Article Text

Abstract
Introduction The effects of bariatric surgery have largely been studied from a medical viewpoint, seeking to measure changes in anthropometric, physiological or quality-of-life factors after the operation. Few studies, however, have focused on the dynamics of lifestyle changes. Yet we know that changing lifestyle habits—which are often part of the established social configurations at the origin of morbid obesity—is essential for a sustainable recovery from obesity. We also know that the major bodily transformations that occur in the six to twelve months following surgery produce a high degree of biographical uncertainty and affect social interactions. From a sociological perspective, the authors propose to study the processes of disruption and re-establishment of lifestyle habits in the first 24 months following bariatric surgery.
Methods and analysis The ChiBarAPS study relies on a mixed-method longitudinal survey, comprising three components: qualitative, quantitative, literature and data review. It aims to document three main dimensions, which must be articulated to understand the dynamics of change: (1) the work undertaken by patients on themselves in order to identify and measure the evolutionary effects of surgery, as well as to adapt to them; (2) the experience of using pre- and post-surgery information and support systems, and evaluating their effects on the agency of the people who have undergone surgery; (3) the evolution of social participation and lifestyle habits. The qualitative component concerns a cohort of 30 patients, interviewed in depth (2 hours) on these three dimensions, 6 months, 12 months and 24 months after the operation. The quantitative part uses questionnaires applied to a second group of 200 patients, following the same timeline.
Ethics and dissemination This study complies with reference methodology MR004 of the French National Data Protection Authority and was registered by the Data Protection Officer of the University of Montpellier on the activity registry of the institution (24 April 2024). Ethics approval has been obtained from the University of Montpellier ethics research board (n°UM2024-037). Informed consent will be obtained from all participants before data collection. The project has received funding from the French National Research Agency (n°ANR-23-CE41-0020-01) from February 2024 to the end of January 2028. The first results of the research will be disseminated from 2026 onwards to researchers, health professionals and patient support organisations. The results of the study will then be published in peer-reviewed scientific journals, both national and international.
- Bariatric Surgery
- Obesity
- Physical Fitness
- Quality of Life
- Life Change Events
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The research uses a multicentre, longitudinal, mixed-method approach capable of capturing the biographical uncertainties that mark the 2-year period following sleeve-type bariatric surgery.
The longitudinal approach makes it possible to capture social processes in the making, but involves repeating interviews and questionnaires with the same panels at 6, 12 and 24 months after surgery, meaning that we must be careful to limit the number of people lost to follow-up.
The sociological approach, which is attentive to the social processes that follow and are consubstantial with weight loss—but more for its own sake than for assessing the effects of certain social variables on the success or otherwise of the operation, or of the operation on certain social components—will provide a demedicalised understanding of the experience of overcoming obesity through bariatric surgery.
The fact that the samples were recruited mainly through public hospital partners may lead to an under-representation of the specific experiences of people operated on in private clinics, and the fact that recruitment was on a voluntary basis may lead to an over-representation of certain experiences, which we will have to try to identify.
Introduction
The health benefits of bariatric surgery have been extensively studied. Although maintaining these benefits requires a lasting change in those lifestyle habits considered to be at the origin of morbid obesity, few studies have questioned the conditions for such a change.
Health and quality of life impacts
Medical literature positively assesses the benefit/risk ratio of bariatric surgery by comparing metabolic improvements due to weight loss and the risks of death or side effects related to the surgery.1 Complications and dietary constraints (in particular to limit gastro-oesophageal reflux and avoid nutritional deficiencies) following the surgery are well documented.2 3 However, Stevens’s sociological approach4 points to the effort of redefining the physiological symptoms experienced by patients after surgery. Indeed, the latter perceive these symptoms rather as a tool for strengthening self-control, or as signs of weight loss synonymous with health gain, than from the perspective of illness or disability.
