Article Text

Abstract
Objectives Elevated baseline serum alkaline phosphatase (ALP) may correlate with higher medium-term to long-term mortality in the general population and in patients with chronic kidney disease. However, few data are available on the association between serum ALP and the short-term prognosis of patients on haemodialysis (HD). We verified the association of ALP levels and bacteraemia or death in maintenance HD patients suspected of bacteraemia in an outpatient setting.
Design We analysed 315 consecutive HD patients suspected of having bacteraemia with two sets of blood culture drawn on admission.
Setting Admission to two tertiary-care university medical centres from January 2013 to December 2015.
Participants Consecutive cases on maintenance HD aged≥18 years. Cases of hospitalised patients who had been transferred from another hospital, had a dialysis vintage<2 months, were also undergoing peritoneal dialysis, and/or were receiving HD less than once a week were excluded.
Primary and secondary outcome measures Primary outcome measure was bacteraemia and secondary outcome was in-hospital death.
Results Among 315 cases included in the study, 187 had baseline-measured ALP levels, with a cut-off value on ROC analysis of 360 U/L (Area Under the Curve (AUC) 0.60, sensitivity 0.49, specificity 0.76). In multivariate analysis, there was a statistically significant association between a higher ALP in hospital visit and bacteraemia (OR: 2.37, 95% CI: 1.17 to 4.83). However, there were no statistically significant associations between higher ALP and in-hospital death (OR: 1.20, 95% CI: 0.57 to 2.54). A sensitivity analysis of 187 patients with no missing ALP values also demonstrated a significant association between elevated ALP and bacteraemia, but no significant association between ALP and in-hospital death.
Conclusions Elevated ALP is a predictor of bacteraemia. In HD patients suspected of bacteraemia in outpatient settings, increased ALP levels were associated with increased likelihood of confirmed disease.
- infectious diseases
- dialysis
- nephrology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first multicentre investigation of the association between alkaline phosphatase (ALP) levels and bacteraemia or death in patients on maintenance haemodialysis (HD).
Elevated serum ALP levels in HD patients suspected of bacteraemia could lead to earlier diagnosis and may potentially allow for earlier medical intervention.
Our findings should facilitate further research to investigate any causal association of ALP elevation with bacteraemia in complex biological systems.
Although the study sample consisted of patients on maintenance HD from two geographically diverse hospitals in Japan, our inferences may not be generalisable to patients on maintenance HD in other clinical settings.
Introduction
In patients on haemodialysis (HD), it is well known that the second most common cause of death after cardiovascular events is infection, especially sepsis or bacteraemia.1 2 The prevalence of bacteraemia in patients with HD is 10–40 times that in the general population3 4 with a 50-fold increase in mortality.5–7
Multiple studies have shown a positive relationship between serum alkaline phosphatase (ALP) and medium-term to long-term mortality in the general population and in patients with chronic kidney disease (CKD), including those on HD and peritoneal dialysis (PD).8–15 The explanation is that elevated levels of serum ALP may reflect abnormalities such as arterial stiffness, renal osteodystrophy and inflammation.11 12 16–18
In addition to the relationship between serum ALP and mid-term to long-term prognosis, observational studies have identified other risk factors for bacteraemia in dialysis patients, including leucocyte dysfunction, malnutrition, parathyroid hormone derangements and vitamin D deficiency.8 19–21
We focused on ALP, an enzyme that hydrolyses phosphate monoester. It is a dimer consisting of two identical molecules, and is expressed as four isoenzymes (placental, germ cell, intestinal and tissue-non-specific (liver/bone/kidney)).22 ALP is known as an indicator of renal osteodystrophy, associated with its close relationship with bone, parathyroid gland function, the GI tract and overall mineral balance.23 Historically, high ALP levels have been considered related to renal osteodystrophy.
Damera et al reported that ALP is one of the inflammatory markers that are independent of 25-OH vitamin D levels in CKD.24 In addition, the ‘BAC-HD score’ (Body temperature ≥ 38.3°C, ALP > 360 U/L, C-reactive protein [CRP] ≥ CRP 10 mg/dL, Heart rate ≥ 125 bpm, Drugs: no prior antibiotic use for 1 week),25 which we previously developed, is a clinical prediction algorithm for bacteraemia among patients with HD.
Tung et al showed that extremely high ALP levels (ALP>1000 U/L) were associated with bacteraemia.26 However, that study had a very small sample size of 16. In other words, there are few studies showing an association between serum ALP and short-term prognosis of bacteraemia and in-hospital mortality.
