Article Text

Abstract
Objectives To describe and map scientific literature related to alcohol consumption, its determinants, governance, harm and control policies by publication output, author affiliations, funding, countries of study and research themes.
Design Bibliometric analysis using performance analysis and science mapping techniques.
Data sources Scientific articles.
Eligibility criteria Indexed scientific articles published between 1 January 2010 and 31 December 2021 with an English abstract focused on alcohol consumption, its determinants, harms, governance and control policies.
Data extraction and synthesis Searches were run in Web of Science and PubMed. Performance metrics were analysed using descriptive statistics. Keywords were used for science mapping in a deductive approach to cluster articles by five main research themes. The ‘policy response’ theme was further analysed by six subthemes.
Results 4553 articles were included in the analysis. Three out of four articles (3479/4553, 76.4%) were authored solely by authors affiliated with HIC institutions. One in five articles (906/4553, 19.9%) had at least one author affiliated to an institution from an upper-middle-income, middle-income or low-income country context. Governments, followed by research institutions, were the predominant funding source. Half (53.1%) studied a single country and, of these, 77.0% were high-income countries (HICs). Australia, USA and UK were the most studied countries, together accounting for 44.9% (975/2172) of country-specific articles. Thematically, ‘consumption’ was most studied, and ‘alcohol determinants’, least. ‘Policy response’ articles were predominately conducted in HIC contexts.
Conclusions Although the attributable harm of alcohol is known to affect more significantly lower-income and middle-income countries, scientific publications primarily report on HIC contexts by authors from HICs. Research themes reflect known cost-effective policy actions, though skewed towards HICs and a focus on consumption. The implementation of context-specific alcohol control policies requires addressing the determinants of the uneven geographical and thematic distribution of research.
- Health policy
- alcohol
- health promotion
- risk factor
- quantitative research
Data availability statement
The full dataset can be made available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This study is novel in its use of bibliometric data to explore the scientific literature related to alcohol research globally.
This study analyzes publication characteristics (publication output, author affiliation and country of affiliation, funding) and the subjects of study (country/region of study, research themes) in scientific articles on alcohol consumption, its determinants, governance, harms and control policies in the years since the global strategy was adopted.
Exploring the alcohol research landscape exclusively by indexed scientific articles may underestimate the total research productivity globally.
The databases searched (Web of Science and PubMed) consist largely of English-language journals, thereby possibly contributing to selection bias.
Introduction
Eight thousand deaths daily, three million deaths annually1; these are the estimates of alcohol-attributable deaths, attesting to the significant effect of alcohol globally. Alcohol consumption is widespread and broadly accepted, yet has negative implications beyond health, affecting sustainable social and economic development. Notably, the harm caused by drinking is disproportionately greater for individuals with lower socioeconomic status. Alcohol consumption increases inequalities between and within countries and the toll is greater for low-income countries (LICs).2–6
At the same time, in 2019, alcohol consumption around the world, measured in litres of pure alcohol per person of 15 years of age or older, was 5.8 L, a 5% relative decrease from 6.1 L in 2010.7 In parallel to this global trend, significant relative increases in drinking can also be observed in counties of the Western Pacific and South-East Asia. This pattern can be explained by increased affordability in these fast-growing economies, new consumers that traditionally abstained and aggressive marketing campaigns.1 A total of 2.3 billion people, or 43% of the population aged 15 years and older, are considered current drinkers, that is, people who have consumed alcohol in the past 12 months.1 The highest per capita consumption of alcohol is recorded among European countries (eg, Latvia, Czechia). However, consumption is also relatively high in countries of Africa (eg, Uganda, Tanzania), the Americas (eg, Argentina, USA) and the Western Pacific (eg, Australia, Laos).7
In 2010, the global strategy to reduce the harmful use of alcohol8 adopted by the World Health Assembly,9 proposed a variety of policy interventions to curb alcohol consumption and reduce harms. This international commitment to reduce alcohol consumption was further strengthened with the adoption of the Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–202010 and its monitoring framework,11 where alcohol reduction was included as one of the voluntary targets, as well as with the adoption of the 2030 Sustainable Development Goals, specifically target 3.5.12 Most recently, in May 2022, a global action plan for the 2022–2030 period was approved at the Seventy-fifth World Health Assembly.13 The action plan aims to accelerate progress in implementing high-impact interventions for alcohol control.
