Article Text

Abstract
Introduction Chromosomal abnormalities and monogenic disorders account for ~15%–25% of recognisable birth defects. With limited treatment options, preconception and prenatal screening were developed to reduce the incidence of such disorders. Currently, non-invasive prenatal screening (NIPS) for common aneuploidies is implemented worldwide with superiority over conventional serum or sonographic screening approaches. However, the clinical validity for the screening of frequent chromosome segmental copy number variations and monogenic disorders still awaits to be proved.
Methods and analysis This study is a multicentre, prospective study. The participants were recruited from three tertiary hospitals in China starting from 10 April 2021. The study is expected to conclude before 10 October 2022. Pregnant women with abnormal prenatal screening results indicated for invasive prenatal diagnosis or those who decide to terminate their pregnancies due to abnormal ultrasound findings will be evaluated for enrolment. Cell-free DNA extracted from the maternal plasma will be used for an analytically validated comprehensive NIPS test developed by Beijing BioBiggen Technology Co. (Beijing, China). The diagnostic results from prenatal or postnatal specimens as well as the pregnancy outcome data will be collected to examine the clinical sensitivity, specificity, positive and negative predictive values of the test.
Ethics and dissemination This study was approved by the Obstetrics and Gynecology Hospital of Fudan University (2020-178). Results of this study will be disseminated to public through scientific conferences and a peer-reviewed journal. Written informed consents will be obtained from participants.
Trial registration number ChiCTR2100045739.
- antenatal
- reproductive medicine
- preventive medicine
- reproductive medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first prospective, multicentre clinical study for an integrated non-invasive prenatal screening test for both chromosomal abnormalities and monogenic diseases.
This study is focused on a panel of preselected diseases which have relatively high incidence.
The limitation for this study includes population stratification for high-risk pregnancies and potential loss of postnatal follow-up.
Introduction
Genetic aetiology of birth defects
Birth defects are congenital conditions causing structural or functional anomalies at birth, which greatly contribute to infant mortality and disability.1 Approximately 3%–5% of newborns are affected by a birth defect worldwide.2 Although the causes of most cases are unknown, about 15%–25% of birth defects are due to genetic diseases such as chromosomal abnormalities and monogenic disorders.3
The screening of severe genetic diseases
Great efforts have been made to prevent birth defects with an underlying genetic aetiology. Carrier screening for recessive disorders such as Tay-Sachs disease was proved to be highly effective for the reduction of its incidence.4 The first-trimester combined screening for fetal aneuploidies by prenatal ultrasound and maternal serum biochemical testing detects over 85% common trisomies at a false-positive rate of ~5% which can lead to parental anxiety and excessive invasive diagnostic procedures for otherwise normal pregnancies imposing a risk for pregnancy loss.5 6 Since the discovery of circulating fetal cfDNA in the maternal plasma during pregnancy, its biological characteristics and clinical implication have been extensively studied.7 8 Non-invasive evaluation for fetal gender and risks for monogenic disorders, aneuploidies, and chromosome segmental CNVs were developed using different molecular or genomic techniques.9–11 Importantly, the emergence of next-generation sequencing (NGS) technology enabled a practical population-based screening method for Down syndrome.12 13 In the past decade, NGS-based non-invasive prenatal screening (NIPS) for trisomy 21, 18 and 13 has become a new standard for prenatal care with proven clinical validity.14 Recently, NIPS was used to detect rare autosome trisomies, sex chromosome aneuploidies, and microdeletion or microduplication syndromes.15 16 However, monogenic disorders which represent another major cause of birth defects are beyond the scope of the current screening of chromosomal abnormalities, and the clinical validity for the screening of such diseases are yet to be demonstrated.