Surgery is also a source of stress and anxiety, before and after the operation. Measured using psychometric scales, these emotional difficulties expose patients to addictive behaviours and eating disorders.5–7 They can also lead to depressive symptoms related to the feeling of not being able to follow medical recommendations.8–10 Post-surgery quality of life is studied using specific scales, such as Bariatric Quality of Life11 or Bariatric Analysis Reporting Outcome System.12 These scales consider the impact of the operation in terms of: (1) reduction or disappearance of adverse effects or medical treatments; (2) reduction of functional limitations and increase of physical activity13 14; (3) reduction of emotional difficulties. By influencing these aspects, bariatric surgery can also impact family, friendship and sexual relationship dynamics.15–17
However, social dimensions are not integrated into quality of life measurement tools, but are designed as distinct variables impacted by quality of life18–20 or impacting it themselves.21–23 Social variables are therefore not completely absent from studies on the health impact of bariatric surgery (or on the predictors of its success on an anthropometric level in terms of weight loss or lowering of body mass index (BMI)). Nevertheless, sociological approaches to the latter remain rare. They aim to shed light on the processes involved in the maintenance or evolution of lifestyle habits following surgery, rather than measuring the positive or negative effects of the operation on health within the broader spectrum of quality of life. These sociological processes are very different from psychological predictors. They involve taking into account the influence of living environments and social interactions on individual experiences.
Living environment, social participation and stigmatisation
Studies on the impact of social representations of obesity and the use of surgery show that it is a means of escaping discrimination in educational environments,24 25 work26 27 and sex life.28 However, the use of bariatric surgery runs the risk of confirming the weakness of character often considered to be at the root of obesity29 30 and contributes to stigmatisation on the part of health professionals themselves.31 32 Verhaak et al33 show that, when weight-related biases are internalised, they affect the clinical attrition of patients engaged in a medicalised path to weight loss. A recent literature review on the stigma of bariatric surgery34 points out the methodological shortcomings of existing studies, all of which were carried out in the general population or with health professionals. The authors regret the failure to take into account the patient’s point of view when studying the effects of surgery and the exploration of the sociocultural foundations of its stigmatisation. To compensate for this lack of data, they propose a comparative survey (the results of which are not yet available) between the Netherlands, France and the UK, questioning people who have undergone surgery, as well as health professionals and the general public.35
Supporting the evolution of lifestyle habits in the face of uncertainty
The effects of prejudice and stigmatisation of bariatric surgery are investigated in the few sociological4 30 36 37 or psychology studies38 examining the social experience of post-surgery body modifications. This experience is marked by a disruption in lifestyle habits, in terms of food intake and hydration, but also in the practice of physical activity.14 After a few weeks or months, the gradual experimentation of increased mobility abilities sometimes produces the feeling of being ‘un-disabled’.39 The rapid weight loss is then often referred to as a ‘rebirth’.40 41 In some cases, identity reconfigurations associated with body changes are described as being more traumatic. Working on oneself is then necessary in order to find a medical,4 aesthetic37 or moral30 meaning to the changes experienced. This work of appropriating one’s ‘new’ body is done under the public eye, by being confronted with the fears to which social interactions expose. All these elements are not included in quantitative studies that seek to assess the impact of surgery on social interactions, based on the comparison of questionnaires administered before and after the operation.42 These descriptive approaches struggle to grasp the processes behind the changes measured, or how they can affect lifestyle habits. However, while bariatric surgery affects social participation and any attempt to adopt new lifestyle habits,43–45 its long-term effectiveness depends on lasting changes to these habits.22
