Article Text

Abstract
Objectives Identifying the barriers and facilitators for Chadian youth (aged 15–24 years) along the pathway of access to HIV information and health services.
Study design Qualitative descriptive study.
Study setting The study was conducted in N’Djamena, Chad, with 20 high schools purposefully selected based on participation in a Blue Cross Chad (BCC) peer-to-peer education programme.
Participants A total of four focus groups, each consisting of 12 participants, stratified by gender and BCC programme participation (two each among participating and non-participating high schools), were conducted.
Methods A descriptive qualitative study using thematic analysis of content was conducted. The qualitative software ATLAS.ti V.22 was used to organise and code the data.
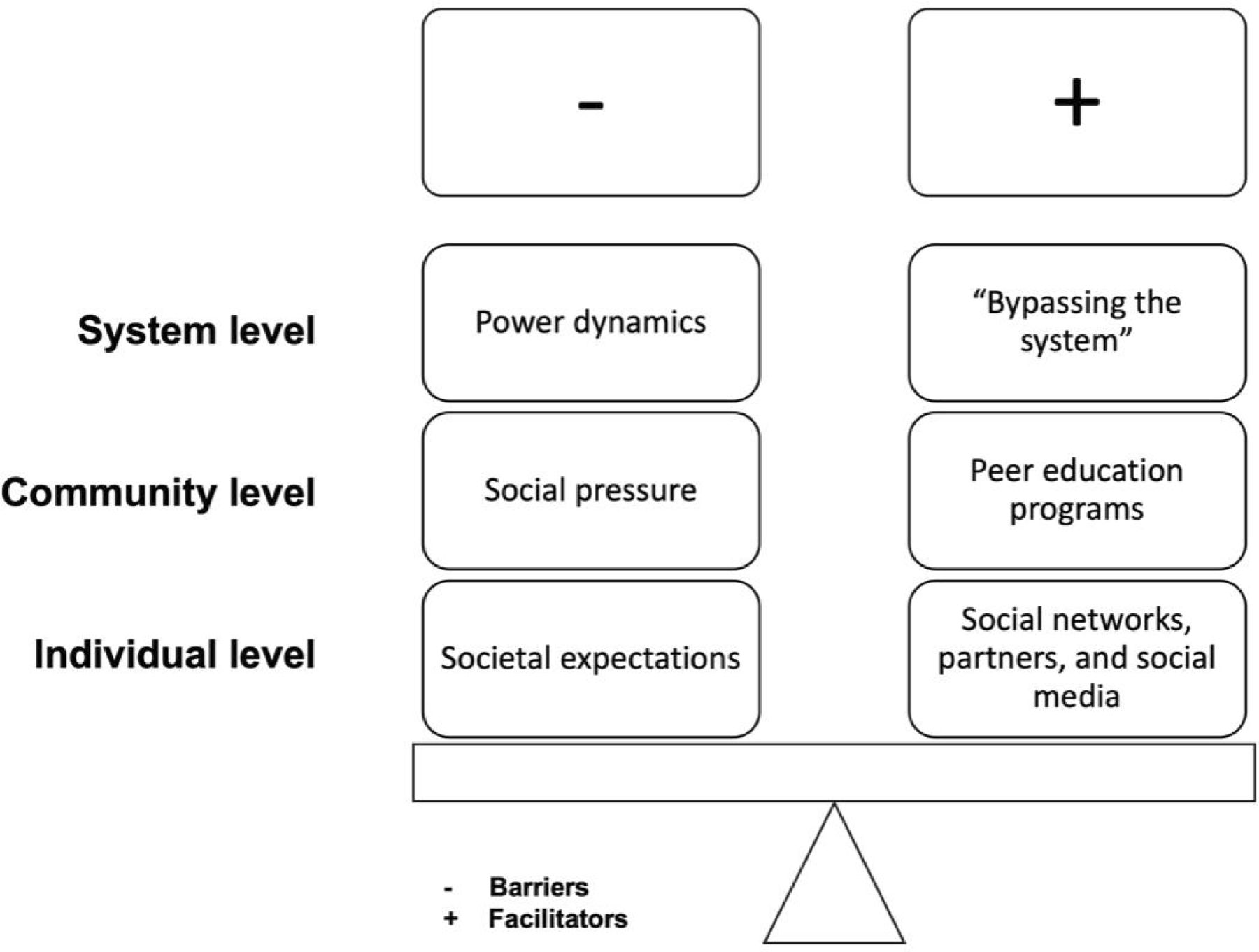
Results Five main categories of barriers and facilitators for HIV information and health services were identified, including (1) societal expectations and norms; (2) power dynamics; (3) social networks; (4) peer-education programmes; and (5) bypassing the system. Barriers and facilitators to information information-seeking and access to health services were observed at individual, community and system levels. High school students expressed that access to information and health services were important when it comes to HIV and AIDS prevention and treatment. Societal expectations and power dynamics were identified as key barriers, while trust through social networks and peer-education programmes were key facilitators to accessing information and health services.
