Article Text

Abstract
Objective To evaluate the impact of a television advertising campaign on the risk of oral ingestion of a topical non-prescription gynaecological preparation containing benzydamine hydrochloride.
Design An interrupted time series design with data routinely collected.
Setting A National Poison Control Centre.
Participants 215 cases of hazardous exposure to the preparation under study occurred in Italy from January 2005 to December 2010.
Primary and secondary outcome measures Mean daily rate of cases of exposure by gender in three different periods, that is, pre-advertisement period, before the advertisement was broadcast (from 1 January 2005 to 19 December 2009), advertisement period, when the advertisement was repeatedly launched (from 20 December 2009 to 27 February 2010), post-advertisement period (from 28 February 2010 to 6 March 2010); observed/expected ratios of cases, with expected cases based on data from the pre-advertisement period, adjusted for estimated variations in the number of users. Comparison of the distribution of the main characteristics of cases in the three different periods by means of Pearson's χ2 test or Fisher's exact test.
Results The adjusted observed/expected ratio of cases in women was 7.48 (95% CI 5.76 to 9.56) in the advertisement period and 2.97 (95% CI 2.24 to 3.85) in the post-advertisement period. Regarding the characteristics of cases, there was an increased proportion of cases of exposure due to confusion about the correct administration route in the advertisement and post-advertisement periods (81% and 55%, respectively, compared to 16% for the pre-advertisement period.) and of individuals with clinical effects (55%, 52% and 27%, respectively).
Conclusions In Italy, an advertisement for a non-prescription medicine seems to have confused consumers regarding the administration route. This effect was observed even after the advertisement had stopped being broadcast. These results highlight the need for the monitoring of medication errors and adverse effects before, during and after advertising.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
The study is focused on documenting the impact of television advertising on the safe use of a benzydamine hydrochloride-containing gynaecological preparation in Italy.
Key messages
Advertising can affect the safe use of medicine. Select outcomes, such as medication errors, should be carefully monitored before, during and after advertising campaigns. To this end, poison control centres can be extremely useful.
Strengths and limitations of this study
The study is based on routinely collected and readily available data (ie, reports and telephone calls made to a National Poison Control Centre), which allowed for the comparison of the main characteristics of cases of dangerous exposure to a medicine and for the evaluation of the association between the occurrence of cases and a television advertising campaign. The main potential limitation is that the data were provided on a voluntary basis to the poison control centre, so that they may not be representative of all cases occurring in the general population.
Introduction
Benzydamine hydrochloride (BHC) (CAS no. 132-69-4) is a local anti-inflammatory and analgesic active ingredient first synthesised by the Angelini research laboratories in the mid-1960s. Since then, topical preparations containing BHC have been marketed worldwide for the symptomatic treatment of oropharyngeal and gynaecological conditions.1 These preparations are sold as concentrated or ready-to-use solutions or as a powder to be dissolved in water. Topical preparations of BHC are usually well tolerated, with infrequent side effects.2 Absorption through the skin and mucosa is low, whereas experimental data indicate that BHC is rapidly absorbed in the gastrointestinal tract.3 4 A limited number of reports on acute oral exposure in humans have shown that BHC overdose can cause nausea, vomiting, visual hallucinations, oesophageal irritation, agitation and somnolence.5–8 These effects have resulted mainly from the ingestion of gynaecological preparations because of confusion about the correct administration route and the preparations being mistaken for oral medicines.8 A few cases of injuries due to intentional ingestion for recreational use have also been reported.7 9
In Italy, from 1977 to 2009, BHC-containing gynaecological preparations manufactured by Angelini were classified as pharmacy-supervised drugs (sold under the supervision of a pharmacy), a category of non-prescription drugs for which advertising to the public is prohibited. In April 2009, these preparations were reclassified as over-the-counter (OTC) drugs with the following therapeutic indications: vulvovaginitis of any origin or nature, characterised by small vaginal discharge, itching, irritation, burning and vulvar pain; and personal hygiene during puerperium. The label on the package was changed from ‘vaginal solution’ to ‘cutaneous solution for external genital organs’.10 Given the drug's new status, advertising to the public was allowed, and the manufacturer launched an intensive television advertising campaign between 20 December 2009 and 2 January 2010, followed by a second campaign between 17 and 23 January 2010. The advertisement focused on solidarity among women and on their ability to solve their ‘intimate problems’ by using the advertised preparation. At the end of the advertisement, an allusion was made to the mode of use, with a woman's silhouette with concentric circles on the abdomen.
