Article Text

Abstract
Introduction To date, there are no prospective studies evaluating the prevention of recurrent veins by the simultaneous treatment of a sufficient anterior accessory saphenous vein (AASV) in patients undergoing endovenous laser ablation (EVLA) of an insufficient great saphenous vein (GSV). This study will provide important information about the impact of the AASV on the development of recurrent veins after EVLA of the GSV. Additionally, it will be clarified whether patients benefit from a preventive ablation of a sufficient AASV.
Methods and analysis This is a multicentre, prospective, controlled, exploratory clinical study in 1150 patients with a medical indication for EVLA of a refluxing great saphenous vein. Patients will be enrolled into two study groups: in half of the patients EVLA will be performed on the insufficient GSV only. In the other half of the patients EVLA will be performed on the insufficient GSV and additionally on the sufficient AASV. Within seven study visits, patients will be followed-up over a time period of 5 years. Primary study endpoint is the recurrence rate; secondary endpoints include inter alia, complication rate, postoperative pain intensity, quality of life and patient satisfaction.
Ethics and dissemination Before initiation of the study, the protocol was presented and approved by the independent ethics committee of the medical faculty of the University of Heidelberg (Ethics approval number S-596/2018). This study was prospectively registered at the German Clinical Trial Register (https://www.germanctr.de/). Research findings will be disseminated in a peer-reviewed journal and at relevant conferences.
Trial registration number German Clinical Trial Registry (DRKS00015486).
- laser therapy
- surgical dermatology
- vascular surgery
- vascular medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This exploratory study investigates the impact of the anterior accessory saphenous vein on the development of recurrent veins in a prospective controlled setting.
Patients will be assessed under real-life clinical conditions.
Study results will be based on a large sample size with a long follow-up period of 5 years.
Essential patient-related outcome measures (eg, quality of life and response to therapy) are being assessed by validated scores.
Limitations arise from the explorative study design which might limit the generalisability of the results.
Introduction
Chronic venous insufficiency caused by varicose veins is a common disorder.1 Approximately, 50% of the western adult population show stigmata of venous disease and 25% suffer from visible varicose veins.2 3 Venous insufficiency is most often linked to reflux of the great saphenous vein (GSV).4 For a long time, high ligation and stripping (HLS) of the GSV was considered as a standard treatment for vein insufficiency.1 5 Innovative endovenous methods such as endovenous laser ablation (EVLA) are being successfully applied worldwide for many years.4 5 Several randomised controlled trials suggest that the clinical results of EVLA and HLS are comparable.4 6–10 Recurrent varicose veins are known to be a common problem after EVLA and HLS which is defined as a reflux in the treated groin area with or without a persistent GSV stump in duplex examination.11 12 One of the most important factors associated with recurrent veins includes a new secondary reflux of the anterior accessory saphenous vein (AASV) after GSV treatment.12–15 The AASV is a tributary of the saphenofemoral junction and is located lateral to the GSV. In a study by Garner et al, patients were observed over a 3-year period after surgery. Out of 141 groin recurrences, 61 (43%) were due to a persistent AASV and, as such, was the most common cause of recurrent varicose veins encountered in this study.13 Within the REVATA-study a recurrence rate of 6.9% after endoluminal procedure was detected.14 According to the authors, every fourth recurrence was caused by a secondary incompetency of the AASV. One possible explanation of the authors is that once the GSV is ablated, the blood flow from the superficial epigastric vein and pudendal junctions is then directed into the AASV. Due to inherent defects in vein wall or valves, resultant insufficiency occurs. Prior to GSV ablation, refluxing flow preferentially follows the larger diameter of the GSV.14
Hitherto, there is only little known about the possible prevention of recurrent veins by the simultaneous treatment of the sufficient AASV in patients undergoing EVLA of an insufficient GSV.15 Therefore, the preventive EVLA of AASV is currently a much discussed topic and is managed differently by phlebologists. Within this study, this issue will be evaluated for the first time in a prospective controlled setting.
Methods and analysis
Study objectives
The primary objective of this study is to generate data to assess the impact of a synchronous treatment of the AASV for prevention of recurrent varicose veins in patients undergoing EVLA of an insufficient GSV. Recurrent varicose veins are defined as a reflux in the treated groin area with or without a persistent GSV stump in duplex examination. Secondary objectives of this study are, inter alia, to address the complication rate, postoperative pain intensity, duration of absence from work and normal activity, health-related quality of life and disease-specific quality of life and patient satisfaction.