The production and dissemination of research is critical for effectively designing and implementing policy interventions.14–16 Scientific publications are critical in creating linkages between evidence (knowledge production) and practice (use).17 In various areas of public health research, concerns about diversity in the geography and country income-level of scientific publishing have been raised.18 19 This is especially concerning in low and middle-income countries, as research shows the uptake of evidence can depend on the context in which it has been produced.20 21 In effect, the inequitable production of research poses a significant obstacle for the effective implementation of alcohol control policies, their applicability, translation into the local context and, overall, response to local needs.22 As the global community works to accelerate the implementation of policy interventions to help countries achieve the set alcohol targets, a rigorous overview of the geography and scientific themes of existing research is of paramount importance to guide future research priorities.
This study set out to gain an overview of scientific publications related to alcohol consumption, its determinants, harms, governance and control policies using bibliometric data through a description of their production and publication characterisics and mapping of the subjects studied. Similar studies have been conducted on tobacco23 and addiction in Europe and the USA24 and, in the sphere of alcohol research related to specific regions (eg, Africa)25 and topics (eg, binge-drinking).26 In this study, five key questions for describing and mapping the global scientific literature landscape on alcohol were defined: (1) what is the research output for the period of study? (2) where is the research produced and by whom? (3) what are the predominant research funding sources?, (4) what countries and regions are studied? and (5) what are the predominant research themes?
Methods
Study design
This study adheres to the protocol for conducting bibliometric analysis detailed by Donthu et al.27 It follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines28 for reporting eligibility criteria, search strategy, article screening process, data collection variables and data management plan (online supplemental file 1). Bibliometric analysis techniques were applied to indexed scientific articles identified through a study-specific search strategy. In line with the study’s aims, the approach applied both a performance analysis to describe publication and production-related metrics (publication output, author affiliation and country of affiliation, funding) and science mapping to describe subjects of study (country/region of study, research themes).27 See online supplemental file 1 for an overview of the metrics, data sources and approaches to analysis applied.
Supplemental material
Bibliometric analysis was selected for its rigorous handling of large volumes of scientific data and its potential for statistical and thematic analysis. It also afforded a means to objectively identify knowledge clusters in the field of alcohol, while identifying crucial knowledge gaps.29 The multidisciplinary study team consisted of complementary quantitative/qualitative research, policy and subject matter expertise.
Data sources
Published papers were searched via a keyword search of title/abstract in PubMed and Web of Science, following a study-specific search strategy (online supplemental file 1). The inclusion of other databases was explored, specifically Scientific Electronic Library Online and Russian-language databases e-Library, CyberLeninka and DisserCat. These tests confirmed PubMed and Web of Science together produced the largest output (online supplemental file 2, figure 2.1). Only two databases were selected to reduce possible (human) errors resulting from the consolidation of multiple smaller search outputs and possible duplicates.27
Eligibility criteria and study selection
The topics of articles within scope were defined as scientific publications focusing on alcohol consumption, its determinants, harms, governance and control policies. The search was restricted from 1 January 2010 to 31 December 2021 to reflect the period following the publication of the global strategy to reduce the harmful use of alcohol.8 Only indexed scientific articles were included (ie, no grey literature) to ensure included publications have undergone rigorous peer review,30 though no restrictions were placed on the type of articles (ie, systematic reviews, original research, case studies) and the language of publication. Only English keywords were used for the search. An exploratory analysis showed that including French and Spanish keywords did not significantly increase the results. This can be explained by English language abstracts provided for articles in those languages, thus, non-English articles could still be captured through the search run.
Search strategy
An initial keyword search was developed by deriving possible search terms from the focus of the study. The study team then identified a set of publications expected to be within the study dataset (online supplemental file 3). Multiple keyword searches that resulted in datasets including these publications were tested. Additionally, subsets of 100 randomly chosen articles of different resulting datasets were prepared by two authors (LJ and TD) and manually checked by four others (EB, CF, MN and JET) by title and abstract to confirm the validity of the search strategy. Five rounds of reviews were conducted and between each round, possible keywords triggering false positives were identified and excluded in subsequent searches. Through this iterative process, the keyword search was optimised. The keyword search was considered final when the resulting dataset included the sample of suitable publications and the rate of false positives was deemed acceptable by the study team. The final keywords used are shown in table 1 and reported in full in the detailed search strategy (online supplemental file 1).