Conclusion This study allowed for the identification of both barriers and facilitators of HIV information and health-seeking in the context of N’Djamena, Chad. Our findings highlight the importance of comprehensive community- and youth-led approaches that are youth-friendly and youth-centric and are needed to effectively communicate HIV information.
- Public health
- Adolescents
- HIV & AIDS
- PREVENTIVE MEDICINE
- Sexually Transmitted Disease
- Health policy
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The study employed locally trained interviewers, which helped in enrich cultural insights and enhanced participant trust during data collection.
A rigorous sampling method was used to ensure a diverse representation of views.
The study design included both schools that participated and did not participate in the Blue Cross Chad peer-to-peer education programme which provided a comparative perspective that enriched the study findings.
The study could have benefitted from the inclusion of high-risk groups to enhance the generalisability of the study findings.
Introduction
There are an estimated 2.78 million children and adolescents living with HIV worldwide and approximately 88% reside in sub-Saharan Africa (SSA).1 Chad is one of Central Africa’s most affected countries by the HIV epidemic with an overall prevalence of 1.6%; it is estimated there are 12 000 young people 15–24 years of age living with HIV in Chad.1 2 However, in the country existing programmes, interventions have largely focused on prevention mother-to-child transmission), and HIV prevention efforts among adolescents and young people (aged 10–24 years) have been more limited.3
In 2012, Blue Cross Chad (BCC) launched the ‘Life Skills and Peer Education’ programme, also called the BCC Lifeskills Project (BCC life skills–based education (LBSE)) (2012–2016) targeting vulnerable school youths aged 14–18 years.4 5 This programme is rooted in the LBSE approach, which has been widely used in youth programmes by many organisations around the world, especially for HIV and AIDS education.6 While such programmes have shown effectiveness in reducing risk behaviours and improving knowledge and attitudes related to HIV, their effectiveness in SSA depends on various factors, such as programme design, cultural context and resource availability.7
The programme aimed to develop skills and knowledge to make informed decisions about alcohol, drug abuse and associated risks, including HIV transmission.5 The BCC LBSE included a wide range of stakeholders, including high school students, parents, community leaders, and local and national political and administrative authorities who play a key role in shaping an enabling environment for the development and implementation of the programme.4 The BCC LBSE was implemented in 15 high schools in N’Djamena from 2012 to 2016 and expanded to 20 high schools until 2021.4 8 Peer educators, trained in life skills lessons, taught topics ranging from HIV transmission to prevention.4 Lessons used a combination of teaching methodologies, including group work and role-play.4 While the BCC LBSE has undergone evaluations in 2016 and 2021, these evaluations mainly focused on its impact on reducing substance use and failed to provide insights into HIV sexual behaviours among youth.4 5
In this qualitative study, our primary goal was to evaluate contextual factors that influenced youth access to HIV information and health services in N’Djamena, Chad. We secondarily explored differences in the views of students from schools that participated and did not participate in the BCC LBSE programme. The insights gained from this research are intended to help shape the development of future community- and youth-led interventions for effective HIV prevention and treatment in Chad.