Social dynamics of lifestyle change and medium-term impact
Social processes follow temporal dynamics. A few months after surgery, when their weight stabilises, the patients who have undergone surgery often find that the amount lost is insufficient.40 41 Over time, regaining weight can also occur.46 In addition to the threat to their attained silhouette,47–49 there is also the risk of losing the social relationships established as a result of weight loss—particularly in relationships of seduction.50 In this situation, social pressure is strong, as is the fear of returning to a ‘fat’ body, a stigma associated with a lack of self-control.30
Bariatric surgery produces multiple and variable effects on the body, as it is perceived over the weeks and months following the operation, and involves managing these effects within the social environments (family, medical, professional) frequented. The rare sociological studies that have studied the articulation of these elements used qualitative data from the retrospective narratives of a small number of patients recruited in a single hospital,4 23 39 or repeated interviews within a timeframe not exceeding 12 months after the operation.30 36
Longitudinal approaches that include more patients and which repeat measurements over time focus on the impact of bariatric surgery on mental health or quality of life in the medium term,51 psychological predictors (mental health, eating disorders) of the success of the surgery,52 or the effects of feelings of self-efficacy and health competence on changes in post-surgery quality of life.53 54 When, exceptionally, a study focuses on the evolution of behaviours, medical and psychological variables remain decisive. The examination of physical activity (as it promotes weight loss, health and quality of life) leads to the observation that none of the psychological determinants measured (pleasure, self-efficacy, social support) explain the level of physical practice.55
Study aims and hypothesis
This article details the protocol of the ChiBarAPS study, which examines the evolution of physical and dietary practices in relation to the overall body experience, within the social environments frequented by the individual, over a period of 24 months after surgery. This protocol aims to shed light on the social factors that weigh on the reorganisation of lifestyle habits following the disruption caused by surgery. ChiBarAPS has three main objectives.
Objective 1
The first objective is to document the work undertaken by patients on themselves in order to identify and measure the evolutionary effects of surgery (bodily transformations, pain, discomfort, fatigue, etc), as well as to adapt to them (transformation of lifestyle, dietary, intake habits, etc).
Objective 2
The second objective is to provide information on the experience of the use of pre- and post-surgery information and support systems (medical devices and non-medical, associative or community networks), and to evaluate their effects on the agency of the people who have undergone surgery.
Objective 3
The third objective concerns the study of the evolution of the forms of social participation and lifestyle habits based on the Human Development Model-Disability Creation Process56 in order to identify processes for reducing situations of disability (eg, by improving physical capacities) or, on the contrary, social participation (due to pain, discomfort, stigma, etc).
The research is based on two hypotheses.
Hypothesis 1
The period of 6–24 months following surgery is a pivotal period, marked by a high degree of biographical uncertainty, during which the success or otherwise of escaping obesity in the longer term is at stake, depending on the ability of individuals to engage in work on themselves and to change their lifestyle in the long term.
Hypothesis 2
‘Escaping’ from obesity is not solely the symbolic passage below a certain weight threshold, but implies a transformation of oneself under the gaze of others, in particular to escape the stigma of obesity; a stigma that the use of surgery can reinforce despite weight loss.