ALP levels can be measured easily and are a less burdensome test for the patient. In addition, bacteraemia is an important outcome for HD patients because of its high morbidity and mortality. Therefore, it is important to investigate serum ALP levels as predictive markers of bacteraemia. Our aim was to verify the association of ALP levels and bacteraemia or death in maintenance HD patients suspected of bacteraemia in an outpatient setting.
Methods
In the present study, the department of nephrology of Aso Iizuka Hospital had collected anonymous data from the participating facilities. Since this study was retrospective, the consent of participants was not obtained. The study results are reported according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cross-sectional studies.27
Study design and participants
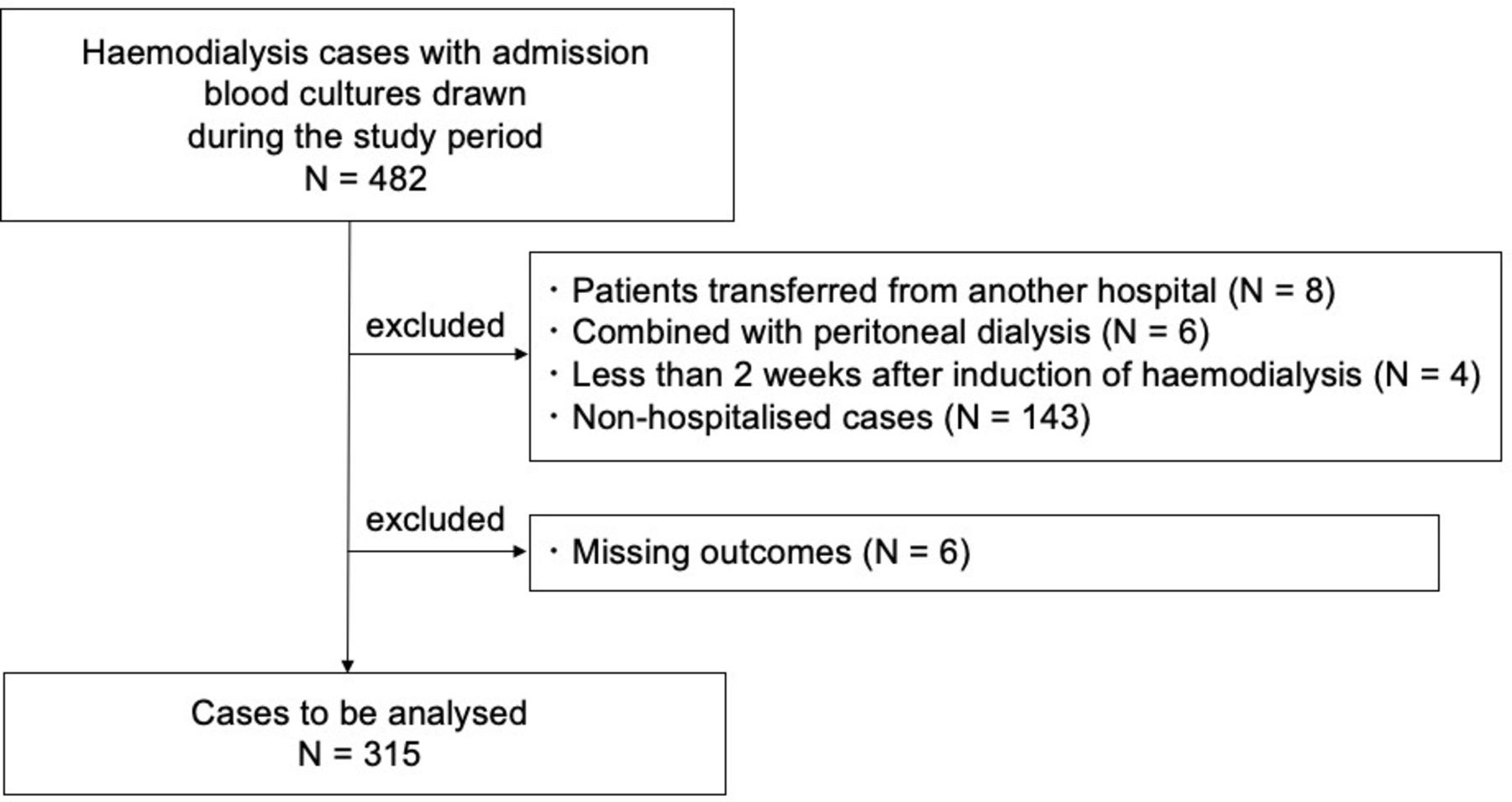
We performed a cross-sectional study at the three academic medical institutions mentioned above. Data were collected from medical records from January 2013 to December 2015 in each facility. We enrolled consecutive cases of patients on maintenance HD who were aged≥18 years and had two sets of blood cultures drawn at admission to assess for the presence of bacteraemia. Cases of hospitalised patients who had been transferred from another hospital, had a vintage of dialysis<2 months, were also undergoing PD, or were receiving HD less than once a week were excluded (figure 1).