Methods
Study setting
The study was conducted in N’Djamena, the capital city of Chad and the most populous with an estimated 1.6 million people.9 It is composed of 10 districts (online supplemental file 1), and convenience sampling was applied as the study setting for this qualitative study as BCC has implemented its programme in 20 high schools in the city.8 Data from the UNICEF show that HIV prevalence among young women and men (aged 15–24 years) is 1.3% and 0.8%, respectively.3 When stratified, the prevalence among young women rises with age. For example, it is at 1.2% among women aged 15–19 years, 1.8% among 18–19 and 2.4% among 23–24.3 In the areas of prevention and medical care for paediatric HIV, only 22% of children living with HIV (aged 0–14 years) have access to retroviral treatment.3 With a median age of 17 years, 65% of the population is under 25 years of age.10 The fertility rate is 6.35 births per woman, and 70% of girls under 18 and 29% of those under 15 are married.9 11
Supplemental material
Study design and sampling
We conducted a conventional qualitative content analysis method to identify the roadblocks that face Chadian youth (aged 15–24 years) along the pathway of getting access to information and health services of HIV. A purposeful criterion sampling method was used to identify and select information-rich subjects for each group of interest, including BCC LBSE participating high schools versus non-participating high schools. Eligibility criteria for both groups included currently enrolled high school (9th to 12th grade) students. For students in participating high schools, eligibility criteria of programme participation in at least 6 months were implemented to ensure sufficient intervention exposure. In each high school, a list of currently enrolled students provided by the school registrar office was used. From these lists, students with missing information were removed. A total of 4 groups of 12 participants (figure 1) was formed. While focus group discussions (FGDs) often consist of 6–8 participants, our large group size (n=12) was chosen for diversity of perspectives and group dynamics. However, due to the exploratory nature of the study, saturation was not reached.

Flowchart of participants. BCC, Blue Cross Chad; HS, high schools.
FGDs were stratified by gender and whether or not the high school participated in the BCC programme to allow participants to feel comfortable sharing their beliefs. The first two groups (one male, one female) included in-classroom participating high school students, whereas the last two groups (one male, one female) included in-classroom non-participating high school students. After being identified by the BCC staff members, school administrators called parents of those under 18 years old and explained the purpose of the research. Following the call, parents who had agreed on the phone were invited to the school to sign the parental written consent. If they could not make it in person, they provided verbal consent. We used the COREQ checklist to guide the reporting of the qualitative methodology and study results (online supplemental file 2).10
Supplemental material
Data collection
For the qualitative study, six BCC staff members were used as interviewers, divided into two teams of three researchers, and each team was composed of at least one female interviewer. However, these six staff members were not involved in the BCC LBSE project in any way. Prior to the study, they were trained in qualitative research methods, including how to conduct interviews. Using locally trained interviewers was beneficial to the study as it helped facilitate entrance and acceptability among members of the community. Although the interviewers were from the same organisation whose programmes were intended to increase HIV prevention knowledge and service use, the ones chosen were not involved in the implementation of the intervention in the selected high schools.
FGDs were conducted by teams in French and Arabic, using a semistructured interview guide (online supplemental file 3). The interviews took place in a secure private location of the BCC headquarters. Participants in each FGD were asked to come during their scheduled time, and their transportation expenses were reimbursed (not exceeding US$10). These FGDs took between 90 and 120 min, and transcription of each FGD took approximately three to 4 hours. Each transcript was discussed with the entire team to ensure that all cultural nuances were captured.