Method
Theoretical approach
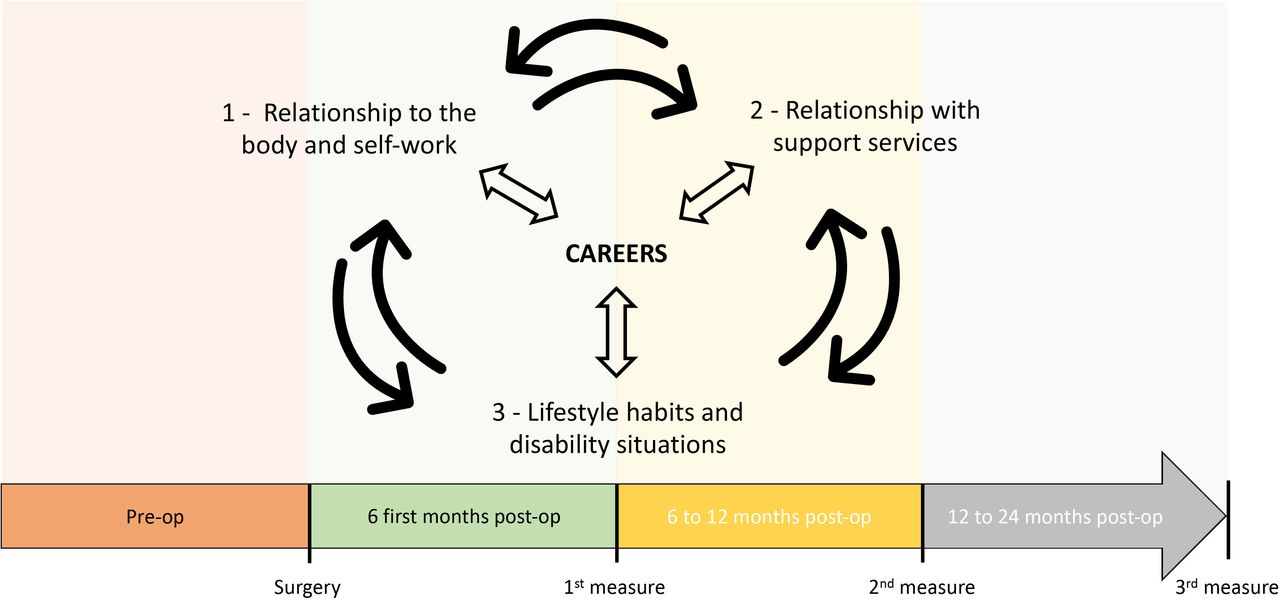
This research focuses on the transformations of the body, lifestyles and social practices (physical activities, diet, sexuality, body care, clothing, etc) following surgery. Post-surgery obesity is understood as a ‘combined in action’57 everyday work, that takes place in different environments (health, sports, professional, family, etc). The sociological concept of career58 59 makes it possible to articulate, based on attention to the different forms of work that the individual deploys, the three objectives mentioned above. It is thus the dynamics of the interactions between the three dimensions associated with these objectives (self-perception, experience of information and support systems, social participation) that should make it possible to model the evolution of careers related to obesity (figure 1). By focusing on the relationships that individuals establish with their social environments, the concept of career aims here to shed light on the social conditions of the transformations identified or ‘the social space of the transformation of the self’.60

Theoretical frame of the ChiBarAPS study, France. Study of the evolution of interactions between three dimensions of the social experience of obesity, articulated through the sociological concept of career, in the 24 months following bariatric surgery.
Study population
The participants in this study have undergone a sleeve procedure, are in employment or of working age (excluding students and retirees), and do not have an illness involving too heavy a treatment likely to have a strong impact on their post-surgery life experience (eg, cancer, multiple sclerosis, Parkinson’s disease). Participants were recruited from within the active lists of the study’s partner hospital departments with the aim of achieving the greatest possible diversity in terms of gender, social origin, preoperative and postoperative weight trajectory, etc. Attention was paid to the recruitment of men, who are not well represented in studies on bariatric surgery. In the event that these sampling diversity objectives were not achieved, recruitment could occasionally take place through patient associations or social networks.
Design of the study
ChiBarAPS is a multicentre longitudinal study conducted by sociologist researchers from Montpellier, Toulouse, Lyon 1, Lorraine, Paris Sorbonne and Saint-Etienne universities, comprising three components: qualitative, quantitative, literature and data review.
The qualitative component of the study aims to carry out semi-structured interviews of the life story and practice type, repeated at 6, 12 and 24 months after surgery with 30 patients. The relationship of trust established by the sociologist and post-doctoral fellow, over the course of these meetings, should make it possible to document several dimensions presented to participants at the beginning of the first interview. Namely, these are the bodily experience (objective 1), the interactions with the actors of the specialised services (objective 2), as well as lifestyle habits (objective 3) during this pivotal period of the first 2 years post-surgery. Recruitment is carried out in partnership with the bariatric surgery departments of the public hospitals of Montpellier, Toulouse and Lyon. It began in May 2024 and will end in March 2026.