During the first television campaign, the National Poison Control Centre in Milan (PCCM) observed an unexpectedly increased number of requests for assistance for cases of unintentional oral ingestion (ie, from approximately one case per month to two cases per day). Based on these findings, the Italian Ministry of Health required that the advertisement be revised to clarify that the product was for topical use. The advertisement was rebroadcast between 21 and 27 February 2010, with a written statement at the end of the advertisement stating that the preparation was for topical use only and a woman's silhouette with concentric circles on the pubis area. Afterwards, the advertisement was voluntarily stopped by the manufacturer. The objective of the present study was to document how unintentional oral exposure to BHC-containing gynaecological preparations was inadvertently promoted by television advertising in Italy.
Materials and methods
Each year, the PCCM receives approximately 42 000 reports of human exposure to different types of substances,11 accounting for more than 60% of all cases referred to Italian PCCs.12 The PCCM mainly provides consultation to hospitals (60% of cases) and to the general public (30% of cases) throughout Italy. Assistance for diagnosing and treating poisonings is provided by medical toxicologists, mainly over the phone. For each case, the toxicologist collects the following data in real time using a standard form: demographic characteristics, exposure characteristics (eg, substance/commercial product, route of exposure, reason for exposure, dose and latency between exposure and onset of clinical effects), signs and symptoms, therapy and outcome. About 45% of the human exposures managed by the PCCM are medicine-related; of these, about 17% are victims of the inappropriate use of medication.13
For the present study, the PCCM database was searched from 1 January 2005 to 31 December 2010 to identify all cases of inappropriate exposure to the BHC-containing gynaecological preparation, which is available in diverse forms (ie, concentrated solution, ready-to-use solution and powder). A clinical toxicologist (FD) reviewed the available information for data consistency and to grade the severity of outcome according to the Poisoning Severity Score (ie, none, no signs/symptoms; minor, mild, transient and spontaneously resolving signs/symptoms; moderate, pronounced or prolonged signs/symptoms; severe, life-threatening signs/symptoms or resulting in significant residual disability or disfigurement; fatal, death as a result of exposure or of direct complications of the exposure effects).14 For the purposes of the present analysis, the identified cases were classified into three groups based on exposure period: (1) the pre-advertisement period (ie, from 1 January 2005 to 19 December 2009), before the advertisement was broadcast; (2) the advertisement period (ie, from 20 December 2009 to 27 February 2010), when the advertisement was repeatedly launched, plus the week following the last day of broadcast (ie, from 28 February 2010 to 6 March 2010), assuming that the advertisement still had an effect and (3) the post-advertisement period (ie, from 7 March 2010 to 31 December 2010).
The mean number of packages sold per day during these periods was estimated based on the information provided by the manufacturer on the number of packages sold per month from November 2009 to October 2010 We assumed that the sales during the pre-advertisement period remained constant; we thus decided to calculate the mean number of packages sold per day based on sales in November 2009 (n=83 745, corresponding to 2791 packages/day). Since the first 20 days of December were included in the pre-advertisement period, the quantity assumed to be sold in these 20 days (55 820 packages) was based on the estimated daily sales in November 2009. This quantity was subtracted from the total number of packages sold in December (n=173 724). The remaining quantity (117 904 packages) was used to estimate the mean number of packages/day sold in the period 20–31 December (n=10 718) under the assumption that the observed increase was completely driven by advertising. During the entire advertisement period, an estimated mean of 8381 packages/day were sold, whereas in the post-advertisement period, a mean of 4764 packages/day were estimated to be sold. The ratio of advertisement period sales to pre-advertisement sales and the ratio of post-advertisement sales to pre-advertisement sales were calculated as an indicator of the increased number of users (ie, the population at risk of exposure). These ratios corresponded to a 3.0-fold mean increase in the advertisement period (range, by calendar month: 2.1–3.8) and a 1.7-fold mean increase in the post-advertisement period (range, 1.2–2.1).
