Article Text

Abstract
Objectives To identify factors associated with kinesiophobia (fear of movement) after cardiac hospitalisation and to assess the impact of kinesiophobia on cardiac rehabilitation (CR) initiation.
Design Prospective cohort study.
Setting Academic Medical Centre, Department of Cardiology.
Participants We performed a prospective cohort study in cardiac patients recruited at hospital discharge. In total, 149 patients (78.5% male) with a median age of 65 years were included, of which 82 (59%) were referred for CR.
Primary and secondary outcome measures We assessed kinesiophobia with the Tampa Scale for Kinesiophobia (TSK). For this study, the total score was used (range 13–52). We assessed baseline factors (demographics, cardiac disease history, questionnaire data on anxiety, biopsychosocial complexity and self-efficacy) associated with kinesiophobia using linear regression with backward elimination. For linear regression, the standardised beta (β) was reported. Prospectively, the impact of kinesiophobia on probability of CR initiation, in the first 3 months after hospital discharge (subsample referred for CR), was assessed with logistic regression. For logistic regression, the OR was reported.
Results Moderate and severe levels of kinesiophobia were found in 22.8%. In the total sample, kinesiophobia was associated with cardiac anxiety (β=0.33, 95% CI: 0.19 to 0.48), social complexity (β=0.23, 95% CI: 0.06 to 0.39) and higher education (β=−0.18, 95% CI: −0.34 to −0.02). In those referred for CR, kinesiophobia was negatively associated with self-efficacy (β=−0.29, 95% CI: −0.47 to −0.12) and positively with cardiac anxiety (β=0.43, 95% CI: 0.24 to 0.62). Kinesiophobia decreased the probability of CR initiation (ORRange13–52 points=0.92, 95% CI: 0.85 to 0.99).
Conclusion In patients hospitalised for cardiovascular disease, kinesiophobia is associated with cardiac anxiety, social complexity, educational level and self-efficacy. Kinesiophobia decreased the likelihood of CR initiation with 8% per point on the TSK.
- REHABILITATION MEDICINE
- Anxiety disorders
- Organisation of health services
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request. Requests for analyses of data from this study should be directed to PK (p.keessen@hva.nl).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Structural equation modelling was used to study direct and indirect effects.
Path analysis allows the exploration of multiple dependent and independent variables simultaneously.
A prospective study design was used to assess temporal relationships between variables.
This observational study does not permit any claims with regard to causal inference.
Introduction
Fear of movement (kinesiophobia) is present in 45% of patients with cardiovascular disease (CVD) at the start of cardiac rehabilitation (CR) and remains present in 20% of patients after 3–10 months after hospital discharge. Kinesiophobia is associated with decreased quality of life and low levels of physical activity (PA).1–3 Moreover, kinesiophobia negatively impacts the uptake of CR, despite CR’s proven benefits such as reduced morbidity and mortality, and better psychological well-being.4–6
The effect of kinesiophobia at hospital discharge on the uptake of CR has not been prospectively investigated. Previous qualitative research has shown that patients attribute high levels of kinesiophobia to a lack of support and information at hospital discharge from a healthcare provider.3 Insight in factors associated with kinesiophobia at hospital discharge, and how kinesiophobia impacts CR initiation, could help to identify potential determinants of kinesiophobia, which in turn could potentially impact CR initiation, and help to adequately support and refer those with kinesiophobia.
Therefore, the aims of this study were to explore (1) factors associated with kinesiophobia at hospital discharge and (2) the impact of kinesiophobia on initiation of CR.