The quantitative component, using questionnaires, targets a minimum of 200 patients, recruited 6 months after surgery and recontacted at 12, then 24 months. This part of the study involves the same partners as for the qualitative study, with the addition of clinics from the same cities, as well as public and private partners from other French cities such as Pau, Bayonne, Dax, Nancy, Rennes, Reims and Paris (which vary in size, territorial location and proximity to the rural world). The minimal number of participants does not correspond to a calculation of representativeness. It is the result of discussions with partner services to estimate the minimum number of participants who can be expected to take part three times, based on their active files, which represent around 25% of the latter over the recruitment period. Initiated 12 months after the start of the qualitative component, it will run from May 2025 to March 2027.
In parallel, a review of the literature and existing databases was undertaken during the first year of the project. The systematic review of the literature on bariatric surgery and the theoretical currents and notions used (see “theoretical approach” section) led to the design of the interview guide and a first version of the questionnaire. The latter will need to be complemented by the analysis of the 6-month interviews, a review of existing quantitative databases on obesity (in order to include a certain number of items for comparative purposes) and a test phase. Figure 2 shows how the different components of the study interact.

Flowchart of the ChiBarAPS study, France. Sociological study of post-bariatric surgery biographical uncertainties (6–24 months) through the prism of changes in bodily practices.
Data collection
Systematic reviews of literature and available data are a crucial step in refining our data collection tools. An equation was applied to various bibliographic search engines such as Isidore, Cairn, Psycinfo, Cochrane, Open Edition, Érudit: (Obesit* OR Fat bod* OR Overweight OR Fat) AND (Bariatric* OR Gastrectom* OR Bypass*). Then, it has been adjusted for Jstor and PubMed to rule out the many results that were not related to bariatric surgery—Jstor: (Obesit* OR Overweight OR Fat) AND (Bariatric* OR Gastrectom* OR Bypass*); PubMed: (post OR after) AND (Bariatric* OR Gastrectom* OR Bypass*) AND (soci* NOT card*). It identified 8300 articles. A sorting by title and abstracts then led to the elimination of articles unrelated to the social dimensions of bariatric surgery, reducing the number of references under consideration to 288. This systematic review of the literature, which is mainly composed of works from the medical field, was finally supplemented by publications developing the sociological theoretical frameworks associated with the research suggested by the sociologists involved in the project.
A second review of existing databases is currently in progress, encompassing national portals (such as the French Open Data Portal and DataIned) and international portals (such as Jstor and PubMed), in addition to medical databases (SNDS) and academic databases (CENHTOR), including the Quêtelet-Progedo-Diffusion network specialising in social sciences. To conduct this research, we performed a lexicometric analysis using text processing software and a vocabulary distribution analysis61 based on the literature review. This process revealed a total of 22 keywords of interest for our study. After testing these keywords on data platforms, we selected five (BMI, Obesity, Health, Disability, Lifestyle Habits) that allowed us to target relevant studies for our research. These five keywords were applied across all existing data platforms to achieve a comprehensive review. Filtering measures were employed to avoid biases related to excessively outdated data or deviations from the relevant disciplinary field. The objective was to target variables corresponding to our primary research domains, namely obesity, disability, health, dietary consumption, bodily transformations, lifestyle habits and social participation. For each of the selected studies, we additionally recorded the emerging sociodemographic data. We then downloaded datasets and variables pertinent to our study objectives, which informed the construction of our questionnaire and served to archive questions that will be used for comparative purposes with our results. This exhaustive review has three objectives: (1) to identify completed or ongoing quantitative studies on the subject, (2) to collect existing databases in anticipation of weighting issues and sample comparisons during analysis phases and (3) to draw inspiration from the formulations and structures of questions and responses from repeatedly administered questionnaires to document changes in lifestyle habits. The design of the interview guide and questionnaire was partly inspired by the ongoing systematic review of the literature and partly by the theoretical approach used under the supervision of four researchers from the team. The questionnaire was also refined based on data from the initial interviews and the database review. The literature review, the database review and the initial results from the interviews served as sources of inspiration during the questionnaire design phase, but their integration was not part of a formalised protocol. The focus here is more on showing that the reviews were conducted primarily to support the development of the methodological tools for data collection rather than for their analytical potential.