The mean daily rate (ie, the mean number of cases of exposure/day) by gender and period was calculated, as were the 95% CIs, assuming a Poisson's process. In the pre-advertisement period, the mean daily rate for both men and women was assumed to be constant over time and used to estimate the expected number of cases in the advertisement and post-advertisement periods. These expected values were adjusted by the estimated increases in the population at risk of exposure in the two periods. The ratio of observed to adjusted expected cases (O/E) was used as a measure of the association between inappropriate exposure and television advertising. The 95% CIs of the O/E ratio were derived assuming a Poisson's process for the observed cases.15 The main characteristics of cases in the three periods were compared using Pearson's χ2 test or Fisher's exact test.
Results
A total of 215 cases of oral exposure to the advertised gynaecological preparations were identified. Of these, 187 were women and 28 were men. All cases were unintentionally exposed through oral ingestion, with the exception of one man who intentionally ingested the preparation.
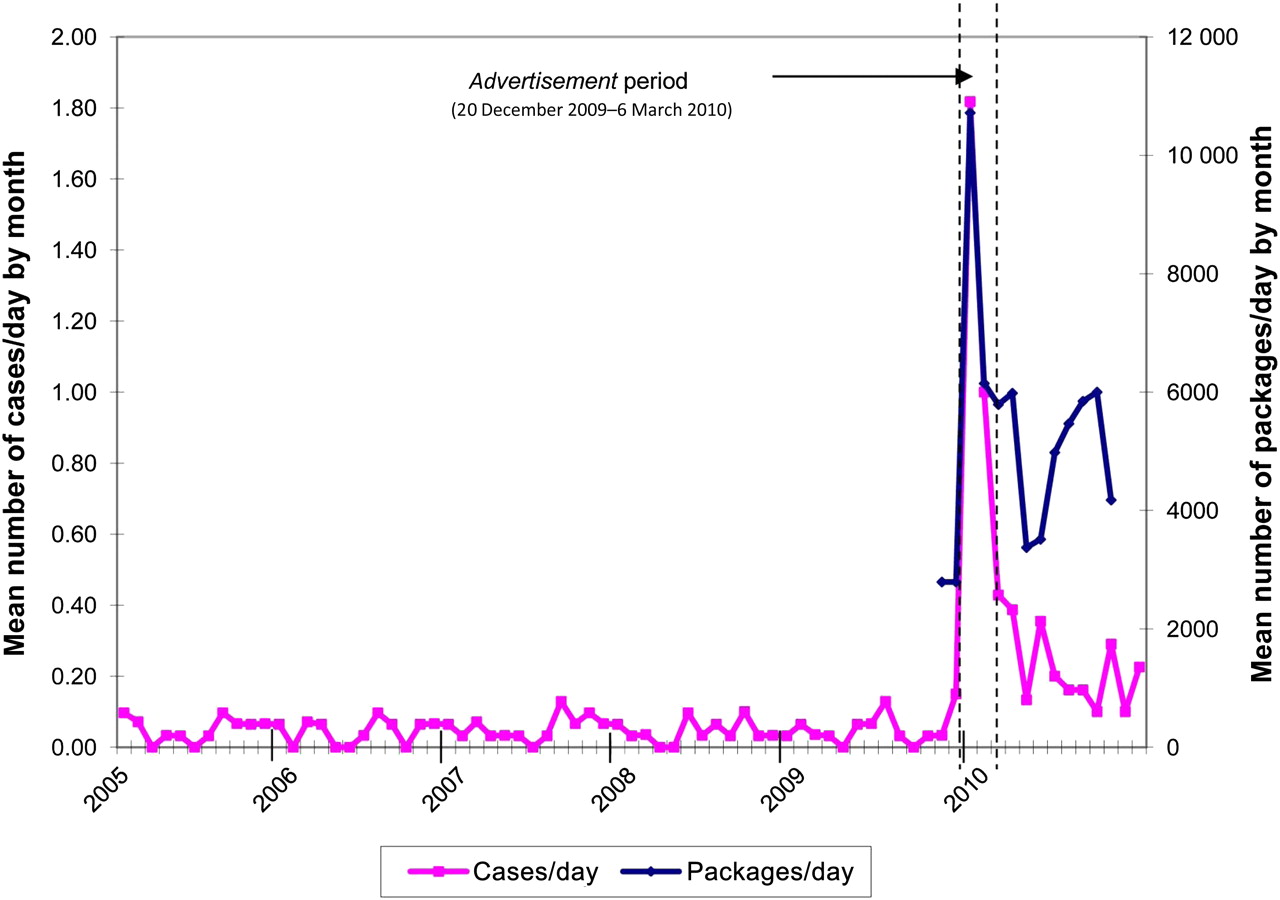
The mean number of cases/day observed by month in the three different periods is shown in figure 1; the mean number of packages sold per day is also shown. In the pre-advertisement period, there were 15–20 cases/year and 0–4 cases/month. The mean number of cases/day by month ranged from 0.00 to 0.15. In the advertisement period, 1.85 cases/day were observed during the last 10 days of December, which were completely covered by the first advertising campaign. In January, 1.00 cases/day were observed; the beginning of this month was covered by the first advertising campaign, which was broadcast until 2 