The development of NIPS for monogenic disorders
Previous studies have shown that the analysis of fetal cfDNA was useful to determine the inheritance of parental alleles associated with autosomal or sex-linked recessive monogenic diseases.17 18 Additionally, non-invasive prenatal testing was also accurate for the diagnosis or screening of the de novo or paternally inherited variants causing dominant diseases such as achondroplasia and Noonan spectrum disorders.19 20 These studies showed potential clinical utility for monogenic NIPS (NIPS-M) in pregnancies at moderate risks (eg, pregnancies with advanced paternal age or ultrasound soft markers). These tests could also be used for the screening of diseases which can only be discovered at late gestational ages (eg, skeletal disorders). Although the analytical accuracy of NIPS-M has been well demonstrated, such tests will not be widely accepted without further evidence-based clinical study.21 First, the clinical validity of NIPS-M has not been supported by large prospective studies. The follow-up studies of the pregnancies tested positive or negative should be evaluated by clinical examination or golden standard diagnostic tests. Additionally, although isolated cases have demonstrated the benefits of NIPS-M leading to early diagnosis and better prenatal/postnatal management, the benefits for the management of patients with different indications are yet to be explored by larger studies.20 22 23 Third, the limitations of NIPS-M need to be evaluated. Accurate genetic counselling is critical to the success of a prenatal screening test which should provide information regarding disease characteristics, natural history, penetrance, expressivity, genotype-phenotype correlation, etc. The benefits and risks of NIPS-M need to be carefully evaluated when patients are counselled based on current understanding of the diseases.24
This study is aimed to address above important issues with a focus on the clinical validation of an innovative NIPS for concurrent screening of common aneuploidies, CNVs and monogenic disorders. The potential benefits and the limitations of this screening test will also be explored based on the pregnancy outcome data.
Aims
To assess the clinical validity of a novel NIPS test for concurrent screening of seven common aneuploidies, nine microdeletion and microduplication syndromes (MMS) and 155 monogenic disorders (75 genes).
To evaluate the pregnancy outcome for the participants of this comprehensive NIPS.
Methods and analysis
Study design
This prospective cohort study aims to evaluate how a comprehensive NIPS test will reveal pregnancies at risks for both chromosomal and monogenic disorders. It is a prospective, multicentre study focused on pregnant women with indications for prenatal diagnosis, including fetal ultrasound markers, high risk results by maternal serum screening or routine aneuploidy NIPS. Pregnancies with elective abortion due to fetal structural abnormality will also be recruited. To assess the performance metrics of this NIPS test, cases will be followed up to compare the screening results with the prenatal or postnatal diagnostic test results including sequencing, chromosomal CNV testing and/or karyotyping. Clinical follow-up will be pursued regarding the pregnancy outcome up to 6 weeks after birth (figure 1).

The diagram for the clinical validation of a comprehensive non-invasive prenatal screening test.
Consent and eligibility
Participants will be recruited from three tertiary hospitals in China including the Obstetrics and Gynecology Hospital of Fudan University (Shanghai), the Hunan Provincial Maternal and Child Health Care Hospital (Changsha), and the Women’s Hospital of Zhejiang University (Hangzhou). The detailed descriptions of inclusion and exclusion criteria are shown in table 1. Pre-test genetic counselling will be provided by healthcare providers to all participants before obtaining the written informed consent to complete enrollment. The purpose and process of this study, as well as potential benefits, risks, data privacy and rights to withdraw will be discussed during the counselling session.
Inclusion and exclusion criteria
Patient and public involvement
Patients or the public were not involved in the design, conduct, or dissemination plans of this research.
Sample size
This study aims to recruit at least a total of 1000 pregnancies undergoing invasive diagnostic procedures or elective abortions due to abnormal prenatal findings suggestive of severe genetic disorders. All eligible subjects will be stratified into different indication groups (table 1), and the number of subjects in each group will be approximately allocated as the following: group 1, fetal structural anomalies detected by ultrasound (60%); group 2, high risk by routine NIPS (20%); group 3, high risk by maternal serum biochemical testing (10%); group 4, suspected genetic causes with other indications (10%). For group 1, further stratification will be achieved based on the gestational age, including 12–16 weeks, 17–21 weeks and 22 weeks and above (table 1). The number of subjects from each hospital will be evenly collected given equal participant availability. In this study, at least 1000 participants will be enrolled from whom we expect to detect at least 25 cases affected with a targeted monogenic or chromosomal disease each. This estimation is based on the detection rate among pregnancies with similar indications.25–27 The sample size in this study allows a probability of 95% or above to observe a possible measuring error at the case level for both the monogenic diseases and chromosomal diseases.