Methods
Study design
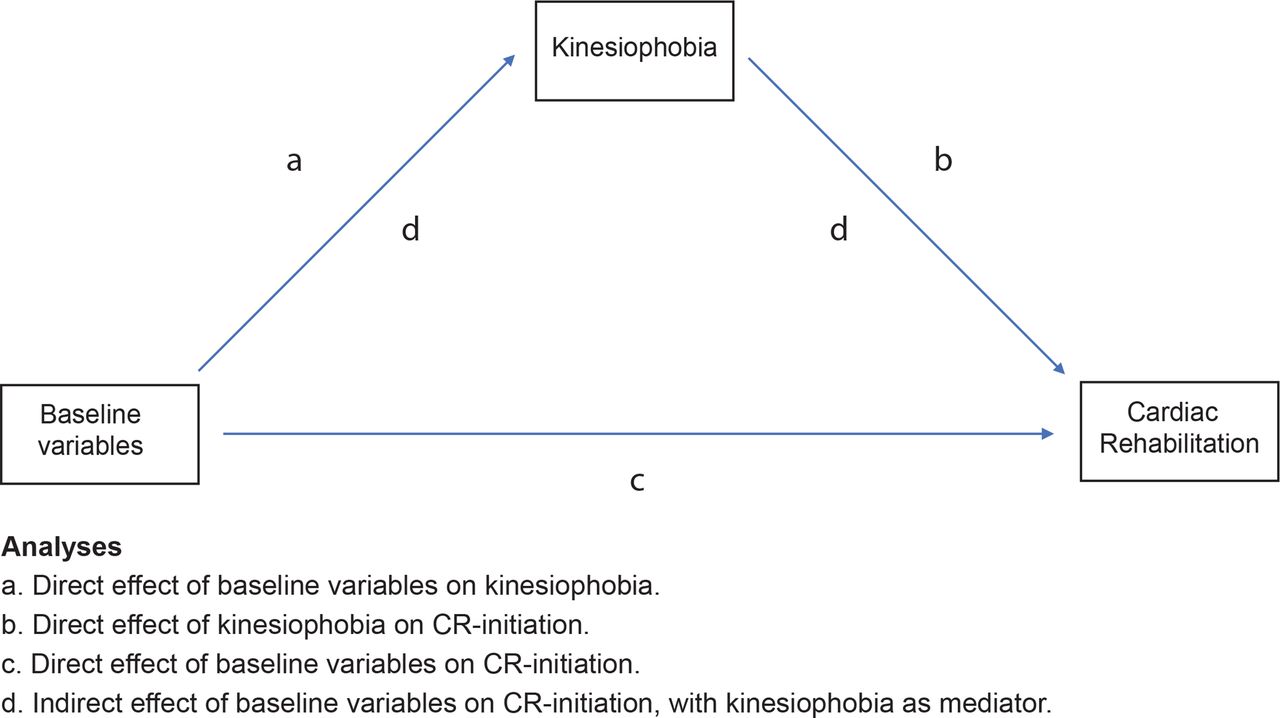
We conducted a prospective cohort study of patients hospitalised with a diagnosis of CVD, during the 3-month follow-up period after discharge. To explore factors associated with kinesiophobia and the effect of kinesiophobia on CR initiation, a hypothetical path model was developed (explained in detail below) (figure 1). Patients were included at hospital discharge (or shortly after) from the Amsterdam University Medical Centre at the Department of Cardiology.

Hypothetical path model. CR, cardiac rehabilitation.
Patient population
Eligible patients had been hospitalised for acute coronary syndrome (ACS), stable angina pectoris, acute heart failure (AHF) or atrial fibrillation (AF). Exclusion criteria were: referral to a nursing home; inability to complete questionnaires, for example, due to language problems.
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination plans of our research.
Sample size considerations
Based on previous research, we expected to include 10 variables in our final path model.2 We therefore aimed to include 15 times the number of parameters in our study, resulting in a final sample size of 150 patients.7
Data collection and measurements
Patients were identified between August 2019 and May 2021 through the electronic health records system of the Amsterdam University Medical Centre. During hospitalisation, eligible patients were interviewed by study staff of the Amsterdam University of Applied Sciences and enrolled in this study if they consented. The following data were collected from the electronic health record: age, sex, educational level, marital status, cardiac diagnosis and disease history. Patients were asked by email to complete questionnaires about their biopsychosocial complexity, the level of self-efficacy, anxiety and depression at discharge.
Outcomes
The primary outcomes were kinesiophobia at hospital discharge and CR initiation (yes/no) 3 months after discharge. At hospital discharge, patients completed the Tampa Scale for Kinesiophobia (TSK-NL Heart). The TSK-NL Heart consists of 13 questions with a 4-point scale ranging from 1 to 4, with a minimum score of 13 and maximum score of 52 points. Scores on the TSK-NL Heart are categorised as follows: subclinical: 13–22; mild: 23–32; moderate: 33–42 and severe: 43–52.1 After 3 months, patients were asked, by telephone, if they (1) were referred for CR, (2) initiated CR, (3) were readmitted to the hospital for an unplanned procedure.