Keywords used for searching articles in Web of Science and PubMed
Analysis
All articles that met the inclusion criteria were included in quantitative content analysis using descriptive statistics and deductive thematic analysis.31 The category counts were performed in R. The article details in the dataset included title, author information, keywords, abstract, affiliations, citation count. Further additional features were derived, namely, the author’s country and income group, the country of study (where applicable) and its corresponding income group. Citation counts were obtained from Web of Science and Crossref. The analysis of funding sources was carried out manually for the 100 most-cited papers. Manual analysis was necessary due to incomplete information about funding sources in the raw data extract.
The categorisation of countries into income groups was conducted based on the World Bank 2019 classification as: high-income country (HIC), upper-middle-income country (UMIC), low-middle-income country (LMIC) or LIC.32 Quality checks of the added characteristics (eg, country income level) were completed based on a randomised extract in Microsoft Excel.
To map research themes, an existing causative pathway linking proximal drivers of alcohol consumption with distal health and social outcomes by Martineau et al33 was adapted and applied. Five research themes were derived: determinants (political, economic); consumption (people, amount, frequency); governance (access to alcohol moderated by its acceptability, availability and affordability); policy response (interventions) and alcohol-related harm (consequences of drinking). Each research theme was assigned keywords for mapping the articles (online supplemental file 4). If one of the keywords appeared in the title of an article, the article was assigned to that theme. Articles could be assigned multiple times.
Further analysis of the theme ‘policy response’ was conducted for a detailed analysis of research available and identification of potential blind spots. Six subthemes were defined based on relevant WHO priority action areas, measurement and monitoring: health service response; community action and settings; drink–driving countermeasures; availability; marketing and labelling; tax and price policies (online supplemental file 5).34–36 The areas also align with Martineau et al’s framework. Once categorised, the themes were analysed over time and by income groups. Due to the small sample size when further clustered by these categories, the analysis was simplied to report results by larger clusters of income groups only, combining UMICs, LMICs and LICs. A further analysis to explore the association between authors and research themes was beyond the descriptive mapping aims of the study.
Patient and public involvement
No patients were involved in this study. A network of stakeholders, especially civil society organisations, will be involved in disseminating results.
Results
Publication output
The initial search resulted in a dataset with 5747 articles, from which 1081 duplicates and 113 articles without a publication year or publication year outside of the time span of the analysis were removed. In total, 4553 articles were included in the final dataset (figure 1). Out of these, 513 were sole-authored and 4026 are coauthored publications (no information available for 6 articles, another 8 listed as anonymous). The number of contributing authors was 24 757.

Flow chart for study selection.
Citation information was available for 4508 articles. Out of these, 3530 (78.3%) had prior citations, for a combined total of 59 356. The average number of citations per cited publication was 17, with the most-cited article having 2693 citations (Griswold et al37).
Author affiliation and country of affiliation
Three out of four articles (3479/4553, 76.4%) were authored solely by authors affiliated with HIC institutions. One in five (906/4553, 19.9%) had at least one author from an UMIC, LMIC or LIC. No information on authors was available for 168/4553 articles (3.7%). 1.1% of the articles (51/4553) had at least one author affiliated to an LIC institution, 3.7% (170/4553) to an LMIC institution and 15.9% (725/4553) to an UMIC institution. Out of 149 author affiliations to an LIC institution, 64 (42.9%) were affiliations to one Ethiopian institution. Uganda had the second-highest number of affiliations, with 23 (15.4%).
Trends towards more research being (co)authored by researchers with an UMIC, LMIC or LIC affiliation can be observed over time. Between 2010 and 2013, only 13.9–17.6% (in absolute numbers between 34 and 53 articles in the dataset) were coauthored by someone affiliated with an UMIC, LMIC or LIC institution. This share increased from 15%–20% from 2014 until 2018 to 24%–30% since 2019. The absolute number of articles increased as well. There were at least 117 articles per year coauthored by a researcher affiliated to an UMIC, LMIC or LIC institution since 2019. In 2021, 117 of 483 articles had at least one author affiliated to an UMIC, LMIC or LIC institution.
Authors with affiliation to HIC institutions produced 97% of articles studying HIC. These numbers are considerably lower for the other income groups: 60.2% for UMICs, 51.4% for LMICs and 45.7% for LICs. Half the authors publishing articles on LMICs and LICs were affiliated to institutions from other income groups, predominately to a HIC institution (and therefore also from other countries). For India, only 67.7% of the 49 articles were authored by researchers affiliated with an Indian institution. For Nigeria, 45.3% of the authors of the 18 articles were affiliated with an institution within the country.