Screening and reporting
The comprehensive non-invasive prenatal screening test used in this study was developed by Beijing BioBiggen Technology Co. (Beijing, China). This test is based on liquid-phase target enrichment followed by high read-depth NGS which can concurrently detect a panel of preselected diseases consisted of 7 common chromosomal aneuploidies, 9 MMS, and 155 monogenic disorders (table 2 and online supplemental table S1). A total of 10 mL peripheral blood is collected from each participant and the plasma is separated through a standard two-step centrifugation process. Manufacturer protocols are used for cfDNA extraction (TIANGEN, China) and NGS library construction (Nanodigbio, China). Custom designed hybridisation probes are synthesised and used for target enrichment (Integrated DNA Technologies, USA). The final DNA library is sequenced at 2×100 paired-end mode on MGISEQ-2000 sequencer (MGI, China).
Supplemental material
The list of diseases and genes included in the screening test
The pathogenicity for both chromosomal and monogenic variants is evaluated according to the American College of Medical Genetics guidelines.28 29 Only pathogenic and likely pathogenic variants are deemed positive and reportable to patients after diagnostic confirmation. For cases with chromosomal abnormalities identified in the NIPS test, karyotyping, chromosomal microarray analysis, and whole genome sequencing for copy number variation analysis are used as diagnostic tests. For cases with screening positive monogenic variants, Sanger sequencing is used as the confirmatory test. Post-test genetic counselling is provided to participants by experienced clinical geneticists regarding the interpretation of the diagnostic results, the implications of these positive findings, and potential management options.
Pregnancy outcomes follow-up
All screening and diagnostic testing results, clinical examination results and images, and other relevant information available to us will be collected in the participants’ medical records and used for statistical analysis. All cases will be followed up for pregnancy outcome including elective abortion, miscarriage, stillbirth or live birth. Newborns will be followed up for birth records and clinical examination or diagnostic testing up to 6 weeks of age. Subjects with positive NIPS results who do not have diagnostic genetic test results are excluded from the cohort. Subjects with negative diagnostic testing results, normal results in newborn physical examination or a genetic aetiology established for diseases other than those included in our screening panel are considered as negative cases.
Statistical analysis
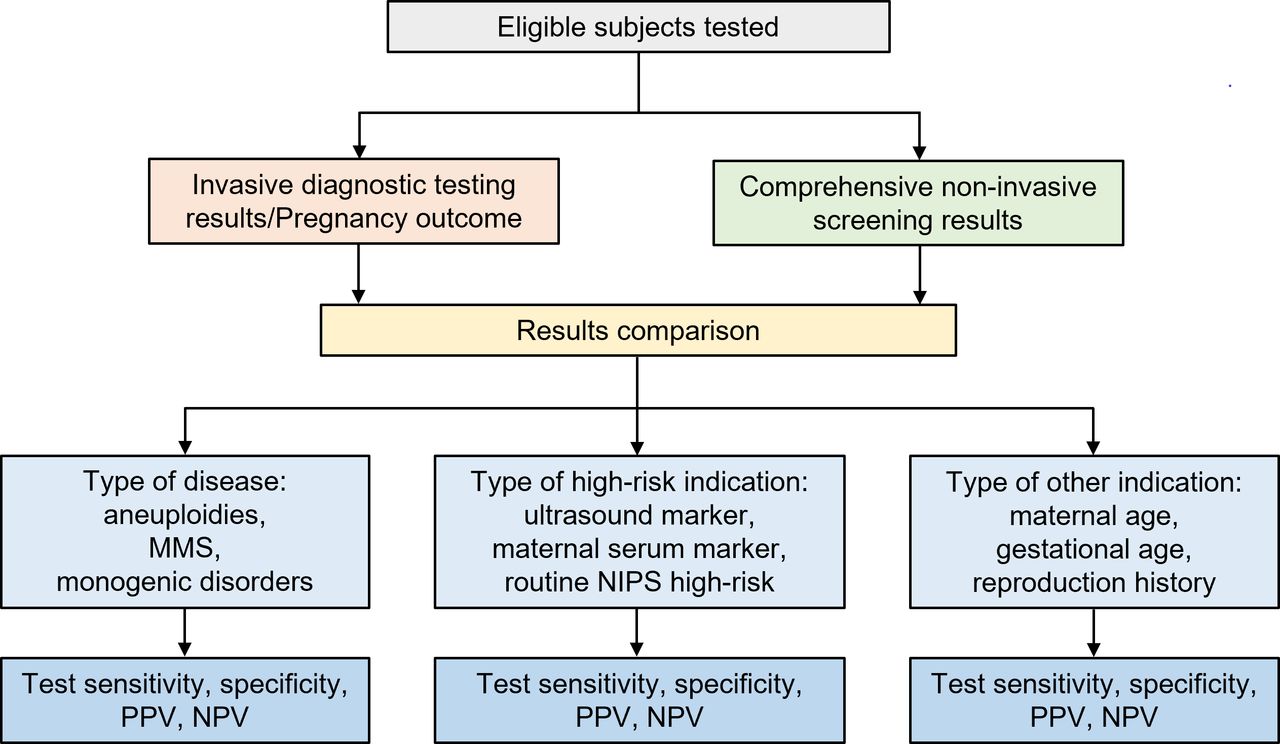