Qualitative interviews, lasting approximately 2 hours, are conducted with patients who have consented to participate in a study introduced by members of the partner services during a post-surgical medical consultation. The recruitment ends as soon as 10 people have been accepted to participate per partner centre. They take place in a location of the patient’s choice, in order to minimise the constraints on discourse production, and are fully recorded. Participants are contacted by telephone at 12 and 24 months after surgery for the second and third interviews.
The questionnaires, each approximately 30 min in length, are administered to a new sample of 200 individuals, 1 year after the initial interviews, over a 6-month period for each assessment phase (+6, +12 and +24 months). The inclusion criteria for participants are consistent with those used in the qualitative study. The sample size was determined based on (1) the representativeness proportion relative to the total number of surgeries conducted over 6 months in France and (2) the practical feasibility of recruiting participants through our partner hospital and clinical services. One week prior to their 6-month postoperative follow-up appointment, patients receive a detailed email invitation, including an informed consent form, to participate in the online questionnaire. If patients have not participated prior to their appointment, assistance is offered, including an in-person meeting or phone support, to facilitate their participation and bridge the digital divide. Following the initial questionnaire at 6 months, participants are invited via email to complete follow-up questionnaires at 12 and 24 months. Non-respondents are contacted to assess their need for support or to document the reasons for their potential withdrawal from the study.
Analysis
This research project is structured in several work packages, four operational and four analytical ones (see figure 3). Among the operational packages, one is devoted to the organisation of meetings and working groups, another to ethical and regulatory approaches, as well as to the literature review (see dedicated section). The other two focus, respectively, on the constitution of qualitative and quantitative data corpora (including database analysis).

{kind=link}
{kind=link}
{kind=link}
Study framework on work packages, ChiBarAPS Study, France. Study of the evolution of interactions between three dimensions of the social experience of obesity, articulated through the sociological concept of career, in the 24 months following bariatric surgery.
The scientific references and the results of the qualitative and quantitative components are then analysed in three working groups, one for each objective of the project, namely: (1) experience of bodily transformations, (2) interactions with care structures, associations or peers, (3) lifestyle habits. These are thematic entries aimed at exploring all types of data (literature, transcribed interviews, cleaned databases) to shed light on a specific research axis. Finally, a fourth work package is responsible for carrying out a cross-sectional analysis of the three axes and disseminating the results. It aims to link and ensure coherence between the interpretations and analyses carried out for the different axes.
Once fully transcribed, the interview data is analysed according to the principles of Grounded Theory,62 in an inductive manner. Individual summary sheets are produced. They will make it possible to readjust the interview grids between the different meetings (6, 12, 24 months) and to carry out case-by-case analyses. At the same time, a transversal thematic analysis grid will record all the verbatim by axis and thematic sub-axes. A first grid will be established, based on the analysis of one case, then completed and reorganised within the framework of collective exchanges between the ten researchers involved in the other cases. Once this grid has been stabilised, the entire corpus of interviews will be coded by the post-doctoral fellow under the supervision of at least one of the ten researchers using the Maxqda software made available by the Humanum Digital Research Infrastructure (a support platform for human and social sciences supported by the French Ministry of Higher Education and Research). The quantitative data will be analysed using the copyright-free statistical software R. This analysis will be carried out per axis within the working groups, then pooled and discussed during wider meetings two times per year.
Each year, during the 48 months of the project, two workshop days will unite all the researchers involved in the study to discuss the data, its analysis and the challenges of presenting and disseminating the results. These workshops will also include external researchers working on related subjects, but also non-academic partners who are experts in the issues addressed (health professionals, representatives of associations and patients).