Self-reported measurements
All self-reported measurements were completed during, or shortly after, hospital discharge (maximum 2 days).
Biopsychosocial complexity
Patients’ biopsychosocial complexity was assessed with the InterMed Self-Assessment (IMSA). The IMSA has three domains: biological complexity (chronicity and severity of symptoms, complications and life threat), psychological complexity (restrictions in coping, resistance to treatment, mental health threat, psychiatric dysfunction) and social complexity (social dysfunction, residential instability). Scores >19 indicate high complexity.8 In this study, the biological, psychological and social domains were analysed separately.
Generic anxiety and depression
Anxiety and depression were assessed with the Hospital Anxiety and Depression Scale (HADS). A sum score of 8–10 is defined as ‘possible anxiety/depressive disorder’, while a sum score of 11–21 is defined as ‘likely anxiety/depression disorder’.9
Cardiac anxiety
The Cardiac Anxiety Questionnaire (CAQ) is an 18-item, self-report questionnaire, designed to measure cardiac anxiety (fear, attention, avoidance of physical exercise and safety-seeking behaviour), rated on a 5-point Likert scale ranging from 0 (never) to 4 (always).10
Self-efficacy
Self-efficacy was assessed with the General Self-Efficacy Scale (GSES). The GSES is a 10-item questionnaire with a 4-point Likert scale ranging from 0 (completely disagree) to 4 (completely agree). A higher sum score indicates better self-efficacy.11
Statistical analysis
Descriptive statistics
Patient characteristics are presented as median and IQR or numbers (%). We analysed baseline kinesiophobia and differences between patients based on CR referral and CR initiation. In addition, we assessed which patients were readmitted to the hospital for ACS, revascularisation or electrocardioversion within the period of this study (3 months).
Path analysis
We explored direct effects (relations between independent and dependent variables) and indirect effects (the effect of an independent variable on a dependent variable through one or more intervening or mediating variables)12 (figure 1). Since little is known about kinesiophobia in patients with CVD, a comprehensive approach was used to explore the association between baseline variables, kinesiophobia and the initation of CR. We studied the association between demographic variables (age, sex, educational level), medical variables (diagnosis, cardiac disease history, risk factors), psychological variables (biopsychosocial complexity, generic anxiety, cardiac anxiety, self-efficacy) and kinesiophobia. Categorical variables were recoded into dummy variables (educational level, diagnosis, cardiac disease history, risk factors). All other variables (age, body mass index, kinesiophobia, psychological variables) were analysed as continuous. In addition, we studied the longitudinal association between kinesiophobia, the above-mentioned demographic, medical, psychological variables and CR initiation. An overview of all analyses is found in online supplemental table 1.
Supplemental material
First, univariable linear regression was used to select variables associated with kinesiophobia (TSK-NL Heart total score). Univariable logistic regression was used to select variables associated with CR initiation in a subsample that was referred for CR (cut-off for variable retainment in both analyses: p<0.10).13 Second, a path analysis was conducted. Backward elimination was used to select significant (p<0.05) variables associated with kinesiophobia. The initiation of CR (yes/no) was regressed on kinesiophobia to study the direct effect of kinesiophobia on CR initiation and possible indirect effects of baseline variables on CR initiation, with kinesiophobia as mediator. Path analyses were conducted for the total sample and in a subsample that was referred for CR.
All effects on kinesiophobia (continuous TSK-NL Heart score) are presented as standardised beta estimates (β). Effect size of (β) was interpreted as small (<0.29), moderate (0.30–0.49) or large (>0.50).14 Effects on the uptake of CR are presented as ORs. In the final model, the effect of kinesiophobia on CR initiation was corrected for age and gender. The Satorra-Bentler scaled X2 test was used to assess model fit. Patterns of missing data were analysed with Little’s test to assess the pattern of missing data. A full conditional specification multiple imputation (FCS-MI) was used to impute data.15 Data imputation was conducted in SPSS V.28. An overview of all missing data is found in online supplemental table 1. All descriptive and univariable analyses were performed in SPSS V.28. The path models were analysed using Mplus V.8.0.