Supplemental material
Participants were asked to describe their perceptions and beliefs on sexuality as it relates to HIV transmission and prevention. Discussions started with an explanation of the interview purpose, reassurance of confidentiality and seeking of respondents’ written or oral informed consent. Participating in this study had some risks, particularly due to the sensitive nature of the topics related to sexual and reproductive health (SRH) and HIV. Participants may have found some questions uncomfortable or difficult to answer, even though measures such as separating FGDs by gender have been implemented to create a safe space. Additionally, loss of confidentiality was a potential risk, but the research team took steps to safeguard privacy. All data were stored securely using Harvard Dropbox with multiple layers of protection, including encryption and private keys. Only the research team members had access to de-identified data, which were labelled using coded identifiers. However, the potential benefits of this research were significant. Insights from this study will contribute to the design, implementation, and scale-up of more effective, youth-centric and youth-friendly health interventions in Chad, ultimately improving access and outcomes for young people in the country. All FGDs were transcribed and translated by the entire team to ensure that the translations captured cultural nuances. All interviews were recorded and transcribed verbatim.
Data analysis
The qualitative analysis software ATLAS.ti V.22 was used to organise and code the data.12 The data were analysed using inductive thematic analysis, codifying and identifying the main emerging themes. Data analysis was carried out at the same time as data collection. During this process, each team member thoroughly read a subset of interviews and labelled each line with codes, resulting in 43 codes. These codes were examined for overlap and then collapsed into 12 broader codes. The codes were further organised into five overarching categories (table 1).
Sociodemographic characteristics of participants (n=48)
The research team used Lincoln and Guba’s evaluative criteria, which include credibility, transferability, dependability and confirmability.13 The texts associated with the codes were extracted and organised by category, and similarities and differences were compared. Since all interviewers were local and familiar with the region’s culture, they all participated in this process. Dependability was achieved through a validation of the coding tree by consensus among team members regarding the definitions and inclusion/exclusion of the codes. The documentation and archiving of all stages and documents of the research process, multiple revisions, and exchange of main and subcategories identified by the authors allowed to achieve confirmability.
Reflexivity
The qualitative research team (multidisciplinary, multilingual, multicultural and multinational) involved in the data collection (interviews) and analysis (transcription and translation) process minimised the presence of any research team member’s bias in the analysis. As the data collection team included locally trained interviewers, it captured cultural nuances, as well as facilitated entrance and acceptability among members of the community. In fact, this latter was reflexive and collaborative as we continuously engaged with the non-governmental organisation (NGO) partner, which informed school officials, government officials and development organisations. Despite the involvement of multiple team members in the processes, there may still be bias present in the conclusions reached. The process of triangulation was applied by sharing findings from the study with members of the community who were not interviewed, as well as individuals who are service providers or experts on the issue within the community. They may be able to identify inaccuracies or biases that the research team failed to recognise.
Ethical considerations
Ethical clearance was obtained from the Harvard T.H. Chan School of Public Health’s Institutional Review Board, protocol #IRB21-1641, and the National Committee on Bioethics of Chad #036CMT/PC/PMT/MESRI/SG/CNBT/2022. Informed consent forms were read aloud and signed by the interviewers prior to the start of the FGDs. Participants were also given opportunities during the consent process to ask any questions.
Patient and public involvement
Participants were not involved in the design, conduct, reporting, or dissemination plans of the study.
Results
A total of 48 in-classroom high school students were divided into 4 FGDs as follows: male beneficiary high school students (BM), female beneficiary high school students (BF), male non-beneficiary high school students (NBM) and female non-beneficiary high school students (NBF). The mean age of all participants was 16.75 years with variations between groups and across genders (table 2). Most participants were in the 10th and 11th grades representing 73% of the sample. The sociodemographic characteristics of the sample are presented in table 2.
Sociodemographic characteristics of participants (n=48)
The following categories were developed from analysing the interview transcripts: societal expectations, power dynamics, social networks, peer education programmes and bypassing the system. Based on the similarity in meaning, we organised and structured the categories into a conceptual framework (figure 2), outlining how identified barriers and facilitators support HIV and AIDS access to information-seeking and health services at different levels.