Patient and public involvement
Patients are involved on several levels. First, in the context of the interviews, by asking for their opinion on the items to be included in the questionnaire for the quantitative part of the study. In addition, interested patients are also invited to participate in the 2 days organised each year, with their travel expenses covered. Finally, they are asked to participate in the design and dissemination of research results for future patients and their families.
Ethics and dissemination
Ethical approvals and consent collection
The protocol of this study was deemed to comply with MR004 by the data protection officer of the University of Montpellier and approved by the ethics committee of the same university (n°UM2024-037). The research is funded for a period of 4 years by the French National Research Agency (n°ANR-23-CE41-0020-01).
Data protection information is presented to the participants, as well as their rights in terms of access, rectification, erasure or limitation of the information collected, or its portability, in accordance with the Data Protection Act and the European regulations for data protection. An information leaflet is provided to each participant by their doctor during the contact phase. It is signed before the interview, or read and approved before the questionnaire. Each participant is also reminded of the non-compulsory nature of participation, the absence of transfer of personal data to doctors or impact on their follow-up, as well as the absence of remuneration for participation. Participation is, however, facilitated by the fact that the interviewer comes to them, thus limiting any inconvenience.
Data processing and analysis
Data management is governed by a data management plan validated by the University of Montpellier’s referent on data protection issues. Specifically, this plan provides: (1) the transcription of data based on the Whisper software made available by Humanum-Progedo, (2) the pseudonymisation and anonymisation of the data, (3) its storage on the Sharedocs server made available by Humanum (digital research infrastructure under the supervision of the French Ministry of Higher Education and Research), to which only researchers involved in data analysis have access, through individual accounts. The questionnaire collects, by design, anonymised information.
Dissemination
The pseudonymised and anonymised data will be used in a certain number of oral communications at conferences and within articles in journals specialising in sociology or medical health. Material vectors for the dissemination of the study results will be produced for patients and care professionals, with the help of some of the latter in order to produce content that is both adapted and accessible to the target populations. Once the main analyses have been carried out, the quantitative database will be made available to the scientific community on the Quêtelet-Progedo-Diffusion platform, in accordance with the principles of open science.
The project will lead to the production of an awareness guide on the issues of long-term follow-up and monitoring of people who have undergone surgery, which will be aimed primarily at patients and their families. This guide will present meaningful indicators to identify key moments in post-surgical development and will propose resources or possible support systems to deal with the difficulties and obstacles encountered in social environments. A book will also be produced for health professionals. It will be possible to use this as support material for the training of individuals responsible for assisting in the use of bariatric surgery. It will aim to disseminate the knowledge obtained concerning the processes that can hinder changes in lifestyle habits. This knowledge can be used to adjust existing postoperative information and support systems, or to consider new ones. Co-constructed with the study’s associative and hospital partners, this book will be promoted and disseminated in conjunction with them.
Discussion
The ChiBarAPS study analyses the transformations faced by people who have undergone bariatric surgery and their management during the 2 years following surgery. Funded by the French National Research Agency (n°ANR-23-CE41-0020-01), it has the particularity of adopting a sociological perspective and relying on a research protocol that is both multicentre, through mixed methods, and longitudinal.
For the time being, the vast majority of studies on the effects of bariatric surgery—whether qualitative or quantitative—focus on patients in a hospital centre. Multicentrism can shed light on variations related to post-operative support depending on the centre involved. However, it will be necessary to ensure that the study includes people who were operated on in centres with very different characteristics (eg, public/private, integrated obesity centre/surgery department, large city/medium-sized city, etc), as well as being attentive to the diversity of the interindividual characteristics of the people operated on (eg, gender, level of education, social origin, rural/urban, etc).