January, and, subsequently, from 17 to 23 January by the second advertising campaign. In February, 0.48 cases/day were observed; the third advertising campaign was broadcast from 23 to 27 February. The estimated number of packages sold per day varied from 10 718 in the last 10 days of December, to 6142 in January, and to 5788 in February. During the post-advertisement period (ie, from 7 March 2010 to 31 December 2010), the mean number of cases/day ranged from 0.10 to 0.35. The estimated number of packages sold per day ranged from 6000 to 3373.

{kind=link}
Distribution by month of the mean number of cases/day exposed to benzydamine hydrochloride-containing gynaecological preparation reported to the National Poison Control Centre in Milan 2005–2010 and the mean number of packages/day sold in Italy between November 2009 and October 2010.
The distribution of cases by gender and period and the corresponding daily rates are shown in table 1. The observed/expected ratios, adjusted by the estimated increase in the population at risk of exposure (ie, 3.0- and 1.7-fold increase in the advertisement and post-advertisement period, respectively), are also shown. In the pre-advertisement period, 67 cases occurred in women, accounting for 0.04 cases/day (95% CI 0.03 to 0.05) and 20 cases occurred in men (0.01 cases/day, 95% CI 0.01 to 0.02). In the advertisement period, in women, there were 64 observed cases and 8.55 expected cases (O/E 7.48, 95% CI 5.76 to 9.56), whereas in men, the observed cases were close to the expected ones (3 vs 2.54, O/E 1.18, 95% CI 0.24 to 3.45). In the post-advertisement period, in women, there were 56 observed cases and 18.87 expected cases (O/E 2.97, 95% CI 2.24 to 3.85). In men, there were five observed cases and 5.63 expected cases (O/E 0.89, 95% CI 0.29 to 2.07).