{kind=link}
{kind=link}
Barriers and facilitators to information-seeking and health services among the youth (aged 15–24) enrolled in high schools in N’Djamena, Chad.
Barriers and facilitators
High school students expressed access to information and health services as important factors of HIV prevention and treatment. We identified societal expectations and power dynamics as key barriers, while trust through social networks and peer-education programmes were key facilitators to information-seeking and health services. We described each of these barriers and facilitators by level in more detail below.
Barriers to information-seeking and health services
At the individual level: societal expectations and norms
Recognising the country’s sociopolitical context, societal expectations and norms were observed as major barriers to accessing both information and health services at the individual level.
Males in the beneficiary group mentioned that it ‘takes a lot to talk about sex’ and highlighted the importance of knowing ‘whom to talk with’ (BM, #8, 19 years). All groups mentioned that they were unable to freely speak about sex with their parents, shown by ‘although I can speak about sex with my friends and girlfriend, I am not able to speak about it with my parents’ (NBM, #30, 18 years). In addition to the topic being taboo, adolescents further explained that they assumed that by asking questions about sex, their parents would automatically assume that they are sexually active which was contrary to the highly encouraged practice of abstinence.
At the community level: social pressure
At the community level, fear and public shame prevailed. Females in the beneficiary group noted that ‘shame is what prevents people from getting the information they need’ (BF, #13, 17 years). This was also observed as a barrier when accessing care, exemplified by ‘the main reason that prevents us from going to health centres are shame and fear’ (NBF, #39, 17 years). Males and females in both the beneficiary and non-beneficiary groups further explained that this fear came from the fact that they did not want to be recognised by family members or friends as this would mean that they are sexually active. This was particularly relevant to the aspect of ‘tight-knit communities’ in which people know each other well. A quote exemplifying this phenomenon is presented below:
…The second reason is that we are scared to find one family member. This will mean that we are actively practicing sex and can be problematic for our families. (NBM, #33, 16 years)
At the system level: power dynamics
At the system level, adolescents perceived power dynamics were at play. Age and gender dynamics emerged. Females shared that they did not feel comfortable in hospitals as healthcare providers tend to be men, as exemplified by ‘the services should be led by women as they are better placed to deal with these issues’ (BF, #16, 16 years). On the contrary, males mentioned that female healthcare workers ‘would make fun’ of them when talking about sex and their health, which made them ‘uncomfortable’ (NBM, #33, 16 years). Finally, it was noted by the youth that healthcare providers were perceived to have authority, which led to a one-way provider-patient relationship. This latter did not create a conducive environment for the youth to seek care, as shown by ‘improvements can be made in the way healthcare workers welcome us as well as create a safe climate in the clinics’ (BM, #5, 16 years).
Facilitators to information-seeking and health services
At the individual level: social networks
Social networks, such as friends, were an important knowledge-sharing platform for the youth: ‘young people often talk about sex with their friends’ (BF, #21, 18 years). Non-programme beneficiaries relied more on social networks as they did not have sexual education available in schools. However, unlocking social networks was based on trust, as shown by ‘it’s a matter of trust, and so I can talk about it with friends that I trust’ (NBF, #41, 19 years). Although these discussions occurred between friends, there seemed to be preferences with the same gender; in other words, females were more comfortable speaking about sex with their female friends, as shown by ‘we easily talk about sex between girls’ (NBF, #40, 17 years), while males were more open to their peers as follows: ‘when we speak about sex with friends, we mostly speak about masturbation’ (NBM, #25, 16 years) and ‘although it is a topic that is private, guys like to gossip about what other people do’ (NBM, #26, 16 years). Despite some individuals’ reliance on social networks, some males and females, particularly in the non-beneficiary high schools, felt it was ‘shameful to talk about sex with friends’ (NBF, #42, 17 years); nevertheless, this confidentiality issue did not appear to be an issue when it was about speaking with partners, shown by ‘feel free to talk about contraception and sex with their partners’ (BF, #13, 17 years). In all groups, the youth mentioned being comfortable speaking about sex with their partners, especially when they were not knowledgeable. Finally, the youth relied on social media when they did not have access to the information they needed. This was explicitly discussed among non-beneficiary females who stated that ‘young women rely on social media to get information’ (BF, #15, 16 years). This was further supported by males in the non-beneficiary group as exemplified by ‘I get all the information from Facebook, Google, and WhatsApp’ (NBM, #30, 18 years).