The choice of a mixed research method should make it possible both to quantify and qualify the changes identified. Quantitative approaches dominate in bariatric surgery research. However, they sometimes struggle to go beyond a descriptive reading to identify the sequence of events and processes underlying the transformations observed. Qualitative methods can, in this instance, help to identify processes that are difficult to objectify. The back and forth between the two parts of the study should help to overcome the limitations of the two approaches taken separately. Concerning the interview approach, 30 people constitute a large cohort regarding other similar studies and the capacity of the recruited person to carry out this work. Particular attention should be paid to building and maintaining relationships of trust so as not to lose individuals over the course of the interviews. Another challenge will be related to the ability to adjust the interview grids from one meeting to the next, in order to renew the questions in a way that is adapted to each individual.
This leads us to the third specificity of the study, its longitudinal dimension. No qualitative study on bariatric surgery has so far offered repeated interviews over such a long period, up to 24 months after the operation, in a longitudinal (and not retrospective) perspective. Longitudinal follow-up of cohorts using quantitative approaches, on the other hand, is common. However, the approaches deployed are often very descriptive and aim, through a before/after comparison, to measure the impact of surgery on quality of life (in the more or less long term) or to identify psychological predictors of the surgery’s success. Oriented by their evaluative purposes, these medical or medico-psychological studies struggle to penetrate the understanding of the social processes underlying the statistical links identified.
The last particularity of the study is linked to its theoretical anchoring, which leads it to go beyond the usual questions concerning the surgery technique and its anthropometric, physiological and psychological effects, to introduce hypotheses stemming from the fields of sociology of the body, health and disability. The approach adopted here places the individual at the centre of the analysis, without seeking to make the postoperative experience a means of evaluating his or her success or failure. Beyond measurable or perceived changes (weight, side effects, etc), it will be a question of looking at the social interactions of individuals within the care structures as well as in their daily environments, paying close attention to the effects of these interactions on lifestyle habits and social participation. These interactions will thus be apprehended both in terms of bodily transformations (objectified by measurement indicators used in other studies, but also considered as they are subjectively felt by the patient) and the support of the care team that can contribute to giving them meaning.
We believe that these different components of the protocol, and the unprecedented results it will bring by shedding light on the situations experienced by individuals, will be equally of interest to sociologists and to the hospital doctors, associations and expert patients who are partners in the project.
Ethics statements
Patient consent for publication
References
Footnotes
Collaborators Study Group: Mathieu Baron, Yan Beldame, Anne Coquereau, Dominique Delaunay, Ute Duranteau, Lucie Favre, Laurène Fituque, Franshelis Garcia, Renaud Gontier, Sophie Garnier, Matthieu Hournau, Anne Marcellini, Marius Matichescu, Yves Morales, David Nocca, Laurent Paccaud, Éric Perera, Mélanie Perez, Simona Petracovschi, Théo Rougnant, Aurélie Savart, Marta Silvestri, Adrien Sterkers, Marie-Alix Thébault, Kirsten Verkooijen.
Contributors As the guarantor of the study, SF designed the research protocol. SF and CB-M wrote this paper. LC-P and PT participated in reviewing the text. All the authors reviewed and contributed to the final version of the manuscript.
Funding The study was supported by the French National Research Agency (ANR-23-CE41-0020-01).
Competing interests SF, PT, CC, DI, M-PJ, CP, ED and YM declared being involved in the presented research, and as such, their research unit received part of the funding granted by the National Research Agency (ANR). LC-P and CB-M declared being salaried respectively by the Universities of Toulouse and Montpellier, through the ChiBarAPS funding obtained from the ANR. PR and ED declared being heads of hospital departments partnering in the project, which received funding to support the recruitment of study participants. J-MO, declared as head of the Integrative Center of Obesity at the Pitié-Salpêtrière Hospital in Paris, is the coordinator of another ANR-funded research program running from 2024 to 2027. He is also a member of the interface committee on osteoarticular diseases and sits on the board of the research group on sport and physical activity at the French National Center for Scientific Research (CNRS).
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.