Results
Demographic and clinical characteristics
In total, 188 patients were assessed for eligibility. After inclusion, 39 patients (20.7%) did not complete any questionnaires, and 2 died. At hospital discharge, 82 (55%) patients were referred for CR, of which 61 (40.9%) initiated CR in 3-month follow up (figure 2).

Flow chart of the study. CR, cardiac rehabilitation.
Finally, 149 patients were included in the analyses with a median age of 65 years (range 32–86). The majority of patients were male (78.5%) and lived with a partner (77.9%). Most patients had been admitted for an elective intervention (55.7%), of which 78.5% underwent a percutaneous coronary intervention (PCI). A history of hypertension was present in 40.9%, dyslipidaemia in 26.2% and diabetes mellitus in 17.4. Prior myocardial infarction was present in 23.4% and prior PCI (acute or elective) in 37.6% (table 1). The distribution of kinesiophobia levels were: subclinical (24.2%), mild (53.0%), moderate (22.1%) and severe (0.7%) (figure 3).

Kinesiophobia scores at hospital discharge. TSK-NL Heart, Tampa Scale for Kinesiophobia.
Baseline characteristics
Baseline TSK scores were, on average, 3 points higher in patients who were referred but did not initiate CR, than in those who did initiate CR (30.39±6.76 vs 27.37±5.98). Within 3 months of follow-up, 15 patients (10%) were readmitted to the hospital: 6 patients for electrocardioversion (ECV), 6 patients for PCI, 2 patients for ACS and 1 patient for AHF.
Univariable analyses
An overview of all our univariable linear regression analyses is presented in table 2. We found small associations between kinesiophobia and female sex (β=0.19, 95% CI: 0.03 to 0.35), age ≤50 years (β=0.22, 95% CI: 0.38 to 2.49) and HADS anxiety (β=0.27, 95% CI: 0.11 to 0.42). Higher education (β=−0.24, 95% CI: −0.40 to −0.08) and GSES self-efficacy (β=−0.18, 95% CI: −0.34 to −0.02) were negatively associated with kinesiophobia. Moderate associations were found between kinesiophobia and HADS depression (β=0.32, 95% CI:0.16 to 0.47), IMSA psychological complexity (β=0.32, 95% CI: 0.17 to 0.48), IMSA social complexity (β=0.33, 95% CI: 0.17 to 0.48) and CAQ cardiac anxiety (β=0.42, 95% CI: 0.27 to 0.57).
Univariable linear regression with TSK-NL Heart as dependent variable (N=149)
In patients referred for CR (N=82), nine candidate predictors of CR initiation were found. TSK kinesiophobia (OR: 0.92, 95% CI: 0.85 to 1.00), treatment with ECV (OR:0.21, 95% CI: 0.07 to 0.69), AF (OR: 0.21, 95% CI: 0.07 to 0.69), HADS anxiety (OR: 0.89, 95% CI: 0.79 to 1.00), HADS depression (OR: 0.93, 95% CI: 0.81 to 1.06) and IMSA psychological complexity (OR: 0.82, 95% CI: 0.66 to 1.00) decreased the odds of CR initiation. Treatment with PCI (OR: 3.56, 95% CI: 1.15 to 11:00), acute admission (OR: 2.58, 95% CI: 0.89 to 7.54) and GSES self-efficacy (OR: 1.18, 95% CI: 1.03 to 1.36) increased the odds of CR initiation (table 3). In those referred for CR, seven patients were readmitted to the hospital for an unplanned procedure, of which six initiated CR (OR: 2.18, 95% CI: 0.32 to 2.85). An overview of all candidate predictors of CR in the total sample (N=149) is found in online supplemental table 2.
Supplemental material
Univariable logistic regression with CR initiation as dependent variable in a subsample referred for CR (N=82)
Path analysis
Analysis 1: total sample
In the total sample, we identified three variables that were associated with kinesiophobia (table 4). CAQ cardiac anxiety (β=0.33, 95% CI: 0.19 to 0.48) was moderately associated with kinesiophobia. A small association was found between kinesiophobia and IMSA social complexity (β=0.23, 95% CI: 0.06 to 0.39) and higher education (β=−0.18, 95% CI: −0.34 to −0.02). We identified two predictors of CR initiation: age (years) (OR: 0.96, 95% CI: 0.93 to 0.99) decreased, while higher levels of GSES self-efficacy (OR: 1.10, 95% CI: 1.01 to 1.20) increased the odds of CR initiation. An overview of all variables associated with kinesiophobia and CR initiation is presented in a path analysis diagram (figure 4). Model fit (X2=−2.254124, df: 5, p>0.9).