Study design and inclusion/exclusion criteria
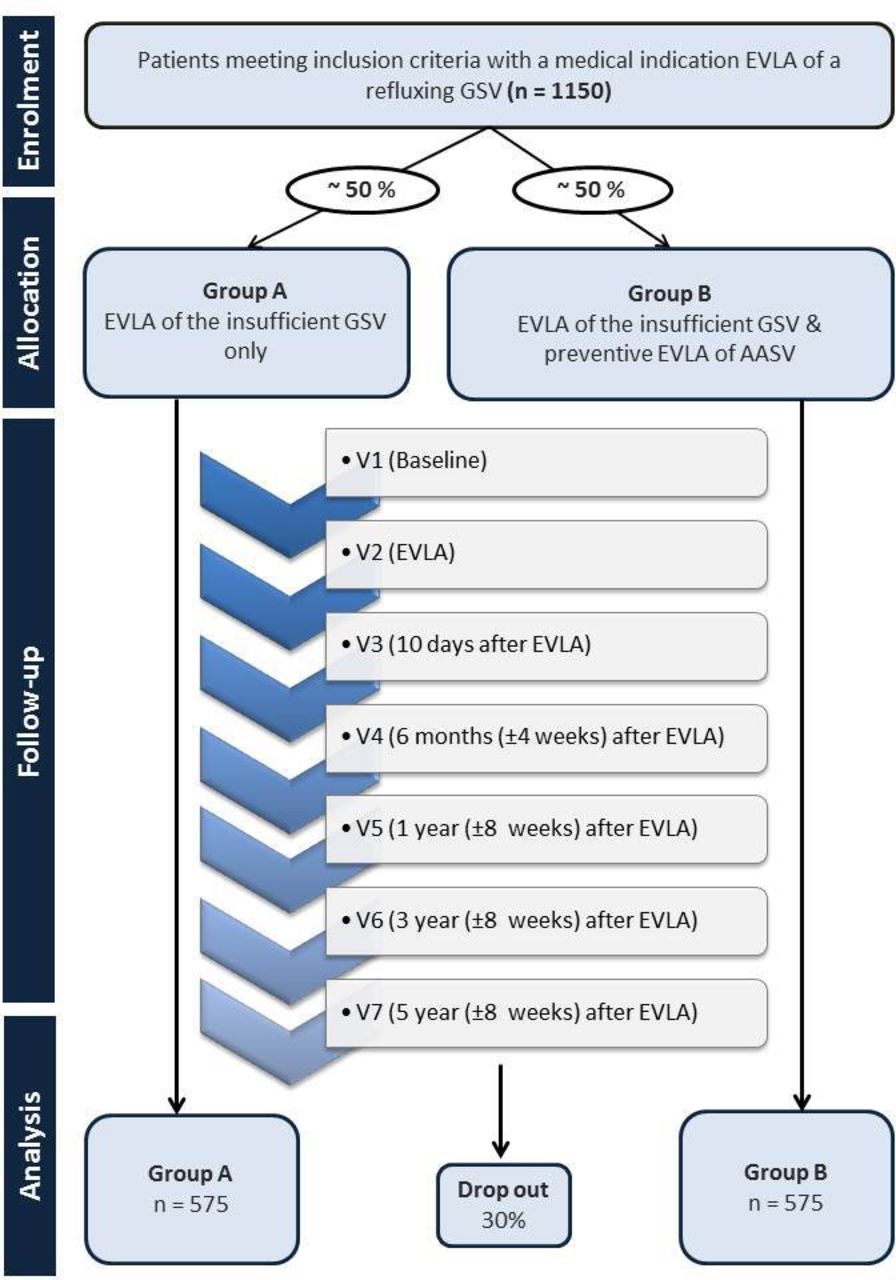
This is a multicentre, prospective, controlled, exploratory clinical study in patients with a medical indication for elective thermal ablation of a refluxing GSV. One thousand one hundred and fifty patients of at least 18 years of age and with a medical indication for elective thermal ablation of a refluxing GSV will be evaluated in this study. Patients with varicose veins and written informed consent will be included in the study. GSV incompetence is defined by a reflux time of >0.5 s on duplex imaging. Patients with an incompetent AASV, a tortuous GSV rendering the vein unsuitable for endovenous treatment, duplication of the saphenous trunk, deep venous incompetence/occlusion or patients that are not able to read, understand or sign the study specific informed consent form (eg, impaired mental state, insufficient knowledge of the German language) or with expected lack of compliance will be excluded from this study. Only study centres were selected that treat a high number of patients with the 1470 nm two-ring radial laser fibre. All recruiting physicians work in a private practice located in Germany. Allocation of the study centres to the two treatment groups was based on the standard practices in each centre for the treatment of refluxing GSV. According to the standard procedure of the respective study centre patients will be enrolled consecutively into two study groups (A/B). Half of the eight study centres will enrol 575 patients into group A and will perform EVLA of the insufficient GSV only. The other half of the study centres will enrol 575 patients into group B and will perform additional EVLA of the AASV (see figure 1).