At the community level: peer education programmes
At the community level, peer-education programmes, such as the BCC LBSE, were identified as an enablers. Among the programme beneficiaries, males mentioned that such programmes are beneficial because they provide knowledge about sex education and HIV. They further stated that ‘sexual education in schools is very beneficial for young people because it allows us to know the dangers that can be associated with practicing sex’ (BM, #10, 18 years). Moreover, beneficiary females shared that they give a chance to young women who are not proactive to learn and safely practice sex, characterised by ‘important for young women who ashamed to talk about sex’ (BF, #17, 16 years). When both non-beneficiary males and females were asked about the potential of having such programmes in their schools, they all agreed that their schools needed these programmes.
At the system level: bypassing the health system
At the system level, ‘bypassing the health system’ (a term noted by the participants) for both access to information and prevention and treatment was observed outside the family and health system. They shared that they preferred social clubs and NGOs instead of hospitals because the staff was more receptive and provided them with the information and health services they needed. This was illustrated by ‘we rely on associations, cultural centres, the Chadian Blue Cross, peer educators to obtain information’ (BM, #7, 17 years). Although condoms are distributed for free at hospitals, the youth mentioned that they preferred getting them from ‘street drug sellers or local shops’ (BF, #20, 15 years) than going to the hospital to either protect their identity from their families or avoid mistreatment at the point of care.
Discussion
In this qualitative study, we sought to assess the contextual factors and mechanisms that influence access to information and health services among youth (aged 15–24 years) in N’Djamena, Chad. We found that the youth heavily relied on their social networks to access information. This reliance on social networks, especially peer-to-peer networks, was mediated by gender, trust and partner relationships. Additionally, youth reported apprehension to seek care due to the quality of care received at the facility and the power dynamics exerted by healthcare providers. Our results are consistent with prior research that showed social networks and peer education were efficient mediums for HIV messaging.14 15 More specifically, its contribution to the existing literature lies in the fact that school-based HIV education was an opportunity for the youth to learn in a safe and enabling environment, as well as provide them with decision-making skills.15–17Furthermore, young people have suggested that these programmes should be incorporated into their school curriculum in Chad. Barriers identified in the study such as societal expectations and power dynamics were similar in other SSA countries.14 18–22 These findings, however, provide an opportunity to integrate HIV prevention into the needs expressed by study participants.
The results of the study suggest harnessing social networks for HIV interventions for youth shows promise. Our research highlighted the significance of social networks, such as friends and partners, in disseminating information and motivating youth to get tested for HIV. Notably, unlocking social networks appears to be influenced by gender-based factors. A systematic review by Fearon et al23 yielded inconclusive results regarding the impact of peers in adolescent sexual behaviour in SSA.23 However, peers were found to play a crucial role in influencing adolescent sexual behaviours within romantic relationships, as supported by numerous qualitative studies.23–27 A baseline assessment of an HIV prevention trial in Tanzania revealed that network structure, composition and norms were associated with HIV testing behaviour among urban Tanzanian men.28 Surprisingly, the study showed that men belonging to networks with a higher proportion of women were more likely to have tested for HIV, contrary to our findings.28 This composition effect was found to outweigh the influence of descriptive norms among closest friends.28 In another study in KwaZulu-Natal, Adeagbo et al29 demonstrated the effectiveness of friends in promoting HIV prevention.29 However, low pre-exposure prophylaxis uptake was attributed to doubts about the professional credibility of friends, as young people may not view them as genuine healthcare providers.29As a result, studies are needed in Chad to determine the best approaches to positively use social networks for HIV prevention efforts in the context.