Funding sources
Half of the articles (2464/4553, 54%) reported a funding source. Out of 100 most-cited articles sampled, 69% (69/100) had information on funding and 31% (31/100) had no funding information. The 69 articles with funding information had 123 funding sources, equivalent to 1.8 sources per article with funding information. Out of all funding sources information, about half (61/123, 49.6%) were government institutions, predominately from the USA, followed by the UK and Australia. Other funding sources included national and supranational research institutions (25/123, 20.3%), universities (3/123, 2.4%), foundations (17/123, 13.8%) and international organisations such as the WHO (9/123, 7.3%). A total of 9 articles (9/123, 7.3%) disclosed funding from the pharmaceutical industry.
Country and region of study
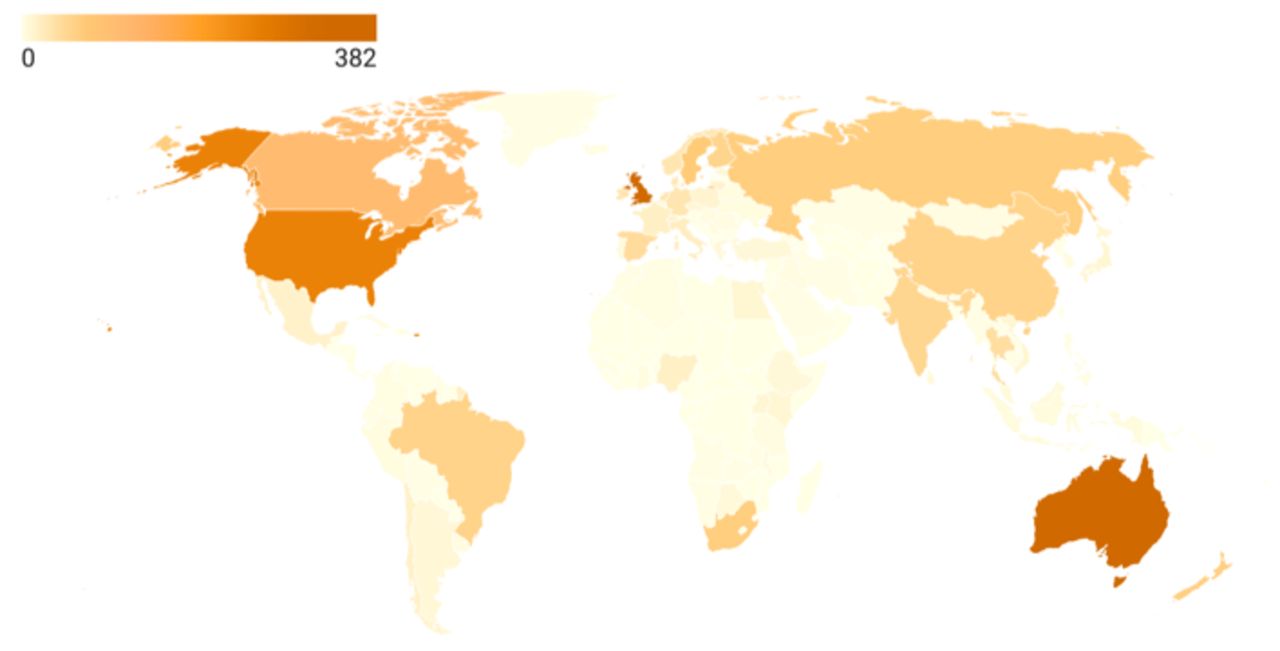
Half of the articles in the dataset (2172/4553, 47.7%) studied a specific country (figure 2). The remainder studied either groups of countries, such as global samples or subregions,38 39 or topics without a specific context which predominately included systematic reviews or other review articles.40 41 Of the country-specific articles, three-quarters studied an HIC (75.5%), while one-quarter studied an UMIC, LMIC or LIC (17.3%, 5.4% and 1.7%, respectively). Nearly half (45%) of country-specific research focused on three HICs: Australia, the UK and the USA. As figure 2 illustrates, there is little or no research on many countries in Africa, the Middle East and Latin America (grey or lightly shaded areas). Of the 20 most studied countries, 19 were either HIC or UMIC, India being the only LMIC (table 2). Only 154 articles (7.2%) focusing on a single country studied an LIC or LMIC, of which 31.8% were on India (49/154 articles).