The diagnostic testing and pregnancy outcome results of all pregnancies will be used to compare with the results generated by our NIPS test. The outcome is the area under the receiver-operating characteristic (ROC) curve for detection of each type of abnormalities (aneuploidies, MMS, and monogenic disorders) by NIPS in high-risk pregnancies. The ROC curve is generated by computation of test sensitivity and specificity, and CIs are computed using the Clopper–Pearson method. Assay performance metrics will also be demonstrated by false positive rate, false negative rate, positive predictive value, and negative predictive value, according to each category of abnormalities (figure 2). Data will be analysed with respect to different groups of indications for high-risk pregnancies, as well as pregnancies at different maternal age or gestational age.

{kind=link}
{kind=link}
The diagram for the screening result analyses based on different disease types and indications. MMS, microdeletion and microduplication syndromes; NIPS, non-invasive prenatal screening; PPV, positive predictive value; NPV, negative predictive value.
Study conduct
In this study, subjects’ demographic and clinical exam data are collected from test requisition forms, hospital medical records and postnatal follow-up surveys. Site monitoring of source data is performed following the study monitoring plan. All patents’ privacy information collected during the study will be kept strictly confidential. Study data will be held securely on paper or electronically at the Obstetrics and Gynecology Hospital of Fudan University. Data safety will be reviewed on a regular basis to identify any safety concerns or trends.
Ethics and dissemination
This study was approved by the Obstetrics and Gynecology Hospital of Fudan University (2020-178). Results of this study will be disseminated to public through scientific conferences and a peer-reviewed journal. Written informed consents will be obtained from participants. Deidentified participant data such as the screening and diagnostic results along with pregnancy outcome data will be shared at the individual or aggregative level. The assay protocols, clinical study protocol, statistical analysis plan, will be shared for at least 5 years after the clinical study is completed. The data will become available within 1 year after the clinical study is completed. All essential data supporting the conclusion of the study as well as detailed assay protocols, analytical algorithms, and customised computational codes will be submitted for publication within 1 year after the clinical study is completed. All the disease-causing variants and the key phenotypes found in the subjects will be published or deposited at a public database. Subjects’ identifiable information including their genomic sequencing data will be kept in a clinical and privacy-compliant laboratory. Non-identifiable sequencing data (eg, individual variant data generated by locus-specific sequencing) can be provided on request from the corresponding author (Dr. Jinglan Zhang, jinglanzhang@foxmail.com) for at least 5 years after the clinical study is completed.