Study flow. After the sampling, 315 cases that met the eligibility criteria were included.
ALP levels
Logistic regression analysis was performed with bacteraemia as the dependent variable and ALP as the explanatory variable. Based on the Receiver Operatorating Characteristic curve (ROC) analysis, the value with the highest discriminatory power was used as the cut-off point.
Outcomes
The primary outcome was bacteraemia, which was diagnosed based on the results of admission blood cultures. To avoid misclassification of the primary outcome, an external consensus panel of infectious disease physicians with more than 10 years’ clinical experience and Japanese board certification in infectious disease determined whether a culture was contaminated or not based on the conventional definition of contamination and their clinical expertise. Contamination was defined as: only one of the two sets of culture bottles was positive; or the presence of certain species of bacteria, such as diphtheroids, Bacillus spp, Propionibacterium spp, Micrococci spp, Corynebacterium spp and coagulase-negative staphylococci. The secondary outcome was in-hospital death.
Other covariates
Clinical information collected on hospital admission included age, sex, body temperature, systolic and diastolic blood pressure, pulse rate, respiratory rate, HD vintage, presence or absence of diabetes mellitus, and use of vitamin D analogues. In addition, white blood cell counts, aspartate aminotransferase (AST), total bilirubin (T-BIL), corrected calcium (cCa), phosphate and CRP were obtained from medical records.
Statistical analysis
The serum ALP levels at diagnosis were stratified by the cut-off value based on ROC analysis, and patients’ baseline characteristics were expressed as medians (quartile) or numbers (%). Multivariate analysis was performed for the primary outcome of bacteraemia in four models adjusted for age, sex, AST, vitamin D analogue use and HD vintage(Model 1, adjusted for age, sex; Model 2, adjusted for Model 1 + aspartate aminotransferase; Model 3, adjusted for Model 2 + vitamin D analogue use; Model 4, adjusted for Model 3 + haemodialysis vintage). Five models were used for the secondary outcome: in-hospital death, adjusted for age, sex, AST, T-BIL, vitamin D analogue use, cCa, P, HD vintage and presence of bacteraemia using a logistic regression model (Model 1, adjusted for age, sex; Model 2, adjusted for Model 1 + aspartate aminotransferase; Model 3, adjusted for Model 2 + vitamin D analogue use; Model 4, adjusted for Model 3 + haemodialysis vintage; Model 5, adjusted for Model 4 + presence of bacteraemia, figure 2). We selected variables for multivariate analysis through a literature review and based on clinical experience. To minimise the bias from missing data, all missing values were imputed using multiple imputation by chained equation treated as missing at random including ALP; 10 imputed datasets were created.28 On multivariate analysis, these 10 datasets were combined with Rubin’s rules and analysed. Analyses were assessed at a two-tailed alpha=0.05. We used commercial software (STATA V.15.0, StataCorp LP, College Station, Texas, USA) for statistical analysis.

{kind=link}
{kind=link}
Association between alkaline phosphatase (ALP) and bacteraemia or In-hospital death: logistic regression model. Multivariate analysis shown in this figure. There was no relationship between higher ALP and in-hospital death; however there was a statistically significant association between higher ALP and bacteraemia. Bacteraemia outcome: Model 1, adjusted for age, sex; Model 2, adjusted for Model 1 + aspartate aminotransferase, Model 3, adjusted for Model 2 + vitamin D analogue use; Model 4, adjusted for Model 3 + haemodialysis vintage In-hospital death outcome: Model 1, adjusted for age, sex; Model 2, adjusted for Model 1 + aspartate aminotransferase; Model 3, adjusted for Model 2 + vitamin D analogue use; Model 4, adjusted for Model 3 + haemodialysis vintage; Model 5, adjusted for Model 4 + presence of bacteraemia.
Sample size
We estimated the prevalence of bacteraemia in maintenance HD patients suspected to have bacteraemia to be 16% based on a previous report.25 Since we planned a logistic regression analysis with five explanatory variables, we estimated that the number of bacteraemia cases was required to be 50, following the rule of requiring 10 outcomes per explanatory variable.29 From these, it was estimated that a total of 312 subjects was needed.