Path analysis in total sample (N=149). CR, cardiac rehabilitation.
Path analysis with TSK and CR as dependent variables (N=149)
Analysis 2: subsample referred for CR
In the subsample that was referred for CR, we identified two variables that were associated with kinesiophobia (table 5). A moderate positive association was found between CAQ cardiac anxiety (β=0.43, 95% CI: 0.24 to 0.62) and kinesiophobia, while GSES self-efficacy (β=−0.29, 95% CI: −0.47 to −0.12) was negatively associated with kinesiophobia. Age (OR=0.98, 95% CI: 0.94 to 1.02) was kept in the model since model fit decreased after omission of this variable and age <50 years was significantly associated with kinesiophobia and initiation of CR (table 2 and online supplemental table 2). Corrected for age, kinesiophobia (OR=0.92, 95% CI: 0.84 to 0.99) significantly decreased the odds of CR initiation. A moderate indirect effect of CAQ cardiac anxiety (OR=0.98, 95% CI: 0.95 to 1.00) on CR initiation was found with kinesiophobia as a mediator. The subsample analysis is presented in a path analysis diagram (figure 5). Model fit (X2=−0.0062, df: 4, p>0.99).
Path analysis with TSK and CR initiation as dependent variables, restricted to patients who had been referred for CR (N=82)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Path analysis in subsample referred for CR. CR, cardiac rehabilitation.
Discussion
We found that mild and moderate levels of kinesiophobia were present at hospital discharge in a substantial group of patients with CVD (53% and 22.1%, respectively). Cardiac anxiety, social complexity and educational level were associated with kinesiophobia at hospital discharge. In patients who were referred for CR, self-efficacy was negatively associated with kinesiophobia. In patients referred for CR, the presence of kinesiophobia was associated with a lower rate of CR initiation. An indirect effect of cardiac anxiety on CR initiation was found.
Our study shows that kinesiophobia decreases the likelihood of CR initiation. Theoretically, this makes sense since the construct kinesiophobia comprises ‘fear of injury’, ‘perception of risk’ and ‘avoidance of physical activity’. Patients with higher levels of kinesiophobia might associate participation in CR as threatening since exercise and PA are the cornerstones of CR.
We identified a moderate association between cardiac anxiety and kinesiophobia. In a previous study, a similar result was found.1 Moreover, we found that kinesiophobia mediated the relationship between cardiac anxiety and CR initiation. This finding is in line with previous research which reports that kinesiophobia mediates the relationship between self-rated anxiety and CR attendance.4 The CAQ measures behaviour and anxiety-related symptoms (eg, ‘I avoid activities that make my heart beat faster’), whereas the TSK-NL Heart measures patients’ beliefs about their physical state (eg, ‘If I tried to be physically active, my heart problem would increase’). More research is needed to investigate the impact of specific kinesiophobic beliefs on behaviour and anxiety-related symptoms and vice versa.
In line with our findings, Brunetti et al showed that educational level was negatively associated with kinesiophobia.16 In a previous study, we found that patients with high levels of kinesiophobia often do not understand medical information and misinterpret body signals, which in turn is associated with poor health literacy and low educational level.3 17 This finding fits well with the call for more tailored and understandable information at hospital discharge, provided by a trained healthcare provider.3
Patients scoring high on social complexity suffered from higher levels of kinesiophobia. This is in line with our previous study where we found that patients with lower levels of kinesiophobia often experienced greater social support than those with higher levels of kinesiophobia.3 The presence of a partner has been shown to improve lifestyle modification in cardiac patients and increase adherence to CR.18 Moreover, participation of partners in CR programmes improves PA levels in patients.19 20 Future studies should evaluate the role of social support on levels of kinesiophobia after cardiac hospitalisation.