Discussion
This is the first study to evaluate the clinical validity of an integrated non-invasive prenatal screening for both chromosomal abnormalities and monogenic disorders. Although NIPS for common aneuploidies has been accepted by professional societies and widely implemented around the world, NIPS for frequent chromosomal CNVs and monogenic disorders requires evidence-based investigation to prove its validity and its potential for pregnancy management. To investigate the performance of this new NIPS test, high-risk pregnancies are selected based on the routine prenatal screening results suggestive of genetic diseases and stratified into different groups. Diagnostic testing results together with pregnancy outcome data will be obtained for the clinical validation. Additionally, important practical issues around this test will be explored and discussed. For instances, the criteria for the selection of diseases, the proper indications for this test, genetic counselling and pregnancy management options will be evaluated based on the detection rate and pregnancy outcome to weigh the benefits and risks when offering a comprehensive NIPS test for different types of diseases. It should be noted that this study is observational, and all high-risk pregnancies recruited will be counselled by clinicians following current clinical guidelines for prenatal care. Patients’ decisions regarding whether to take invasive diagnostic testing or how to proceed with their ongoing pregnancy will not be intervened by the screening results of this test unless it is confirmed by diagnostic testing. Previous studies (online supplemental table S2) assessing the clinical validity of aneuploidy or chromosomal CNV prenatal screening were also observational although most of these studies were conducted at an early gestational age when different pregnancy managing options are possible.14 15 30 31 The primary goal for this study is to assess the clinical validity of this new comprehensive NIPS test in a high-risk population in which abnormal prenatal screening results are mostly discovered at a late gestation age. Therefore, redirecting ongoing pregnancy can be challenging when the diagnostic test result is not available in time. Future study on general pregnancy population will be performed to investigate how this test may impact the prenatal or postnatal management at an early gestation age.
Overall, in this prospective, multicentre study, we will provide invaluable data to assess the clinical validity of a novel comprehensive NIPS test for the concurrent screening of chromosomal and monogenic disorders. This test has the potential to be offered as an expanded and a next-generation NIPS test for general pregnancy population.
Ethics statements
Ethics approval
This study had been reviewed and approved by the Obstetrics and Gynecology Hospital of Fudan University (2020-178).
Acknowledgments
The technology development for this work was supported by Beijing BioBiggen Technology Co., Ltd.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
CX, XC and SC contributed equally.
Contributors JZ and H-FH conceived the study. JZ, H-FH, YW, CX and XC participated in the design of the study and drafting of the manuscript. CX, SC, QL, HX, DZ and HW participate in recruitment of participants and assessment of clinical outcomes. XC and JZ will design the statistical analysis plan and oversee statistical analysis. All authors critically reviewed and approved the manuscript for submission.
Funding This study was supported by The National Key Research and Development Program of China (2020YFA0804000) and the National Natural Science Foundation of China (82071661). The clinical validation and research work were partially supported by Technology Innovation Project of Shanghai Shenkang Hospital Development Center (SHDC12019107 and SHDC12018X17), the International Science and Technology Collaborative Fund of Shanghai (18410711800), the National Natural Science Foundation of China (81661128010), CAMS Innovation Fund for Medical Sciences (2019-12M-5-064), National Key Research and Development Program of China (2018YFC1002804), Program of Shanghai Academic Research Leader (20XD1424100), Outstanding Youth Medical Talents of Shanghai Rising Stars of Medical Talent Youth Development Program, Clinical Research Plan of Shanghai Shenkang Hospital Development Center (SHDC12018X17), and Clinical Research Project of Shanghai Municipal Health Commission (201840210, 20184Y0349). The cost of sample processing and high-throughput sequencing was supported by Beijing BioBiggen Technology Co., Ltd.
Competing interests XC, JZ are employees or shareholders of Beijing BioBiggen Technology Co. The other authors declare no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.