance in helping relieve the economic burden on caregivers. In addition to economic support, more attention was paid to this group because of increasing caring activities, media reports and social propaganda such as the ‘Ice Bucket Challenge’ all over the country.38 Multiple-centre clinical studies of potential drugs based on animal experiments have also been conducted by a great number of Chinese research teams,39 40 bringing hope and light to patients and caregivers of ALS.
On the other hand, according to our study, social support only had a modest action on caregiver burden. This phenomenon might be caused by insufficient and unbalanced social support in China. Therefore, we speculated that greater social support would bring about less caregiver burden. In some well-developed regions such as Hong Kong, the promotion of multidisciplinary teams provides effective support for the disease, which encourages patients and families of ALS in a highly positive manner.41 Family care is the main strategy for Chinese caregivers to look after ALS patients, and older women and spouses still play an important role in providing family care, while in some other countries, hospital care, nursing home care and community care were made full use of to help alleviate the families’ burden.42 43 The lack of professional caring experience, staff and facilities could affect the efficiency of caring and thus lead to an increasing caregiver burden. Although China has developed rapidly in recent years, there have been obvious differences in medical development and medical investments between eastern and western areas. Little research on ALS has been conducted in western areas, where economic conditions are relatively poor and social support is inadequate. In contrast, modern countries, such as Japan and other European countries, can offer stronger social aid and help systems to ALS families through long-term care insurance, home visit rehabilitation and peer group rehabilitation, suggesting that more social support could be provided to Chinese ALS caregivers to relieve their burden.13 43–46 In addition, medical expenses and end-of-life care were guaranteed in well-developed countries like Japan. Obviously, there is an urgent need for more economical, practical, physical, emotional and spiritual support for caregivers of ALS.
It was surprising to find in our study that educational level influenced caregiver burden. In this study, caregivers of ALS patients were mainly their spouses who were of the same age (50–70 years) and had similar educational levels (middle school) to the patients. A possible explanation is that understanding abilities varied among different caregivers and could be a limitation in low-educated groups. Under the current situation in China, patients were not able to address all their questions in a short period because of the large hospital outpatient quotas. For those caregivers who had a lower educational level, they might feel difficult to quickly understand the key points in caring and follow doctors’ suggestions. In addition, they possibly lacked the abilities to search for information and teach themselves to improve the efficiency of home nursing work.
We investigated the correlations between caregiver burden and caregivers’ mental states, including anxiety, depression, sleep quality index and fatigue. Although we observed a slight correlation between anxiety, depression and caregiver burden, they did not show high weights in the LASSO regression model as we expected. In contrast with other studies conducted in China, mental problems do exist comprehensively in caregivers of ALS, and anxiety and depression were associated closely with each other.10 47 However, the actual condition was more complicated. First, anxiety was not only seen in caregivers of ALS but was also common in regular populations, especially women in their perimenopausal or postmenopausal period.48 Based on the results of an epidemiological study of ALS in the Chinese population, the ratio of male patients to female patients in China was about 1.45–1.98:1,37 which is consistent with our findings. As there were more male patients than female patients in our study, it was speculated that caregivers were mostly women aged 50–70, who had possible risks of being anxious in any event. Traditionally, Chinese women of this age also face the burden of taking care of their grandchildren, making it harder to balance family and their feelings. Second, as there was obvious collinearity among anxiety, depression and quality of sleep, their actual influence on caregiver burden may be overestimated. Even though, non-drug intervention seems to be available and effective for alleviating caregiver burden among caregivers of patients with neuropsychiatric disorders.49 50
From the conclusion obtained above, practical actions should be done for healthcare system to help relieve caregiver burden of ALS. Financial assistance and professional nursing guidance, including long-term care insurance, medical investments, professional online communication groups, home visit rehabilitation, nursing home care, community care, etc may be particularly beneficial as part of ALS care.13 43 45 Regional ALS centres participated by doctors, nurses, psychologists, rehabilitation trainers, social workers, nutritionists, communities, speech trainers, families and researchers are necessary for healthcare system to provide complete and efficient support.10 51 Physical, psychological, emotional and social support are potential effective non-medication interventions to help relieve caregiver burden.42 52–54 Healthcare system should pay more attention to the health status of both the patients and their caregivers proactively. Hopefully, positive and effective strategies can be developed as soon as possible to improve the situation.
Limitations
There were four limitations in this study. The sample size was small and respondents could experience remission, so our observational analysis could have been biased. In addition, we failed to assess intervention effects with quantified coping strategies in a prospective study. Another limitation of the study was the lack of information about the patients and the lack of correlations between patients’ physical or psychological aspects and caregiver burden. Lastly, this was a study conducted in south-eastern China, and caregivers may only represent a part of the Chinese population.
Conclusion
In conclusion, our study demonstrates that the most influencing factor of caregiver burden is the severity of ALS patient. Caregivers of ALS patients may suffer less from caregiver burden when the patients are less severe, and the caregivers are younger. Low educational status could increase caregiver burden. Caregiver burden is positively correlated with the degree of fatigue and negatively correlated with social support.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but As this descriptive study is an analysis of existing data, which does not involve patients’ or caregivers’ diagnosis and treatment, no ethics approval is required from the Ethics Committee of First Affiliated hospital of Sun yat-sen University. exempted this study Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank all patients and their caregivers of ALS for taking part in this research. We gratefully acknowledge the contribution of the doctors, nurses, and other colleagues during the study.
References
Footnotes
Contributors LL: drafting of the manuscript and data analysis. MZ: data collection and follow patients. RH: formal analysis. JL: paper editing and submission. WC: validation. ZP: direct guidance, paper editing and reviewing. XY: project designing and guidance. LL and MZ equally contributed to the paper. XY was the guarantor for the article. All authors commented on previous versions of the manuscript and approved the final manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.