As discussed by the youth, more specifically non-beneficiaries, social media was an integral part of their access to information. As the youth advocated for better promotion of existing health services available to them, social media appeared to bridge communication mediums. Bull et al30 conducted a cluster randomised control trial to determine whether STI prevention messages delivered via Facebook were efficacious in preventing increases in sexual behaviours at 2 and 6 months in American youth and young adults.30 31 This study found that the intervention increased condom use and the proportion of safe sex acts at the 2-month follow-up.30 31 Across the world, several government programmes have also used social media to promote safe sex behaviours and HIV prevention.30 31 For instance, the US Centers for Disease Control and Prevention has developed a social media toolkit to promote online sexual health campaigns using Facebook, Twitter and YouTube.32 As it relates to linkage to care, a systematic review and meta-analysis conducted by Cao et al33 showed that HIV testing uptake increased after social media interventions, which mostly used Facebook as a social media platform.33 Additionally, in the studies where social media interventions were participatory, HIV testing uptake was higher in the intervention arm than in the comparison arm.33 Despite the low internet penetration (17%) as well as the number of social media standing at 3% of the total population in 2021, Facebook (88%) and Twitter (10%) were the most used social media in Chad.34 35This growing popularity of social media provides an opportunity for HIV prevention information for youth via social media globally; however, it is important to meaningfully involve young people in delivering HIV prevention information and services, particularly considering the cultural context. For example, this could be done by training peers who are from the target population and have experience with both social media and community outreach, which would have great potential to expand coverage and reach.36
For many students, schools represented a safe and enabling environment, which can be used as a platform to deliver high-impact HIV education interventions. Kelly challenges the education sector (2000) by arguing that schools provide different levels where HIV/AIDS-related interventions are needed.37 This is particularly important in the context of Chad as our results suggested that young people may be engaged in sexual behaviours earlier than the targeted audience for BCC LBSE. Therefore, programmes such as BCC LBSE should not solely focus on high schools but should begin early in primary school since primary school-age children have not yet formed sexual behaviour patterns. Although schools have been identified as the preferred location for SRH education by students in our study, school-based HIV education is not included in the core education curriculum in Chad. In that context, the national education programme could formally integrate and scale up peer education programmes into the curriculum. However, the education sector cannot do it alone. This calls for a concerted effort between stakeholders, including civil society, donors, NGOs and United Nations (UN) agencies to collaborate with national authorities to build the education sector’s capacity to design, implement, monitor and evaluate life skills programme. In the past, the Ministry of Culture trained youth facilitators for their 45-min weekly cultural activities in public schools. Furthermore, the National AIDS Control Programme developed a life skills training module on HIV/AIDS and reproductive health intended for trainers of peer educators who implement HIV and AIDS activities.38 For them to be sustainable, there is a need to train and support teachers, as well as the need to provide resources to and support for peer educators.39 Therefore, if these efforts are aligned, and there is better collaboration between these national and international stakeholders, a nationwide curriculum can be developed. An example from Benin showed that the design of the curriculum was a collaboration between the Ministries of Education, Health and Family.40 In their article, Sturke et al41 recognised the crucial role of partnerships as they offer avenues for implementing comprehensive intervention programmes in schools, encompassing early detection and support for HIV, as well as addressing mental and neuropsychiatric concerns among adolescents.41 They further argued that these initiatives need to be integrated into primary healthcare and community-based services to ensure broad accessibility and impact.41