Distribution of country-specific studies in the dataset.
Top 20 most studied countries in the dataset
Research themes
84.5% of the articles in the dataset were categorised into one of the five main research themes, the remaining 15.5% being assigned to ‘other’. Less than 2% of articles were assigned to four or five main themes. Articles related to the theme ‘alcohol consumption’ were most predominant (39.8%), followed by ‘policy response’ (31%), ‘governance’ (26.9%), ‘alcohol-related harm’ (26.7%) and ‘determinants’ (12.6%) (figure 3).

Distribution of research themes in the dataset by income group. HIC, high-income country; LIC, low-income country; LMIC, low-middle-income; UMIC, upper-middle-income country.
Figure 4 shows that for the theme ‘policy response’, over half of the articles in the dataset (756/1411, 53.5%) had a country of study. The remaining 46.4% (655/1411) of articles either studied multiple countries or studied policy response(s) in general. Across all research themes, there are more articles for HICs than for UMIC, LMIC and LICs combined.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Articles on ‘policy response’: distribution of subthemes by income group. HIC, high-income country; LIC, low-income country; LMIC, low-income middle-income country; UMIC, upper-middle-income country.
The volume of research also varied between theme by country income level. For example, 42.6% of LIC articles are on consumption, 37.9% of LMIC and 38.2% UMIC articles; this share is only 28.4% for HIC. When it comes to evidence that could guide the development of specific policy responses, only 18.5% of (the already smaller number of) scientific publications on LIC are on ‘policy response’; 20.7% for LMIC, 18.5% for UMIC; for HIC, this share is at 26.2% and is a share of a larger total amount.
Figure 4 shows the distribution of the relevant articles across the six subthemes of the policy response research theme. The subtheme ‘drink–driving countermeasures’ is the least frequently studied policy response in the dataset, with only 146 articles focusing on this (10.3% of articles in the theme ‘policy response’ equivalent to 3.2% (146/4553) of all articles in the dataset).
More than 100 articles are available across all subthemes for HIC over 2010 and 2021 aside from drink–driving interventions (n=53). For the UMICs, LMICs and LICs combined, the number of scientific publications varied between 18 and 35 articles per subtheme over the studied period.
Discussion
More than 10 years from the release of the global strategy to reduce the harmful use of alcohol8, attention has turned to accelerating the implementation of its proposed policy options to reduce the harmful consumption of alcohol. This bibliometric analysis has studied publication characteristics (publication output, author affiliation and country of affiliation, funding) and the subjects of study (country/region of study, research themes) in scientific articles on alcohol consumption, its determinants, governance, harms and control policies in the years since the global strategy was adopted. We observe the following main findings.
First, regarding performance (publication) related metrics, specifically the geographical distribution of authors, we note that despite the positive trend towards more researchers from LICs, the overall proportion of authors remains limited. This finding may reflect limitations in local research capacities and the imbalance of power structures, inequitable partnerships and systemic discrimination that has been described by others.42–45 This finding may have several consequences on the potential uptake of available research results. For example, studies have shown that authors with different countries of origin than the country of study may influence the article’s perceived relevance.46 47 Additionally, research produced by a peer is considered more credible and trustworthy to public health decision-makers in LMICs.48 Fit-for-purpose research needs further prioritisation to effectively drive the implementation of alcohol control policies over the next decade. Mentorship schemes for early-career researchers, resources to support submissions of non-native English-speaking authors, and more ambitious expectations for diversity among author teams and editorial boards are some actions that need to be taken.49
Further to the above publication-production-related observation, regarding funding sources, our findings align with others that report a skewing towards institutions in HIC contexts.50 Transparency of funding sources for research is critical in alcohol control policies, as the alcohol industry often works through partnerships or foundations.50 51 There is a long history of lack of disclosure of industry funding by researchers.52 In our analysis of a subset of articles, we concluded for the 100 articles studied that the alcohol industry was not named as a funding source. Nonetheless, we find critical gaps in the reported funding sources in the databases used for this analysis. As greater attention is given to the commercial determinants of health53 and the reported influence of corporations on alcohol-related research,52 54 further standardisation to ensure funding sources are explicitly and consistently stated, such as author details, is needed.