Self-efficacy was negatively associated with kinesiophobia, in those referred for CR, and predicted CR initiation in the total sample. Self-efficacy refers to ‘one’s belief in their capacity to execute behaviours necessary to produce specific performance attainments’.21 The association between self-efficacy and kinesiophobia has been shown in patients with musculoskeletal disorders, but not in patients with CVD.22 23 Zelle et al reported that the impact of kinesiophobia on PA is largely mediated by self-efficacy, and should therefore be evaluated when targeting kinesiophobia.24 Our study showed that self-efficacy increased the likelihood of CR initiation by 10%. Self-efficacy is linked to CR initiation, but is often lacking in patients with psychological distress.25 Therefore, self-efficacy-building activities should be considered before CR initiation.26 Currently, behaviour change strategies are offered in CR programmes to improve PA levels, and promote smoking cessation and a healthy diet.27 However, these interventions are currently limited to those who initiate CR. An early behavioural intervention, aimed at reducing kinesiophobia and stimulating self-efficacy shorty after hospital discharge, might improve CR initiation.
Strengths and limitations
Our study has several strengths. First, we studied kinesiophobia and CR initiation using a prospective design. We were therefore able to study the temporal sequence of kinesiophobia and CR initiation, and multiple factors that impacted our outcomes. Second, using a path model allows for the specification of multiple, dependent and independent variables simultaneously and thereby gives insight into complex relationships between variables.12 Our comprehensive path analysis gives insight in the factors that are associated with kinesiophobia and predict CR initiation. These findings aid the development of tailored interventions to target kinesiophobia and improve CR initiation.
Our study has some limitations. First, a substantial number of patients were included after the start of the COVID-19 pandemic. Although CR was offered remotely, this might have impacted kinesiophobia levels and CR initiation. Second, by using path analysis, we were able to explore a network of sequential relations with contributions from all paths (direct and indirect). Conceptually, a mediation model (in contrast to a confounding model) assumes that a series of variables relate via a causal chain of effect and each variable in the model affects variables occurring later in the chain.28 In our model, an indirect effect of cardiac anxiety, through kinesiophobia, was found on CR initiation. Theoretically, our finding makes sense, since somatic symptoms, such as chest pain or palpitations (cardiac anxiety), can lead to negative beliefs about one’s physical state (kinesiophobia), which in turn might lead to not initiating CR. Future studies should evaluate the potential mediating role of kinesiophobia in the uptake of CR. Third, although our interest is in causes of kinesiophobia and kinesiophobia as a cause of not initiating CR, our observational study does not permit any claims with regard to causal inference since necessary conditions for causal inference (exchangeability, positivity and consistency) have most likely not been met.29 Nevertheless, this study reports important associations between baseline variables and kinesiophobia. In addition, we showed that kinesiophobia decreased the likelihood of CR initiation. Future studies, using a causal design, can use these results to investigate determinants of kinesiophobia and the effect of kinesiophobia on CR initiation.
Conclusion
Kinesiophobia is prevalent at hospital discharge. Path analysis revealed that cardiac anxiety and social complexity were positively associated, whereas educational level and self-efficacy were negatively associated with kinesiophobia at hospital discharge. In addition, patients with (high levels of) kinesiophobia were less likely to initiate CR.
Data availability statement
Data are available upon reasonable request. Data are available on reasonable request. Requests for analyses of data from this study should be directed to PK (p.keessen@hva.nl).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and the Medical Ethics Committee of the Amsterdam University Medical Centre approved the study (protocol number: NL65218.018.18). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors are grateful to the Department of Cardiology of the Amsterdam University Medical Centre, all research nurses involved in the data collection and patients who participated in this study: Hiltje van der Werf, Manon Ootes, Marjon van Maarl and Willeke Veenhuizen.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GTR, BV, HJ, CL and WSoR participated in the design of the study. PK and IvD were responsible for coordination and acquisition of the data. PK, K-JK and GTR performed the statistical analysis. All authors contributed to the preparation and critical review, and approved the final manuscript. WSoR is responsible for the overall content as guarantor.
Funding Financial support was received from the Dutch Research Council (NWO) as a personal grant (PK; nr: 023.010.064) and a RAAK-PRO grant (RAAK.PRO02.083).
Disclaimer The funding bodies had no role in the design of the study and collection, analysis and interpretation of data and in writing the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.