Sensitivity analysis
To demonstrate the robustness of our inferences, we conducted a complete case analysis for ALP as a sensitivity analysis, which meant excluding participants missing admission ALP. In addition, we added CRP, which is not a confounding factor but is a strong prognostic factor, and performed a sensitivity analysis.
Patient and public involvement
No current patients or members of the public were directly involved in this study.
Results
The cut-off value for ALP was 360 U/L based on ROC analysis (AUC 0.60, sensitivity 0.49, specificity 0.76) in complete cases of ALP. Among the 315 cases included in the study (figure 1), 187 had baseline measured ALP levels (133 with normal levels≤360 U/L and 54 with ALP levels>360 U/L). Table 1 shows the baseline characteristics of the cohort.
Baseline characteristics
Occurrence of outcomes
Table 2 shows the incidence of bacteraemia and in-hospital deaths in the total and groups stratified by ALP. The high-ALP group had a higher incidence of bacteraemia.
Incidence of bacteraemia and in-hospital death in the total and groups stratified by ALP
Association of ALP in hospital visit and bacteraemia
In the multivariate analysis shown in figure 2, there was a statistically significant association between higher ALP in hospital visit and bacteraemia in all four models.
Association of ALP in hospital visit and in-hospital death
As shown in figure 2, there were no statistically significant associations between higher ALP and in-hospital death in all five models.
Sensitivity analysis
To examine the robustness of the findings, we conducted a complete case analysis for ALP excluding participants who were missing ALP values. A sensitivity analysis of the 187 patients with no missing ALP values also demonstrated a significant association between ALP and bacteraemia, but no significant association between ALP and in-hospital death (figure 2). In a sensitivity analysis with the addition of CRP, results showed no significant association between bacteraemia and ALP levels in analysis adjusted for age, sex, AST, CRP, vitamin D analogue use or HD vintage (OR: 1.97, 95% CI: 0.97 to 4.01) as shown in the online supplemental figure.
Supplemental material
Discussion
This study showed a statistically significant positive correlation between ALP levels and bacteraemia in HD patients suspected of having bacteraemia in the outpatient setting. Few studies examining the association between serum ALP and short-term prognosis have been reported. This is the first multicentre investigation of the association between ALP levels and bacteraemia or death in patients on maintenance HD.
Based on the results of this study, elevated serum ALP levels in HD patients with suspected bacteraemia could allow for early recognition and may potentially allow for earlier medical intervention.
Association between ALP and bacteraemia
We considered two reasons why elevated ALP levels were associated with bacteraemia. First is the involvement of hepatobiliary infections such as cholangitis. We hypothesise that it may cause bacteraemia or sepsis, leading to elevated ALP levels.30 31 However, since the main cause of bacteraemia in HD patients is bloodstream infection with staphylococci, it is considered that bacteraemia due to biliary tract infection does not significantly affect ALP levels in this population. In addition, we adjusted for the liver enzyme AST in multivariate analysis, but the changes in the OR of bacteraemia were small. These findings suggest that the increase in ALP levels in HD patients was due to factors other than hepatobiliary infection.
Second, we considered a biological response to bacteraemia. Previous studies have shown that ALP acts on inflammatory mediators, such as bacterial endotoxin and extracellular ATP, and may detoxify them via dephosphorylation.10 12 32–34 In animal models of sepsis (mice, rats, sheep, piglets), it has been reported that treatment with ALP reduced systemic inflammation and organ dysfunction, and improved survival.32 35–39 There are also reports suggesting that ALP is effective in the treatment of sepsis in HD patients.40 Sepsis-related AKI is thought to be the result of a combination of inflammatory, nephrotoxic and ischaemic injury with rapid progression of renal damage. Pickkers et al showed that treatment with ALP improved creatinine clearance, as well as the need for and duration of dialysis in patients with sepsis-related AKI.41
The above two points suggest that the increase in ALP may be a response to inflammation or bacteraemia.
In maintenance HD patients with a high risk of infection, the therapeutic strategy, including antimicrobials, is often distressing until the results of blood culture are available. Unnecessary administration of antimicrobials can be harmful to the patient, because antimicrobial resistance is a serious problem for them. However, it has also known that delayed administration of empiric antimicrobial therapy leads to increased mortality.42 We need to decide the timing of administration of therapy and choice of antimicrobial agents appropriately. Serum ALP levels have been reported as one example of a simple clinical prediction rule in the bacteraemia ‘BAC-HD score’.43 In maintenance HD outpatients suspected of sepsis, elevated serum ALP levels may indicate the presence of bacteraemia and may aid in the decision to begin early antimicrobial therapy and in the choice of the antimicrobial agent.