Finally, regarding the subjects of study, the volume of research evidence clustered by research topics is sparse. A similar finding was described by Ghandour et al55 on scientific publications on alcohol consumption in the Arab region, reporting a total of 81 articles across 22 countries in two decades.55 Of importance in our findings is the observation that across research themes and subthemes on ‘policy response’, the little evidence available offers insufficient country-specific insights, particularly among LICs. Across the six policy responses analysed, UMIC, LMIC and LIC contexts were predominately less studied in all instances. In the case of ‘marketing and labelling’ and ‘drink–driving countermeasures’, articles in the dataset were predominately classified as ‘no income group’. This finding suggests that research on these policy measures was primarily reviews or theoretical studies rather than applied, experimental study designs. Redressing this imbalance to increase local and context-based research is an issue of equity and a requirement for realising the acceleration of the effective implementation of policy measures sought.
Based on our findings, we note the following areas as possible priorities for future research. First, country-specific research, in particular in the context of LIC countries, should be prioritised. Importantly, as attention turns to the accelerated implementation of proven policy interventions, country-specific research should focus on further reporting policy responses in practice. Second, the analysis of themes of study found the ‘determinants of alcohol’ as an area that merits prioritisation to redress the comparatively fewer studies in this area to date. Lastly, as an initial study to describe and map the alcohol research landscape, additional research exploring the available bibliometric evidence through networking techniques remains needed and may offer further insights into trends and the relative importance of metrics explored here.
Research limitations
In addition to those inherent to bibliometric studies, the findings should be considered in light of the following limitations. First, similar to other studies, the databases used are dominated by English-language articles which may introduce a possible language bias.56 Ultimately, the two databases choosen resulted from careful consideration and piloting of the search strategy in alternative databases. Second, despite the iterative methods to refine the search strategy, outliers in the dataset may account for 15.5% of articles, reflecting those assigned the category ‘other’ in the thematic analysis. Third, inaccuracies in the assignment of categories to publications in the dataset, such as country of study and research themes, are possible. For example, some publications may cover more than one country and, in these cases, the country of the study was deducted from the first country mentioned in the title or its abstract. Studies covering broader regions were not assigned a country of study. A subset of 200 articles was inspected to gauge the robustness of the analysis. The false positivity rate with respect to the automated retrieval of countries was 6%. Similarly, the assignment of research themes was limited to a keyword search of the title only and may contribute to an under-representation of research themes had the abstract or full text been analysed. For the purposes of the study and its scope, the analysis by title to gauge the predominant research theme was considered sufficient.
Conclusion
Our study confirms a critical geographic imbalance in scientific publications skewed towards HIC contexts. Notably, the geographical distribution of publications does not correspond to countries with higher per capita consumption of alcohol globally; there is a complete absence of LICs among the top twenty most studied countries. A similar finding is observed regarding funding sources and the country of affiliation for authors, though a positive trend for the latter is reported. The research themes are found to relate to alcohol consumption predominately, and of those related to policy responses, these are mainly on health services responses rather than more population-wide and preventive interventions.
With the new global action plan for the current decade brought into effect, intentional investments in scientific research in LIC contexts are needed. Challenges to effectively implementing known, cost-effective and population-wide alcohol control policies are among the key barriers the new action plan sets out to address. Our findings call for country-specific studies, specifically in LIC contexts, and research themes beyond alcohol consumption and care. With the 2030 Sustainable Development Goals on the horizon, investments in fit-for-purpose scientific research on alcohol and alcohol control policies cannot wait.
Data availability statement
The full dataset can be made available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge the contributions and are grateful for and to the following: technical reviews by Ruediger Krech (WHO) and Carina Ferreira-Borges (WHO); support for additional data collection for the funding analysis by Harjeet Sehra (Azim Premji University); and the feedback of peer reviewers Noelle Loconte, Surasak Chaiyasong, and Lim Weng Marc.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LJ, EB, CF, MN, RM and JET designed the study. LJ, CF and TD conducted data collection. LJ, TD, EB, MN, CF, RM and JET contributed the analysis and interpretation of results. LJ prepared a first version of the manuscript. LJ, TD, EB, MN, CF, RM and JET provided feedback and contributed to the revising of the manuscript. LJ, TD, EB, MN, CF, RM and JET approved the final version. JET is guarantor.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.