{kind=link}
Flowchart of the study. AASV, anterior accessory saphenous vein; EVLA, endovenous laser ablation; GSV, great saphenous vein.
Endovenous laser ablation
According to the standard operating procedures of the respective study centre the AASV will be treated simultaneously in patients undergoing EVLA of an insufficient GSV or not. When the AASV is treated simultaneously with the GSV, an explicit informed consent will be obtained concerning this procedure. In all study centres, EVLA is performed with a 1470 nm two-ring radial laser fibre of the same manufacturer at 10 Watts (Biolitec, Jena, Germany). Since it is known that a long residual saphenofemoral stump promotes recurrence, flush ablation of the junction is performed in all individuals in order to minimise stump length (endovenous crossectomy).16 17 In endovenous crossectomy the saphenofemoral junction with the epigastric vein remains open or reopens postoperatively. All other junctional branches which flow into the femoral vein via GSV are immediately closed. AASV is closed via another puncture in a second step. In addition to EVLA, miniphlebectomies and sclerotherapy may be routinely performed in conjunction with EVLA if tributaries are present.
Study visits
In total, there will be seven study visits during the study. The patients will be examined at the time of recruitment (V1), on the day of the procedure/EVLA (V2), until 10 days after EVLA (V3), 6 months (±4 weeks; V4), 1 year (±8 weeks; V5), 3 years (±8 weeks; V6) and 5 years after EVLA (±8 weeks; V7). For evaluation of the primary endpoint, the rate of recurrent varicose veins in general and in particular recurrent veins caused by a new AASV reflux will be obtained after EVLA in V3–V7. The secondary endpoints will be obtained by documentation of the complication rate and duration of absence from work and normal activity after the procedure. The disease-specific quality of life, disease severity and outcome of therapy for venous disease, postoperative pain intensity and patient satisfaction will be evaluated by means of the respective questionnaire in V1–V7 (see figure 1). The following data will be obtained during the respective study visit.
Visit 1 (preoperative baseline visit)
Assessment of exclusion/inclusion criteria, documentation of baseline characteristics and disease severity, performance of clinical and duplex examination (the patients are examined in the standing position and reflux >0.5 s is considered positive. Duration of reflux and the vein diameter (mm) of the GSV at the saphenofemoral junction (and 3/15 cm below) and the length of vein will be documented). Determination of disease severity and disease-specific quality of life.
Visit 2 (EVLA)
Length of treated vein (GSV and AASV), intraoperative complications, postoperative anticoagulation, postoperative compression therapy.
Visit 3–7
Postoperative complications (eg, the presence of ecchymosis, hyperpigmentation, necrosis/burns at the puncture site, deep vein thrombosis or endovenous heat induced thrombosis) and sensory disorders. Treatment success/failure (closed vein or no longer visible), recurrent varicose veins, postoperative pain intensity, duration of absence from work and normal activity, disease-specific quality of life, disease severity and outcome of therapy for venous disease, patient satisfaction.
Data assessment via patient questionnaires
The disease severity and outcome of therapy for venous disease are being assessed via validated Venous Clinical Severity Score.18 Disease-specific quality of life is determined by means of the Aberdeen Varicose Vein Questionnaire which is a validated 13-question survey addressing all elements of varicose vein disease.19 Furthermore, each patient is required to evaluate patient satisfaction with the treatment on a scale of 1–5. By means of a pain intensity score, patients will be asked to evaluate the pain on a scale of 1 (no pain) to 10 (severe pain): A: the greatest pain since the last visit, B: currently experienced pain in the area of the operated limb, C: the current pressure pain, D: the most severe pressure pain since the last visit.