Mean daily rates and observed/expected ratios of ingestion of a benzydamine hydrochloride-containing gynaecological preparation reported to the National Poison Control Centre in Milan in 2005–2010
The main characteristics of female cases by period of exposure are reported in table 2. In the advertisement and post-advertisement periods, the percentage of women (95% and 92%, respectively) was significantly higher than that in the pre-advertisement period (76%, p=0.001 and 0.025, respectively). The percentage of individuals who were hospitalised in the advertisement period (52%) was slightly higher, though not significantly, than that in the pre-advertisement (42%) and post-advertisement (43%) periods. When comparing cases in the pre-advertisement and advertisement periods, significantly different distributions were found for age class (p=0.003), reason for exposure (p<0.001) and medical outcome (p=0.002). In particular, the advertisement period, compared to the pre-advertisement period, was characterised by a predominance of cases aged 20–49 years (77% vs 46%), medication error due to misunderstanding of the correct mode of use (81% vs 16%) and individuals suffering recognised BHC-related effects (55% vs 27%). In the post-advertisement period, the distribution of cases by age was comparable to that reported in the pre-advertisement period, whereas significant differences were found for the distribution of cases by reason of exposure (p<0.001) and medical outcomes (p=0.005).
Main characteristics of female cases of ingestion of a benzydamine hydrochloride-containing gynaecological preparation reported to the National Poison Control Centre in Milan in 2005–2010
Altogether, 82 women suffered recognised BHC-related effects. The severity of medical outcomes was minor in 70 women (85%) and moderate in 12 (13%). No severe or fatal effects were observed. The signs and symptoms most frequently associated with BHC ingestion included vertigo (n=26), pyrosis (n=25), oropharyngeal irritation (n=19), vomiting (n=19), nausea (n=14), hallucinations (n=7), pharyngeal pain (n=6) and headache (n=6) (table 2).
With reference to men exposed in the pre-advertisement period (n=20), 50% mistook a BHC solution for drinking water or other beverage, whereas for the remaining 50%, the exposure was due to confusion with other medicine. Similarly, in the advertisement period, two cases reported having mistook a BHC solution for a beverage and one for another medicine. Among the five cases detected in the post-advertisement period, in one case the exposure was due to intentional abuse; one case each mistook the solution for a beverage or another medicine. Altogether, six patients were symptomatic and suffered oropharyngeal irritation (n=3) and vomiting (n=3).
Comments
In the European Community, advertising to the public is only allowed for medicinal products that are classified as ‘not subject to medical prescription’,16 commonly referred to as ‘OTC’. This classification should be based on an evaluation of the balance between the potential benefits of the products being readily available for self-treatment and the potential harm resulting from unsupervised or inappropriate use. Thus, the safety of OTC medicines needs to be continuously monitored, to identify unforeseen problems and implement suitable interventions to minimise the potential for harm.17–19
Advertising to the public is a source of information that tends to emphasise the beneficial effects of the advertised product,20 which could inadvertently contribute to unnecessary or inappropriate use. However, the impact of advertising to the public on the safe use of non-prescription medicines has only been studied to a limited extent.21 22
Some studies have shown that self-medication of vaginal conditions with OTC antifungal preparations is associated with unnecessary use and a delay in proper diagnosis and treatment.23 24 With specific regard to BHC-containing gynaecological preparations, a study in Spain has shown a high frequency of medication error due to misunderstandings about the correct administration route.8
In Italy, until April 2009, BHC-containing gynaecological preparations had been classified in a category of medicines that can be obtained without a prescription yet for which advertising to the public is not allowed. The re-classification as ‘OTC’ was not associated per se with an increase in cases of exposure (figure 1) or with changes in the case distribution by gender or other characteristics. Instead, the daily rate of cases of exposure reported to the National PCCM increased abruptly in association with television advertising, and this increase can be explained only in part by the increased number of users. In particular, during the first advertising campaign (ie, 20 December 2009–2 January 2010), there was a 17.5-fold increase in the daily rate of cases of oral exposure compared to the pre-advertisement period, but only a 3.8-fold increase in the number of users; when adjusting for the number of users, there was still a 9.5-fold increase in the daily rate of cases. The analysis of the observed/expected ratio, which was performed taking into account a mean 3.0-fold increase in the number of users during the advertisement period, showed a statistically significant 7.5-fold increase in the risk of exposure in association with advertising. In the post-advertisement-period, when the estimated number of users was on average 1.7-fold higher than that in the pre-advertisement period, the risk of exposure was approximately three times higher than that in the pre-advertisement period, suggesting that the advertisement had a long-lasting effect.