ALP isozymes
Intestinal isozyme may be of possible relevance to sepsis-related treatment.33 40 However, no association has been found between specific isozymes and bacteraemia or sepsis, and we do not recommend the measurement of isozymes at this time in clinical practice. If the above two points are resolved, it may be useful to measure ALP isozymes in the future.
The species associated with bacteraemia
It is known that percutaneous bloodstream infections caused primarily by gram-positive cocci (GPC) are common in HD patients.44 However, a previous meta-analysis reported that about 20% of HD catheter-related bacteraemias were caused by gram-negative rods (GNR) as well as coagulase-negative staphylococci and Staphylococcus aureus.45
In our study, GNR-induced sepsis accounted for 34% of cases, which may have been associated with ALP levels. However, the median quartile values of ALP in bacteraemia due to GPC and GNR were 302 (range, 217–455) U/L and 388 (range, 225–530) U/L, respectively, and there may be reasons other than this hypothesis. Second, given the mechanism by which GPC inactivates inflammatory mediators, ALP can be elevated not only by GNR but also by GPC-induced sepsis.46 From the above, it is considered that ALP is associated with bacteraemia in HD patients regardless of the category of the offending bacterium.
Association between ALP and mortality
We found no significant association of ALP with mortality in the analysis for secondary outcome, in contrast to previous studies.10 14 47 In one study, HD patients with elevated ALP levels had an approximately 50% higher risk of infection-related mortality compared with those with normal ALP levels.14 One reason for the significant difference in bacteraemia but not in mortality may be that the overall prognosis for maintenance HD patients in Japan is good.
Limitations
Our study has several limitations. First, there may be unmeasured confounding factors, a limit of observational studies. However, the study was designed to optimise the selection of adjusted confounding factors and to minimise their effect as compared with previous studies. It is possible that intact PTH was a residual confounding factor. However, we could not test this possibility because we did not measure intact PTH in this study, for two reasons: first, because intact PTH may not contribute significantly to outcomes for bacteremia or mortality48; and second, since ALP reflects factors of origin other than bone, we considered that the association between PTH and ALP in the acute phase, such as the subject of this study, might be still unclear. Nevertheless, there are reports of increased mortality in patients with PTH outside the normal range in the non-acute phase,49 and further validation is needed. Second, since it is a cross-sectional study, the possibility of reverse causation cannot be denied. However, high ALP levels were shown to be a predictor of bacteraemia. Third, this was a retrospective study, and the uncertainty of the data extracted from medical records cannot be ruled out. Fourth, while we conducted a multicentre study, the sample size was relatively small and there were substantial missing data. In patients with ALP data, there was a statistically significant association between ALP and bacteraemia, but no association between ALP and in-hospital mortality. We consider the small sample size as a reason why we could not show an association with mortality, unlike previous reports. This is the first study suggesting that serum ALP is one of several independent predictors of bacteraemia in HD patients. Our study should facilitate further validation studies to confirm the association of ALP elevation and bacteraemia in maintenance HD patients. Fifth, it cannot be determined in this study whether serum ALP levels were elevated before illness or due to bacteraemia. However, baseline serum ALP levels are often unknown in clinical practice. Therefore, we consider it may be clinically acceptable. Lastly, the study sample consisted of patients on maintenance HD from three geographically diverse hospitals in Japan, and our findings may not be generalisable to patients on maintenance HD in other clinical settings (eg, patients with hospitalisation at index dates). Nonetheless, our inferences should remain relevant for over 340 000 patients on maintenance HD in Japan, a vulnerable population with high mortality from bacteraemia, at about 14 times that of the general population.50
Conclusions
By conducting a multicentre retrospective observational study, we identified elevation of ALP levels as an independent predictor of bacteraemia among maintenance HD outpatients suspected of having sepsis. The association remained consistent after adjusting for other potential predictors for bacteraemia. For clinicians, our data may support the early identification of patients with bacteraemia and their resultant prompt hospitalisation. Our findings may facilitate further research to investigate any causal association of ALP elevation with bacteraemia in complex biological systems.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the ethics committees of Aso Iizuka Hospital (No. 17167), Okinawa Chubu Hospital (H28_No. 51), and Saku Central Hospital (201701-01), and was conducted in accordance with the ethical standards of the Declaration of Helsinki.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AK and SS contributed equally.
Contributors All authors have read and approved the submission of the manuscript; the manuscript has not been published and is not being considered for publication elsewhere, in whole or in part, in any language, except as an abstract. SS created the study design. SS, YR, SY, KT, MM and RN performed data collection. AK and SS analysed data and wrote the article. SS is responsible for the overall content as the guarantor. All authors reviewed the manuscript. KF approved the submission of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.