Statistical analysis
As this is the first explorative study investigating the recurrence rate of varicose veins caused by a persistent AASV in patients with a treated refluxing GSV, a formal sample size calculation is neither applicable nor feasible. Nevertheless, a sample size of n=1150 patients is planned to be included as this is feasible within a reasonable period of time. Assuming a drop-out rate of 30%, this leads to a sample size of 800 to be analysed. The information on the rate of varicose veins in general varies strongly in the literature. However, in group A, we expect to obtain a recurrent varicose vein rate of 20% after 3 years. With a sample size of 800, a reduction of 7.4% (from 20% to 12.6%) of recurrent varicose veins can still be detected with a power of 80% and a significance level of 5% using a chi-square test. The primary analysis will be adjusted for covariates which, in general, rather increases the power of the procedure. All endpoints and patient characteristics will be analysed descriptively by tabulation of the measures of the empirical distributions. Depending on the scale level of the variables, either means, SD, medians, and first and third quartiles, as well as minimum and maximum, or absolute and relative frequency will be reported. Descriptive p values of t-tests and χ2 tests for continuous or categorical data will be given, respectively. Furthermore, the associated 95% CIs of the means or rate differences will be provided. If appropriate, graphical methods will be used to visualise the findings. The primary null hypothesis of equal rates in the primary endpoint (varicose veins, yes/no per person) after 3 years (V6) in both groups will be tested using a logistic regression model. The group variable, age, body mass index and gender will be included as predictors. For each factor, the OR with 95% CIs and p values will be reported. Missing values will be imputed using a multiple imputation approach. A Fully Conditional Specification method will be applied. This is a commonly used method and appropriate for an arbitrary structure of missing values which is the most general form of a missing data pattern. All variables that are used in the primary model will be included in the imputation models. The same logistic regression model will be fit when analysing the primary endpoint at the other time points (V3–V5 and V7). For all other endpoints, (generalised) regression models will be applied as appropriate including the same predictors as in the primary analysis. Furthermore, longitudinal (mixed) regression models for all endpoints will be applied including all time points into one model. A random intercept (for patients) will be included and different correlation structures will be applied (in particular, an unstructured covariance matrix and an auto-correlation structure). Again, the same predictors as before will be included as fixed factors and ORs with 95% CIs and p values will be reported.
Study organisation and data management
Study coordination and data management is performed by the Department of Dermatology, University of Heidelberg. Data collection is done via case report forms. Statistical analysis will be performed by the Institute of Medical Biometry. All study procedures will be done according to approved standard operating procedures which are based on International Conference on Harmonization-Good Clinical Practice (GCP) guidelines (E6), the German implementation of GCP and the current laws.
Ethical considerations, dissemination plan and regulatory obligations
The study is conducted in accordance with the Declaration of Helsinki principles (2013), applicable local government regulations and independent Ethics Committee policies and procedures. Before initiation of the study, the protocol was presented and approved by the independent ethics committee of the medical faculty of the University of Heidelberg (Ethics approval number S-596/2018). This study was prospectively registered at the German Clinical Trial Register (https://www.germanctr.de/). Research findings will be disseminated in a peer-reviewed journal and at relevant conferences.
Patient and public involvement
No patient involved.
Recruitment and status of the study
Ethical approval was granted in October 2018. First enrolment was in February 2019. The estimated time required for recruitment is 48 months. The total duration of the study is expected to be 108 months, including statistical analysis.
Discussion
To date, there are no controlled prospective studies evaluating the impact of a simultaneous EVLA of AASV for prevention of a secondary reflux in patients undergoing EVLA of an insufficient GSV. Therefore, it remains unclear whether patients benefit from this procedure. This exploratory study addresses this important open question for the first time in a prospective controlled setting under real-life clinical conditions based on a relatively large sample size. Additionally, essential patient-related outcome measures (eg, quality of life and response to therapy) are being assessed by validated scores. Limitations arise from the explorative study design which might limit the generalisability of the results. Nevertheless, data provided by this study makes it possible to plan and perform a randomised controlled future trial with a formal sample size calculation.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors Conception and design: CF, KH, TH, TM, H-CW, TW, MS, FP, LU. Analysis and interpretation: CF, CD, KH, TH, LU. Data collection: CF, CD, KH, TM, H-CW, PZ, JV, TW, GL, LM, MS, FP, LU, TH. Writing the article: CF, CD, KH, TM, H-CW, PZ, JV, TW, GL, LM, MS, LU, TH. Critical revision of the article: CF, CD, KH, TM, H-CW, PZ, JV, TW, GL, LM, MS, FP, LU, TH. Final approval of the article: CF, CD, KH, TM, H-CW, PZ, JV, TW, GL, LM, MS, FP, LU, TH. Overall responsibility: CF, KH, LU, TH. All authors read and approved the final manuscript.
Funding This study received a research grant by the German Society of Phlebology (Forschungsförderung durch die Deutsche Gesellschaft für Phlebologie – DGP; grant number: N/A).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.