The comparison of the main characteristics of female cases in the different periods revealed an abrupt increase in association with advertising not only for the occurrence of cases but also for the percentage of cases due to misunderstandings about the administration route, which was the main reason for exposure during the advertisement period. In the last 11 days of December, which fell within the period of the first advertising campaign, 100% of the female cases were exposed because of confusion over the administration route; this percentage was 81% when considering the entire advertisement period, whereas in the 5-year pre-advertisement period, it was only 16% (table 2). The television advertisement, which was discontinuously broadcast, emphasised the ability of women to achieve a quick remission of their ‘intimate problems’ by simply going to a pharmacy and buying the product. During the first two campaigns, the advertisement did not contain any direct indication of the mode of use. In the third campaign, it included a written statement that the preparation was for topical-only use. However, this attempt at clarification did not seem to have any effect, given that nine of the 11 cases observed during the last advertising campaign were exposed because of incorrect administration route, though there are too few cases to make a definitive conclusion. The percentage of women who misunderstood the correct mode of use decreased during the post-advertisement period, yet it remained higher than that in the pre-advertisement period, indicating that the misleading effect of the advertisement was long lasting.
A strength of this study was that it was based on routinely collected and readily available data and that during the study period the means of collecting data did not change. However, a potential limitation of the study is that there may have been a selection bias in the population, which consisted of reports provided on a voluntary basis to the National PCCM. Nonetheless, the observed increase in the risk of exposure due to an incorrect administration route can hardly be explained by selection bias and can be reasonably considered to be indicative of an increased risk of this type of incident among users in the general population.
The reported findings document how advertising to the public can negatively affect the correct use of an OTC medication, highlighting the need for monitoring select outcomes, such as medication errors and adverse effects, before, during and after advertising campaigns. Data routinely collected by PCCs, although referring to a select subset of cases of dangerous exposure and poisoning, can be useful in advertising surveillance and provide valuable information for regulatory agencies.
Acknowledgments
The authors wish to thank the staff of the National PCCM for having collected the data (Fabrizio Sesana, MSc; Maurizio Bissoli, MD; Rossana Borghini, MD; Tiziana Della Puppa, MD; Valeria Dimasi, MD; Marcello Ferruzzi, MD; Ilaria Rebutti, MD; Paola Moro, MD; Angelo Travaglia, MD; Francesca Assisi, MD; Paolo Severgnini, MD; Tania Giarratana, MD; Mrs Antonella Pirina). They also thank Mr Mark Kanieff for his useful comments and language editing.
References
Footnotes
To cite: Settimi L, Davanzo F, Lauria L, et al. Oral ingestion of a topical benzydamine hydrochloride-containing gynaecological preparation in association with television advertising in Italy: analysis of cases managed by a National Poison Control Centre. BMJ Open 2012;2:e000204. doi:10.1136/bmjopen-2011-000204
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed the Unified Competing Interest form at http://www.icmje.org/coidisclousure.pdf (available on request from the corresponding author) and declare that all authors had (1) no financial support for the submitted work as declared above; (2) no financial relationships with commercial entities that might have an interest in the submitted work; (3) no spouses, partners, or children with relationships with commercial entities that might have an interest in the submitted work and (4) no non-financial interests that may be relevant to the submitted work.
Ethics approval Data were anonymous and based on routinely collected medical information. No ethics approval was required.
Contributors LS developed the research proposal, planned the study design and the analysis and drafted and edited the paper. FD was responsible for data collection and assessment of severity of cases and contributed to editing the paper. LL contributed to planning and performing the analyses and to drafting and editing the paper. MLC and FF contributed to editing the paper and are guarantors.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement http://bmjopen.bmj.com.ezproxy.u-pec.fr/site/about/resources/datamanagement.xhtml". The authors agree to honour any reasonable request by other researchers for materials, methods or data necessary to verify the conclusion of the article.