Despite having access to information, many young women did not feel encouraged to seek care. Furthermore, they preferred going to social clubs instead of hospitals. Providing private and hidden health services has been recommended by the youth, especially young women as a potential solution. In Zambia, FAWEZA has created safe (social) spaces to allow young girls to play games, engage in sports and receive technical skills training.42 Although creating such safe spaces would not completely solve the issue, making sure to hire a diverse staff, including young, and female health workers, and ensuring that they are routinely trained would address issues around discomfort and mistreatment. A study conducted by Aung et al43 showed that training staff in working with key populations and supporting clinic policies that promote confidentiality and informed decision-making by young people led to clinics being more sensitive and capable of providing appropriate youth-friendly services.43
In their recommendations, the youth advocated for the practice of abstinence to be further promoted in mass awareness campaigns. However, even as the sociocultural and religious contexts must be considered, reliance on abstinence has been largely discredited as an effective HIV prevention approach, particularly to the extent many young people have already engaged in sex by the time they are reached by messaging—which, as a result, may counterproductively promote shame rather than motivate communication.44 45 Furthermore, these abstinence-based programmes disproportionately affect women and girls.46 Due to conservative beliefs, religious leaders possess a special position that enables them to play a significant role in addressing HIV/AIDS, shaping societal norms, disseminating reliable information and exerting influence on public opinion.47 To that extent, religious leaders should be meaningfully involved in the design of these HIV prevention strategies. In Kenya, Maulana and colleagues showed that it is possible to engage Islamic communities in designing interventions to suit their cultural and religious context, making use of their own views and perceptions of risks.48
Limitation
This study included some limitations. Our study sample took place in high schools and, therefore, did not include youth outside the formal education system. This is important as those in the formal system only represent 18 to 30% of the population. Second, although the interviewers selected were not involved in the implementation of the intervention in the selected BCC high schools, their posture as adults may motivate more socially desirable responses among young people about HIV and sex. The last limitation is that our findings did not specifically target most at-risk groups, including youth sex workers, men who have sex with men, transgender people and those who use injection drugs. When considering the epidemic, understanding the crucial role that most at-risk groups play in the transmission of HIV is important. Not only do young people constitute a large percentage of most at-risk groups, but they also frequently have higher HIV infection rates within these groups.49
Conclusion
This study identified barriers and enablers that the Chadian youth face along the pathway of getting access to information and health services for HIV and AIDS. We identified societal expectations and power dynamics as key barriers, while trust through social networks as well as peer education programmes were key facilitators to information-seeking and health services. Our findings suggest there is potential for peer education programmes that integrate sexual health and HIV prevention, particularly leveraging social media platforms, to engage youth. Importantly, this work also highlighted the value of qualitative methods and the active involvement of youth in health services research. Youth insights may be crucial for designing future interventions that are not only effective but also culturally and contextually tailored to the needs and realities of young people in Chad.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the ethical clearance that was obtained from the Harvard T.H. Chan School of Public Health’s Institutional Review Board, protocol #IRB21-1641, and the National Committee on Bioethics of Chad #036CMT/PC/PMT/MESRI/SG/CNBT/2022. Informed consent forms were read aloud and signed by the interviewers prior to the start of the FGDs. Participants were also given opportunities during the consent process to ask any questions. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful for the collaboration and support from Blue Cross Chad from which this research originated. We thank the participants for their time and willingness to share their experiences with us.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors EB: conceptualisation, methodology, investigation, data curation, formal analysis, writing–original draft, writing–review and editing, funding acquisition, project administration, supervision, visualisation. NB: methodology, investigation, data curation. DS: writing–review and editing. CRS: conceptualisation, methodology, writing–review and editing. EB is the guarantor.
Funding The study received funding from the Rose Service-Learning Fellow at the Harvard T.H. Chan School of Public Health, and the Fostering Diversity in HIV Research Program, led by Massachusetts General Hospital and Harvard T.H. Chan School of Public Health. The Fostering Diversity in HIV Research Program is supported by the National Institutes of Health (R25MH119857).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.